
Early Effects of Nivolumab and Ipilimumab Combined Immunotherapy in the Treatment of Metastatic Melanoma in Poland: A Multicenter Experience

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Patient Characteristics
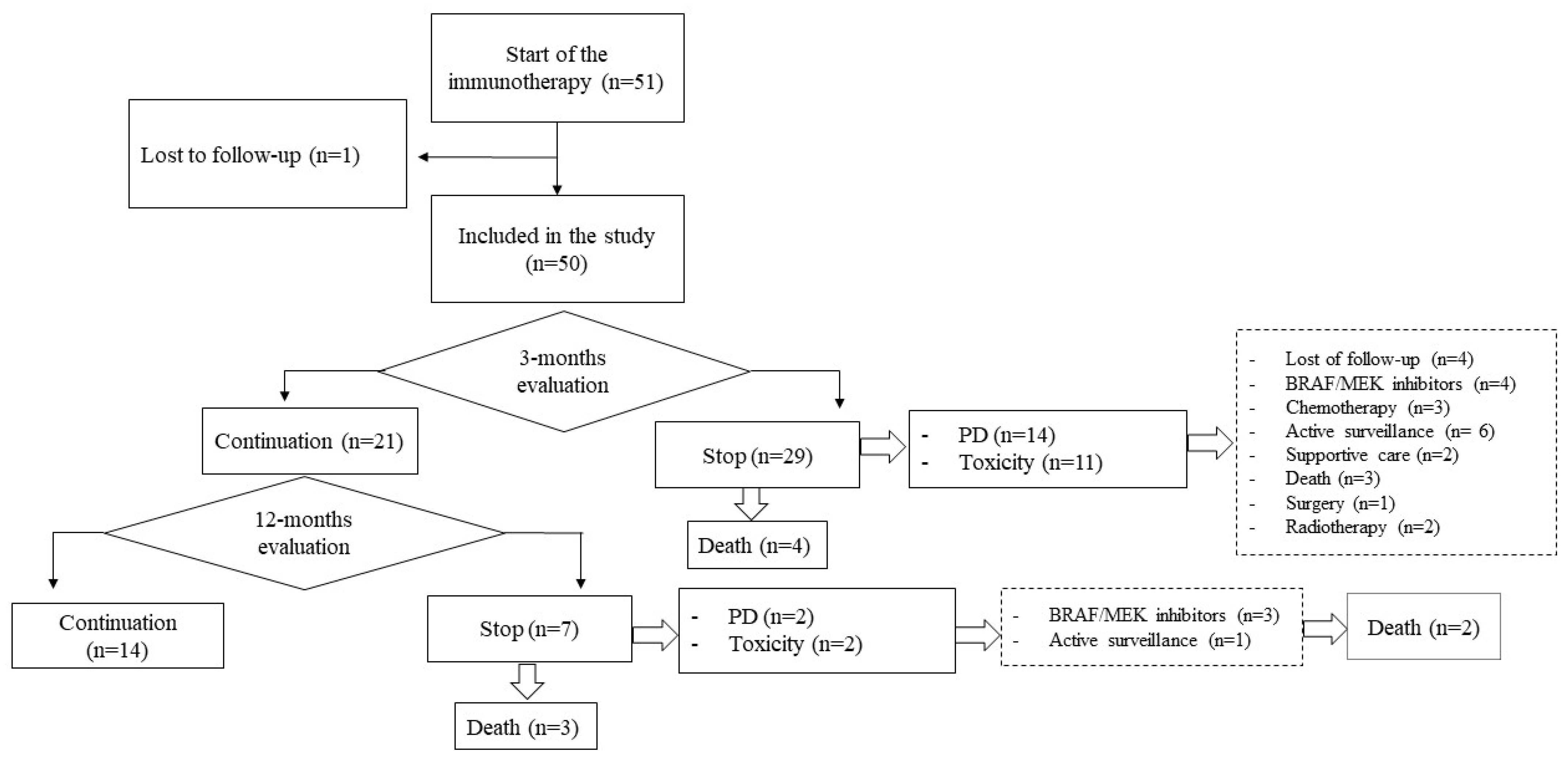
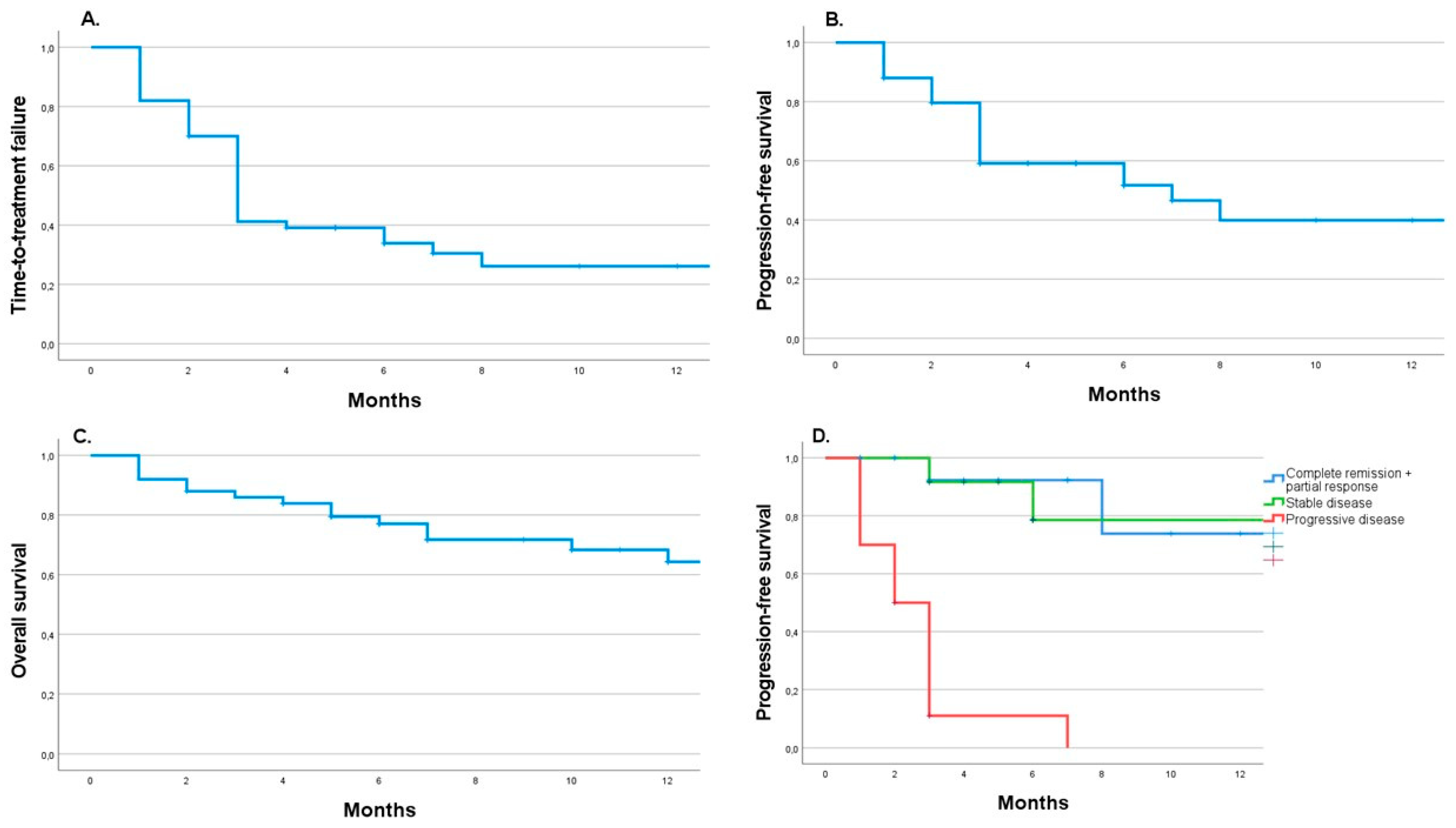
3.2. About 60% of Patients Recorded a Disease Control Rate after the Immunotherapy Induction Phase
3.3. Only 29% of Patients Continued Immunotherapy Till the 12-Month Checkpoint
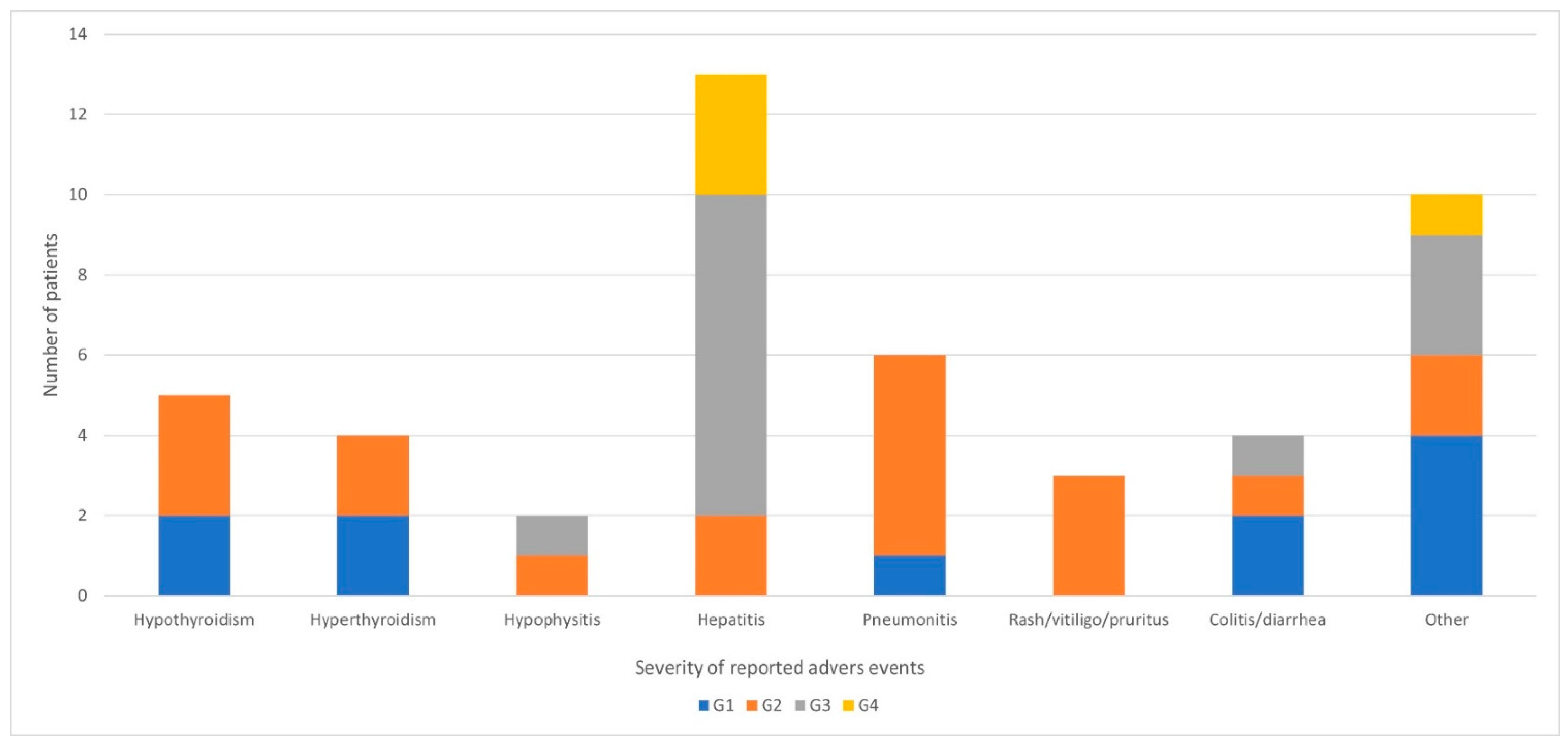
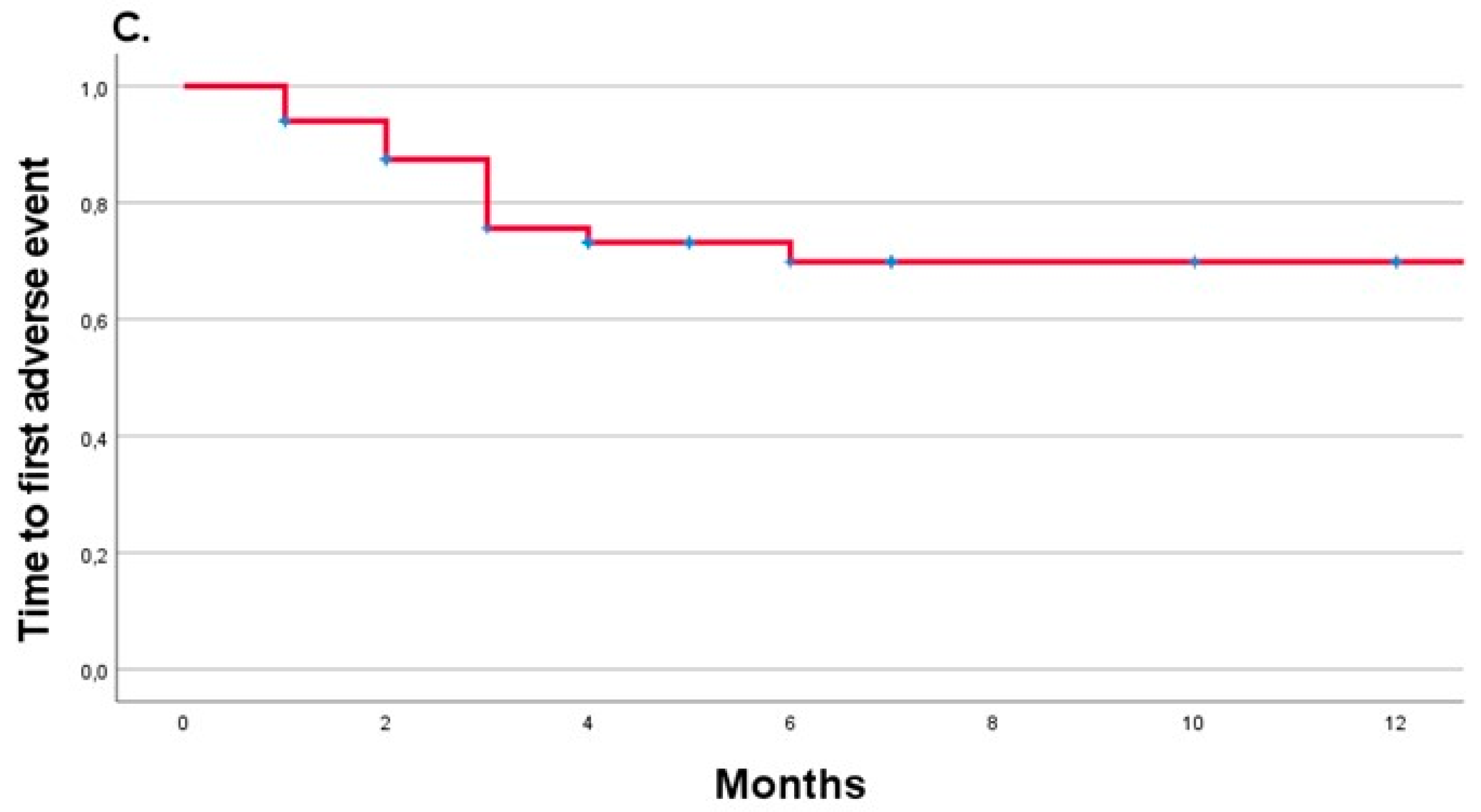
3.4. Hepatotoxicity, Pneumonitis, and Thyroid Gland Disturbances Were the Most Frequent Adverse Events Related to the Combined Immunotherapy
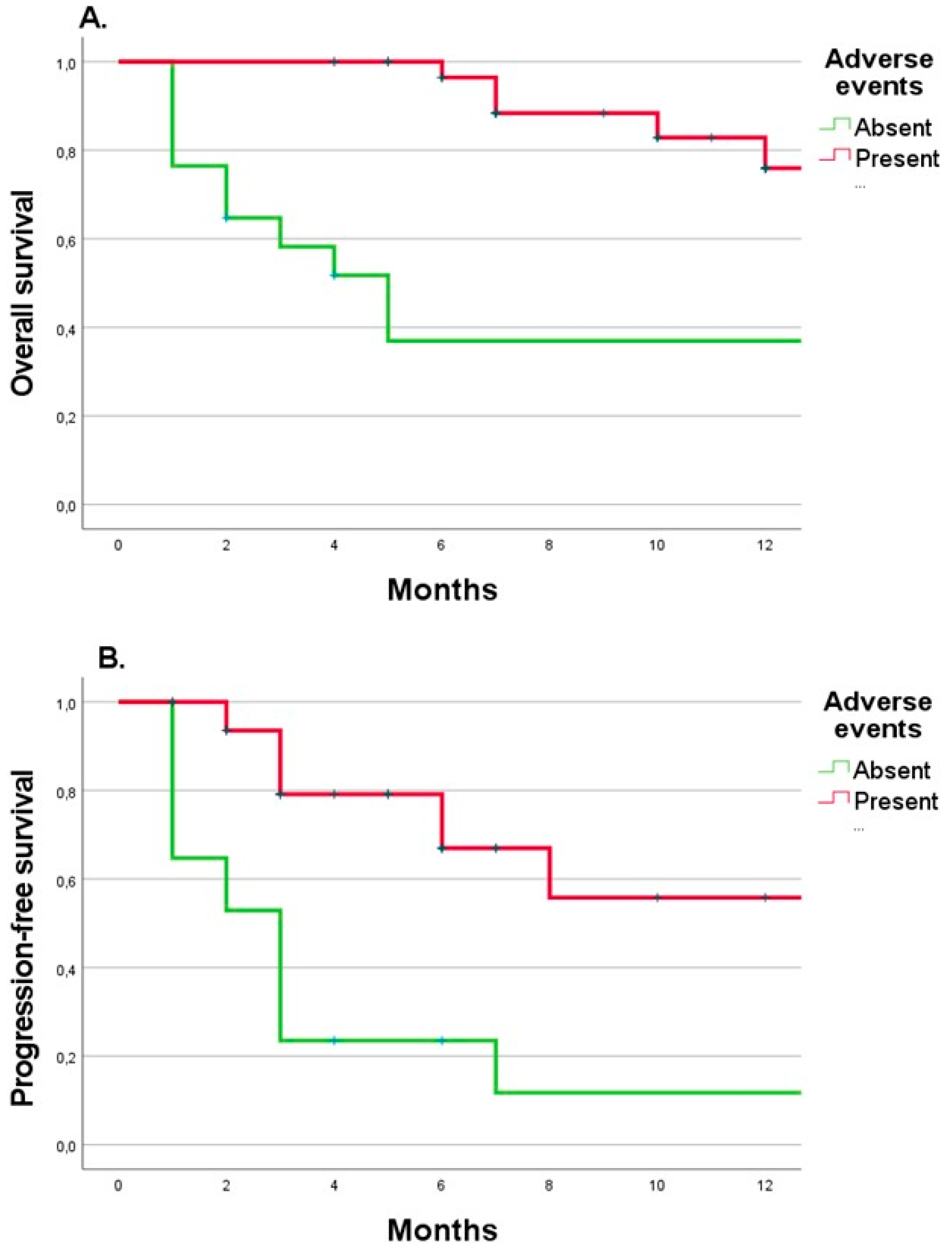
3.5. The Combined Immunotherapy Duration and Presence of Adverse Events Were Beneficial Predictors of the 12-Month Follow-Up Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Didkowska, J.; Wojciechowska, U.; Michałek, I.; Caetano dos Santos, F.; Olasek, P. Nowotwory Złośliwe W Polsce W 2019 Roku (Cancer in Poland in 2019). 2021. Available online: http://onkologia.org.pl/wp-content/uploads/Nowotwory_2019.pdf (accessed on 10 September 2022).
- Rutkowski, P.; Wysocki, P.J.; Kozak, K.; Nasierowska-guttmejer, A.; Jeziorski, A.; Wysocki, W.M.; Kalinka, E.; Świtaj, T.; Kamińska-winciorek, G.; Czarnecka, A.M.; et al. Postępowanie Diagnostyczno- -Terapeutyczne u Chorych Na Czerniaki—Zalecenia Ekspertów. Onkol. W Prakt. Klin. 2020, 16, 163–182. [Google Scholar] [CrossRef]
- Michielin, O.; Van Akkooi, A.C.J.; Ascierto, P.A.; Dummer, R.; Keilholz, U.; ESMO Guidelines Committee. Cutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1884–1901. [Google Scholar] [CrossRef] [Green Version]
- Dacarbazine-Summary of Product Characteristics. Available online: https://file.wuxuwang.com/hma/AT_H_0239_004_FinalSPC.pdf (accessed on 17 June 2022).
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; He, Z.; Wang, X.; Li, H.; Liu, X.-S. Antigen presentation and tumor immunogenicity in cancer immunotherapy response prediction. eLife 2019, 8, e49020. [Google Scholar] [CrossRef]
- Kirkwood, J.M.; Strawderman, M.H.; Ernstoff, M.S.; Smith, T.J.; Borden, E.C.; Blum, R.H. Interferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: The Eastern Cooperative Oncology Group Trial EST 1684. J. Clin. Oncol. 1996, 14, 7–17. [Google Scholar] [CrossRef]
- Atkins, M.B.; Kunkel, L.; Sznol, M.; Rosenberg, S.A. High-Dose Recombinant Interleukin-2 Therapy in Patients with Metastatic Melanoma: Long-Term Survival Update. Cancer J. Sci. Am. 2000, 6 (Suppl. 1), S11–S14. [Google Scholar]
- Atkins, M.B.; Lotze, M.T.; Dutcher, J.P.; Fisher, R.I.; Weiss, G.; Margolin, K.; Abrams, J.; Sznol, M.; Parkinson, D.; Hawkins, M.; et al. High-Dose Recombinant Interleukin 2 Therapy for Patients With Metastatic Melanoma: Analysis of 270 Patients Treated Between 1985 and 1993. J. Clin. Oncol. 1999, 17, 2105–2116. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Suciu, S.; Testori, A.; Santinami, M.; Kruit, W.H.; Marsden, J.; Punt, C.J.; Salès, F.; Dummer, R.; Robert, C.; et al. Long-Term Results of the Randomized Phase III Trial EORTC 18991 of Adjuvant Therapy With Pegylated Interferon Alfa-2b Versus Observation in Resected Stage III Melanoma. J. Clin. Oncol. 2012, 30, 3810–3818. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbé, C.; Bastholt, L.; Hamid, O.; Rutkowski, P.; et al. Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2017, 18, 611–622. [Google Scholar] [CrossRef]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Jr, W.H.M.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients With Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Puzanov, I.; Dummer, R.; Schachter, J.; Daud, A.; Schadendorf, D.; Blank, C.; Cranmer, L.; Robert, C.; Pavlick, A.; et al. Final overall survival for KEYNOTE-002: Pembrolizumab (pembro) versus investigator-choice chemotherapy (chemo) for ipilimumab (ipi)-refractory melanoma. Ann. Oncol. 2016, 27, vi379. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. CheckMate 067: 6.5-year outcomes in patients (pts) with advanced melanoma. J. Clin. Oncol. 2021, 39, 9506. [Google Scholar] [CrossRef]
- Wysocki, W.M.; Grela-Wojewoda, A.; Jankowski, M. Fallen dogmas—Recent advances in locoregionally advanced melanoma. Pol. Arch. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Choroby Onkologiczne-Ministerstwo Zdrowia-Portal Gov.Pl. Available online: https://www.gov.pl/web/zdrowie/choroby-onkologiczne (accessed on 16 June 2022).
- Melanoma-National Drug Program B59_(Od_09-2021). Available online: https://www.gov.pl/web/zdrowie/choroby-onkologiczne (accessed on 16 June 2022).
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- EMA Product Information: Ipilimumab. Available online: https://www.ema.europa.eu/en/documents/product-information/yervoy-epar-product-information_en.pdf (accessed on 13 December 2020).
- Nivolumab-Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (accessed on 16 June 2022).
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [Green Version]
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 19 March 2020).
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.; Peters, S.; Larkin, J.; Jordan, K. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv119–iv142. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Asher, N.; Ben-Betzalel, G.; Lev-Ari, S.; Shapira-Frommer, R.; Steinberg-Silman, Y.; Gochman, N.; Schachter, J.; Meirson, T.; Markel, G. Real World Outcomes of Ipilimumab and Nivolumab in Patients with Metastatic Melanoma. Cancers 2020, 12, 2329. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.C.; Chen, D.; Hu-Lieskovan, S.; Grossmann, K.F.; Patel, S.; Colonna, S.V.; Ying, J.; Hyngstrom, J.R. Real-world survival of patients with advanced BRAF V600 mutated melanoma treated with front-line BRAF/MEK inhibitors, anti-PD-1 antibodies, or nivolumab/ipilimumab. Cancer Med. 2019, 8, 7637–7643. [Google Scholar] [CrossRef] [Green Version]
- Maeda, T.; Hiura, A.; Uehara, J.; Toyoshima, R.; Nakagawa, T.; Yoshino, K. Real-world efficacy of nivolumab plus ipilimumab combination therapy versus nivolumab monotherapy for Stage IV melanoma patients in Asia. Eur. J. Dermatol. 2021, 31, 662–664. [Google Scholar] [CrossRef]
- Curtin, J.A.; Fridlyand, J.; Kageshita, T.; Patel, H.N.; Busam, K.J.; Kutzner, H.; Cho, K.-H.; Aiba, S.; Bröcker, E.-B.; LeBoit, P.E.; et al. Distinct Sets of Genetic Alterations in Melanoma. N. Engl. J. Med. 2005, 353, 2135–2147. [Google Scholar] [CrossRef]
- Furney, S.J.; Turajlic, S.; Stamp, G.; Thomas, J.M.; Hayes, A.; Strauss, D.; Gavrielides, M.; Xing, W.; Gore, M.; Larkin, J.; et al. The mutational burden of acral melanoma revealed by whole-genome sequencing and comparative analysis. Pigment Cell Melanoma Res. 2014, 27, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Freeman-Keller, M.; Kim, Y.; Cronin, H.; Richards, A.; Gibney, G.; Weber, J.S. Nivolumab in Resected and Unresectable Metastatic Melanoma: Characteristics of Immune-Related Adverse Events and Association with Outcomes. Clin. Cancer Res. 2016, 22, 886–894. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, A.M.M.; Kicinski, M.; Blank, C.U.; Mandala, M.; Long, G.; Atkinson, V.; Dalle, S.; Haydon, A.; Khattak, A.; Carlino, M.S.; et al. Association Between Immune-Related Adverse Events and Recurrence-Free Survival Among Patients With Stage III Melanoma Randomized to Receive Pembrolizumab or Placebo. JAMA Oncol. 2020, 6, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Maher, V.E.; Fernandes, L.L.; Weinstock, C.; Tang, S.; Agarwal, S.; Brave, M.; Ning, Y.-M.; Singh, H.; Suzman, D.; Xu, J.; et al. Analysis of the Association Between Adverse Events and Outcome in Patients Receiving a Programmed Death Protein 1 or Programmed Death Ligand 1 Antibody. J. Clin. Oncol. 2019, 37, 2730–2737. [Google Scholar] [CrossRef]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Prisciandaro, M.; Randon, G.; De Braud, F.; Del Vecchio, M. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic melanoma. J. Cancer Res. Clin. Oncol. 2018, 145, 511–521. [Google Scholar] [CrossRef]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [Green Version]
- Kooshkaki, O.; Derakhshani, A.; Hosseinkhani, N.; Torabi, M.; Safaei, S.; Brunetti, O.; Racanelli, V.; Silvestris, N.; Baradaran, B. Combination of Ipilimumab and Nivolumab in Cancers: From Clinical Practice to Ongoing Clinical Trials. Int. J. Mol. Sci. 2020, 21, 4427. [Google Scholar] [CrossRef]
- Xia, A.; Zhang, Y.; Xu, J.; Yin, T.; Lu, X.-J. T Cell Dysfunction in Cancer Immunity and Immunotherapy. Front. Immunol. 2019, 10, 1719. [Google Scholar] [CrossRef] [Green Version]
- Pasquali, S.; Hadjinicolaou, A.V.; Chiarion Sileni, V.; Rossi, C.R.; Mocellin, S. Systemic Treatments for Metastatic Cutaneous Melanoma. Cochrane Database Syst. Rev. 2018, 2, CD011123. [Google Scholar] [CrossRef]
- Cybulska-Stopa, B.; Pacholczak-Madej, R.; Kamińska-Winciorek, G.; Ziętek, M.; Czarnecka, A.M.; Piejko, K.; Galus, Ł.; Ziółkowska, B.; Kieszko, S.; Kempa-Kamińska, N.; et al. First-line treatment of advanced/metastatic melanoma with anti-PD-1 antibodies: Multicenter experience in Poland. Immunotherapy 2021, 13, 297–307. [Google Scholar] [CrossRef]
- Hribernik, N.; Boc, M.; Ocvirk, J.; Knez-Arbeiter, J.; Mesti, T.; Ignjatovic, M.; Rebersek, M. Retrospective analysis of treatment-naive Slovenian patients with metastatic melanoma treated with pembrolizumab—Real-world experience. Radiol. Oncol. 2020, 54, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Kuzmanovszki, D.; Kiss, N.; Tóth, B.; Kerner, T.; Tóth, V.; Szakonyi, J.; Lőrincz, K.; Hársing, J.; Imrédi, E.; Pfund, A.; et al. Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study. Biomedicines 2022, 10, 1737. [Google Scholar] [CrossRef] [PubMed]
- Arheden, A.; Skalenius, J.; Bjursten, S.; Stierner, U.; Ny, L.; Levin, M.; Jespersen, H. Real-world data on PD-1 inhibitor therapy in metastatic melanoma. Acta Oncol. 2019, 58, 962–966. [Google Scholar] [CrossRef]
- Pacholczak-Madej, R.; Grela-Wojewoda, A.; Lompart, J.; Żuchowska-Vogelgesang, B.; Ziobro, M. Effective Treatment of a Melanoma Patient with Hemophagocytic Lymphohistiocytosis after Nivolumab and Ipilimumab Combined Immunotherapy. Prague Med. Rep. 2022, 123, 35–42. [Google Scholar] [CrossRef]
- Teimouri, A.; Minard, L.V.; Scott, S.N.; Daniels, A.; Snow, S. Real-World Adherence to Toxicity Management Guidelines for Immune-Related Adverse Events. Curr. Oncol. 2022, 29, 3104–3117. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics, n = 50 | ||
|---|---|---|
| Demographics | ||
| Age | 57.5 (46–65) | |
| Males, n(%) | 26 (52) | |
| Body-mass index (kg/m2) | 27.9 (23.5–30.1) | |
| Comorbidities | ||
| Hypertension, n(%) | 18 (36) | |
| Ischemic heart disease, n(%) | 2 (4) | |
| Autoimmunologic diseases, n(%) | 2 (4) | |
| Hypothyroidism, n(%) | 2 (4) | |
| Diabetes mellitus type 2, n(%) | 5 (10) | |
| Hypercholesterolemia n(%) | 9 (18) | |
| Baseline melanoma-specific characteristics | ||
| Performance status, n(%) | 0 | 22 (44) |
| 1 | 28 (56) | |
| TNM stage IV AJCC 8th edition, n(%) | M1a | 6 (12) |
| M1b | 3 (6) | |
| M1c | 31 (62) | |
| M1d | 10 (20) | |
| Number of disease sites, n(%) | ≤3 | 30 (60) |
| >3 | 19 (38) | |
| Unknown | 1 (2) | |
| Site of metastasis at enrollment, n(%) | Lymph nodes | 34 (68) |
| Subcutaneous tissue | 17 (34) | |
| In-transit | 7 (14) | |
| Liver | 19 (38) | |
| Central nervous system | 10 (20) | |
| Lungs | 25 (50) | |
| Bones | 13 (26) | |
| Other | 19 (38) | |
| BRAF mutation, n(%) | Wild-type | 30 (60) |
| V600E | 16 (32) | |
| V600K | 3 (6) | |
| Undetermined | 1 (2) | |
| PD-L1 expression > 5%, n(%) | Present | 4 (8) |
| Absent | 28 (56) | |
| Not available | 18 (36) | |
| Basic laboratory parameters | ||
| Hemoglobin (g/dL) | 13.1 (11.2–14.6) | |
| Neutrophils (103/uL) | 4.8 (3.6–6.2) | |
| Lymphocytes (103/uL) | 2.1 (1.6–5.3) | |
| Platelet count (103/uL) | 280 (210–337) | |
| Lactate dehydrogenase (U/L) | 209.7 (175.4–472) | |
| Estimated glomerular filtration rate (mL/min/1.73 m2) | 76 (60–90) | |
| Alanine transaminase (U/L) | 21.9 (11.8–33.6) | |
| Aspartate aminotransferase (U/L) | 20.5 (16–30.2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pacholczak-Madej, R.; Grela-Wojewoda, A.; Puskulluoglu, M.; Lompart, J.; Las-Jankowska, M.; Krawczak, K.; Wrona, E.; Zaręba, L.; Żubrowska, J.; Walocha, J.; et al. Early Effects of Nivolumab and Ipilimumab Combined Immunotherapy in the Treatment of Metastatic Melanoma in Poland: A Multicenter Experience. Biomedicines 2022, 10, 2528. https://doi.org/10.3390/biomedicines10102528
Pacholczak-Madej R, Grela-Wojewoda A, Puskulluoglu M, Lompart J, Las-Jankowska M, Krawczak K, Wrona E, Zaręba L, Żubrowska J, Walocha J, et al. Early Effects of Nivolumab and Ipilimumab Combined Immunotherapy in the Treatment of Metastatic Melanoma in Poland: A Multicenter Experience. Biomedicines. 2022; 10(10):2528. https://doi.org/10.3390/biomedicines10102528
Chicago/Turabian StylePacholczak-Madej, Renata, Aleksandra Grela-Wojewoda, Mirosława Puskulluoglu, Joanna Lompart, Manuela Las-Jankowska, Katarzyna Krawczak, Ewa Wrona, Lech Zaręba, Justyna Żubrowska, Jerzy Walocha, and et al. 2022. "Early Effects of Nivolumab and Ipilimumab Combined Immunotherapy in the Treatment of Metastatic Melanoma in Poland: A Multicenter Experience" Biomedicines 10, no. 10: 2528. https://doi.org/10.3390/biomedicines10102528