
Latent Tuberculosis: A Promising New Compound to Treat Non-Replicating and Intramacrophagic Mycobacteria

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
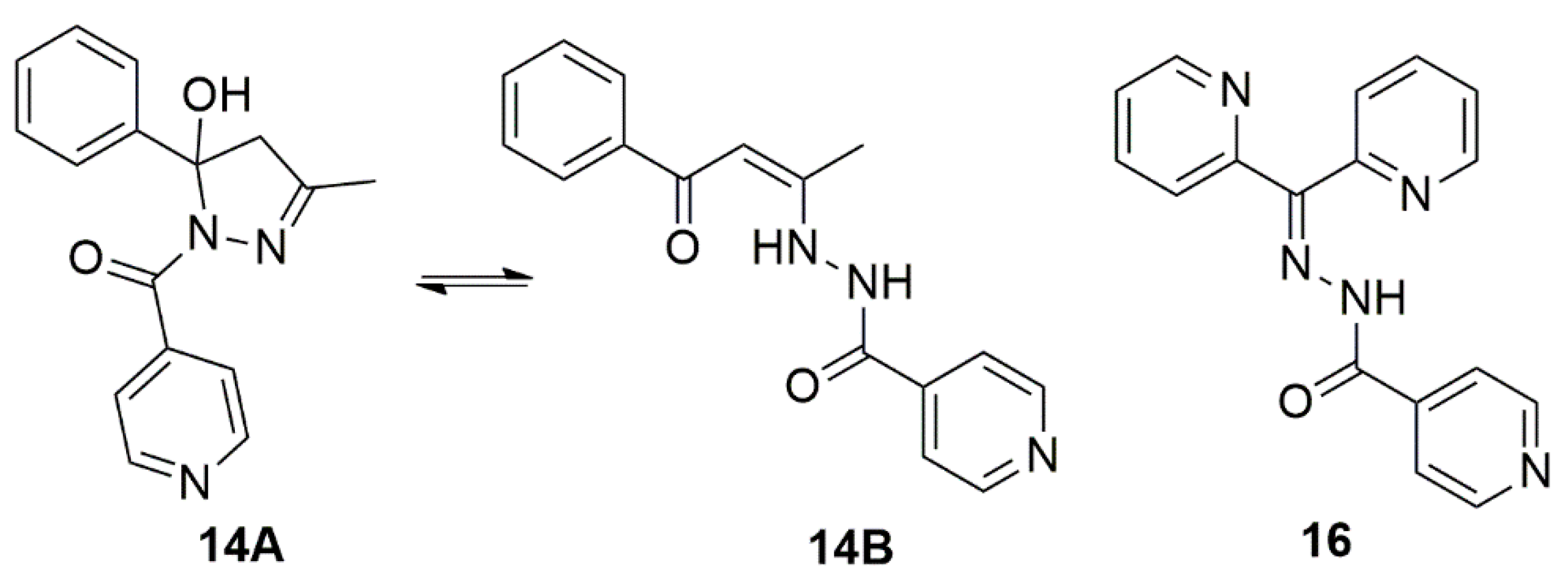
2.1. Hydrazones and Anti-TB Drugs
Analytical
2.2. Bacterial Culture
2.3. Minimal Inhibitory Concentration (MIC90) Evaluation against Replicating M. tuberculosis and M. smegmatis
2.4. Minimal Inhibitory Concentration Evaluation against Non-Replicating M. tuberculosis
2.5. Cytotoxicity against Eukaryotic Cells
2.6. Determination of the Selectivity Index
2.7. Intramacrophagic Activity
2.8. Time-Kill Curve
2.9. Evaluation of Activity Spectrum
3. Results
3.1. Minimum Inhibitory Concentration (MIC90) Values against M. tuberculosis in an Active and Non-Replicating Metabolic State
3.2. Cytotoxicity Index (IC50) and Selectivity Index (SI) Results against Macrophage Cells and Lung Fibroblasts at 24, 48, and 72 h
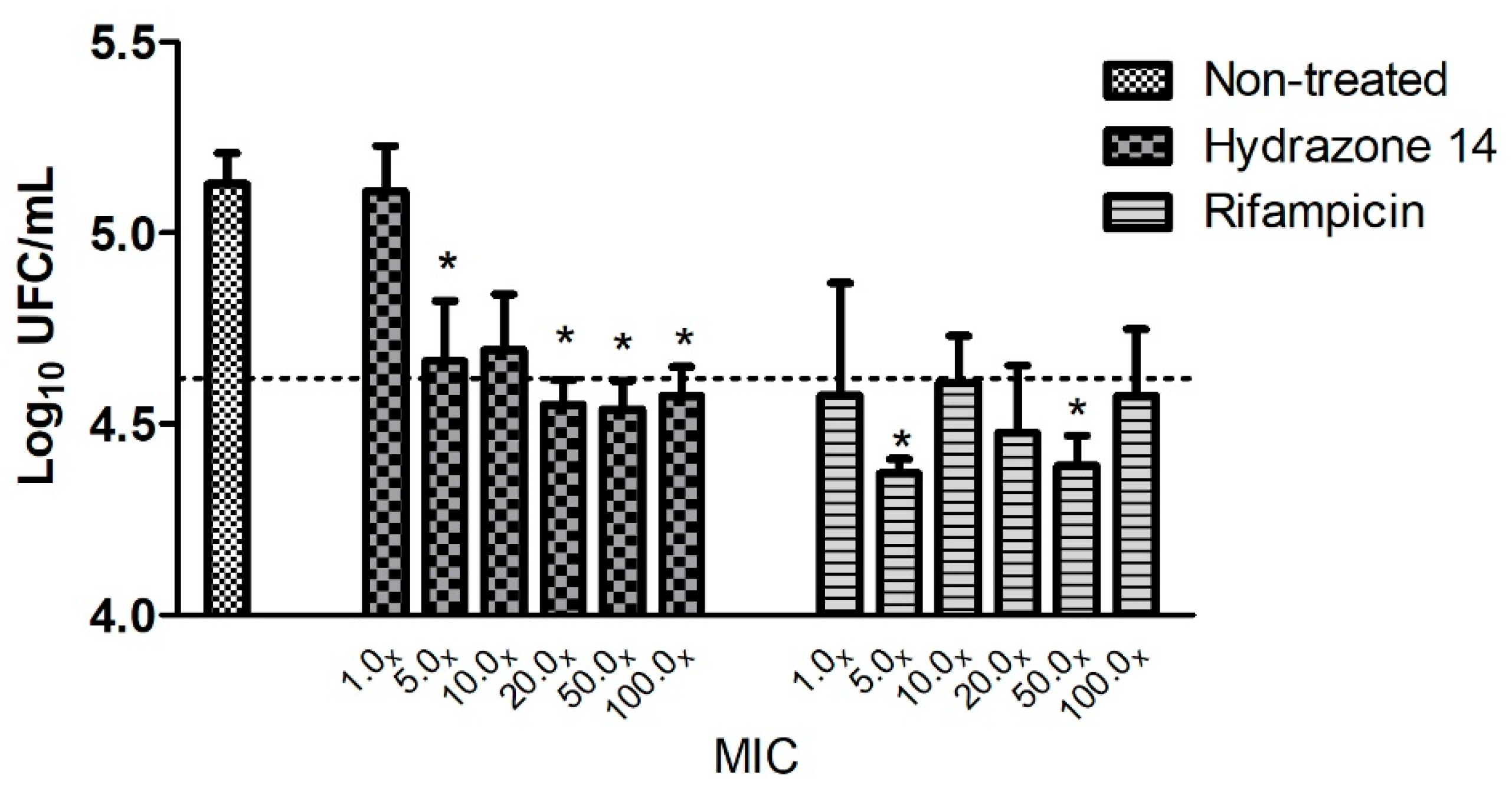
3.3. Intramacrophagic Activity
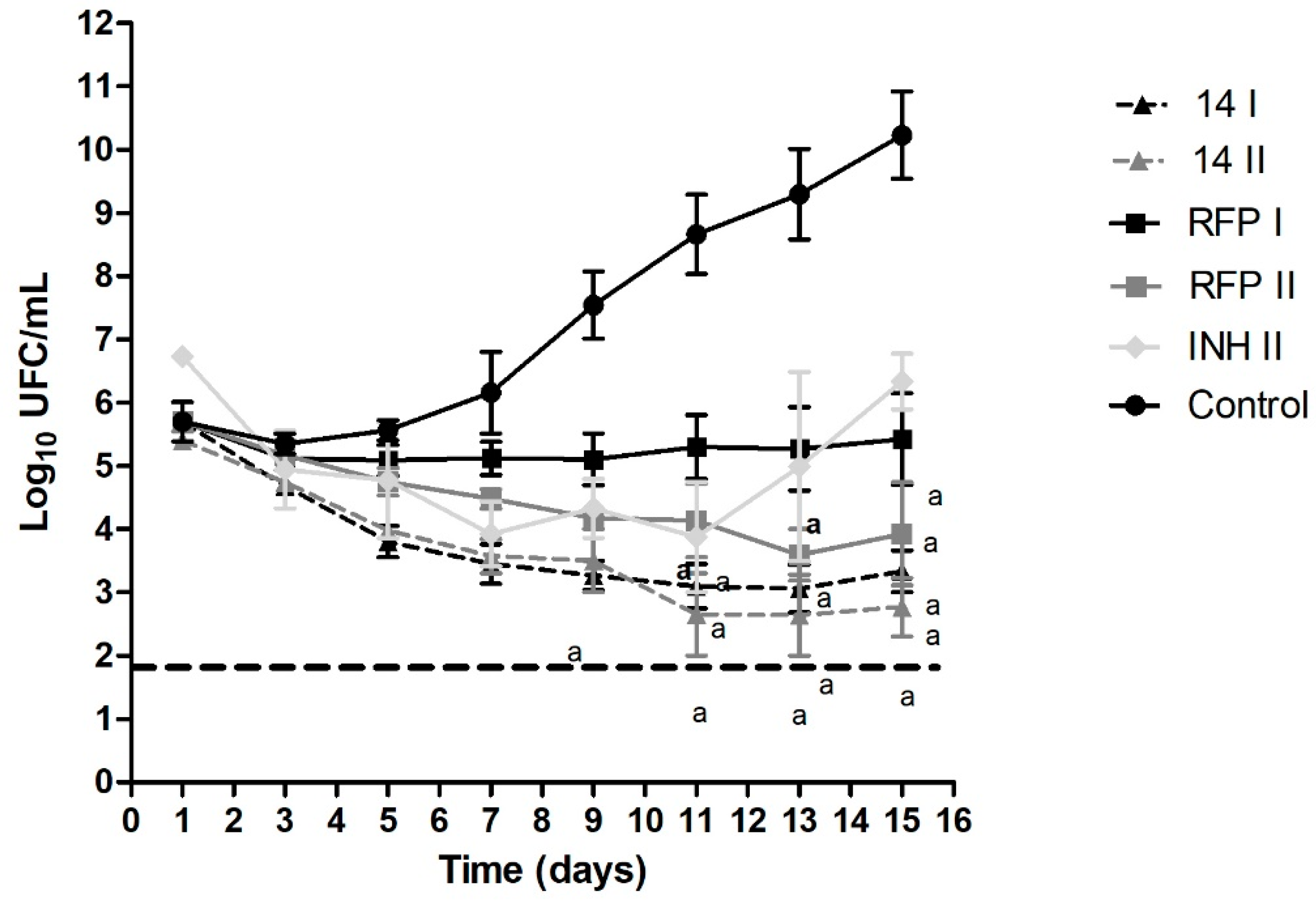
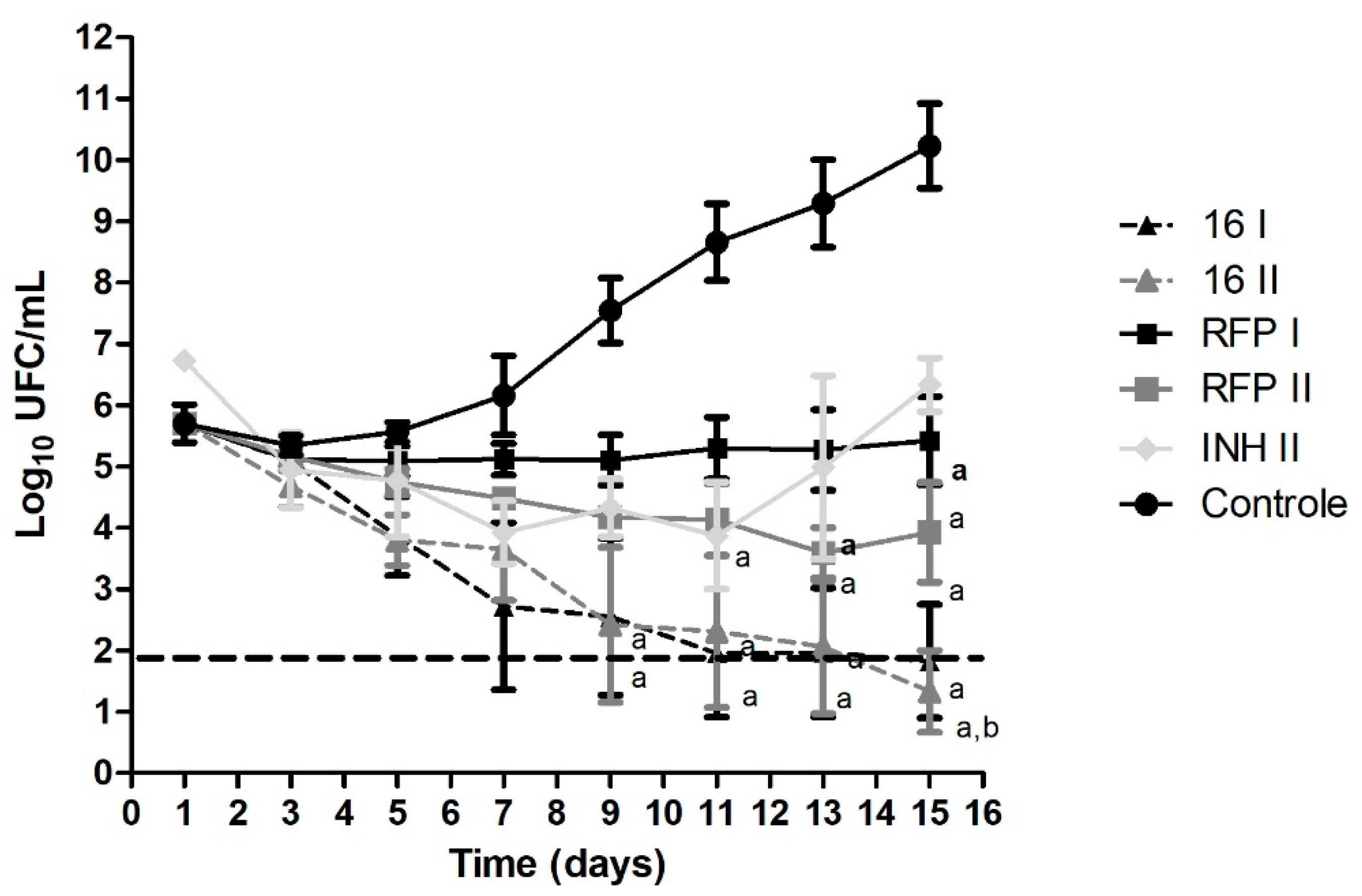
3.4. Time-Kill Curve
3.5. Spectrum Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240037021. [Google Scholar]
- Houben, R.M.G.J.; Dodd, P.J. The Global Burden of Latent Tuberculosis Infection: A Re-Estimation Using Mathematical Modelling. PLoS Med. 2016, 13, e1002152. [Google Scholar] [CrossRef] [PubMed]
- Furin, J.; Cox, H.; Pai, M. Tuberculosis. Lancet 2019, 393, 1642–1656. [Google Scholar] [CrossRef]
- Shea, K.M.; Kammerer, J.S.; Winston, C.A.; Navin, T.R.; Horsburgh, C.R. Estimated Rate of Reactivation of Latent Tuberculosis Infection in the United States, Overall and by Population Subgroup. Am. J. Epidemiol. 2014, 179, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Horsburgh, C.R.J. Priorities for the Treatment of Latent Tuberculosis Infection in the United States. N. Engl. J. Med. 2004, 350, 2060–2067. [Google Scholar] [CrossRef]
- Dye, C.; Glaziou, P.; Floyd, K.; Raviglione, M. Prospects for Tuberculosis Elimination. Annu. Rev. Public Health 2013, 34, 271–286. [Google Scholar] [CrossRef]
- World Health Organization. Latent Tuberculosis Infection Updated and Consolidated Guidelines for Programmatic Management. Patient Care 2019, 38, 13–14. [Google Scholar]
- McClintock, A.H.; Eastment, M.; McKinney, C.M.; Pitney, C.L.; Narita, M.; Park, D.R.; Dhanireddy, S.; Molnar, A. Treatment Completion for Latent Tuberculosis Infection: A Retrospective Cohort Study Comparing 9 Months of Isoniazid, 4 Months of Rifampin and 3 Months of Isoniazid and Rifapentine. BMC Infect. Dis. 2017, 17, 146. [Google Scholar] [CrossRef]
- Pease, C.; Hutton, B.; Yazdi, F.; Wolfe, D.; Hamel, C.; Quach, P.; Skidmore, B.; Moher, D.; Alvarez, G.G. Efficacy and Completion Rates of Rifapentine and Isoniazid (3HP) Compared to Other Treatment Regimens for Latent Tuberculosis Infection: A Systematic Review with Network Meta-Analyses. BMC Infect. Dis. 2017, 17, 265. [Google Scholar] [CrossRef]
- Bhat, Z.S.; Rather, M.A.; Maqbool, M.; Lah, H.U.; Yousuf, S.K.; Ahmad, Z. Cell Wall: A Versatile Fountain of Drug Targets in Mycobacterium Tuberculosis. Biomed. Pharmacother. 2017, 95, 1520–1534. [Google Scholar] [CrossRef]
- Hu, Y.Q.; Zhang, S.; Zhao, F.; Gao, C.; Feng, L.S.; Lv, Z.S.; Xu, Z.; Wu, X. Isoniazid Derivatives and Their Anti-Tubercular Activity. Eur. J. Med. Chem. 2017, 133, 255–267. [Google Scholar] [CrossRef]
- Ferraresi-Curotto, V.; Echeverría, G.A.; Piro, O.E.; Pis-Diez, R.; González-Baró, A.C. Synthesis and Characterization of a Series of Isoniazid Hydrazones. Spectroscopic and Theoretical Study. J. Mol. Struct. 2017, 1133, 436–447. [Google Scholar] [CrossRef]
- Pavan, F.R.; Maia, P.I.d.S.; Leite, S.R.A.; Deflon, V.M.; Batista, A.A.; Sato, D.N.; Franzblau, S.G.; Leite, C.Q.F. Thiosemicarbazones, Semicarbazones, Dithiocarbazates and Hydrazide/Hydrazones: Anti-Mycobacterium Tuberculosis Activity and Cytotoxicity. Eur. J. Med. Chem. 2010, 45, 1898–1905. [Google Scholar] [CrossRef]
- Verma, G.; Marella, A.; Shaquiquzzaman, M.; Akhtar, M.; Ali, M.R.; Alam, M.M. A Review Exploring Biological Activities of Hydrazones. J. Pharm. Bioallied Sci. 2014, 6, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Popiołek, Ł. Hydrazide–Hydrazones as Potential Antimicrobial Agents: Overview of the Literature since 2010. Med. Chem. Res. 2017, 26, 287–301. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, P.V.; Caldwell, L.M.; Chaston, T.B.; Chin, P.; Richardson, D.R. Cytotoxic Iron Chelators: Characterization of the Structure, Solution Chemistry and Redox Activity of Ligands and Iron Complexes of the Di-2-Pyridyl Ketone Isonicotinoyl Hydrazone (HPKIH) Analogues. J. Biol. Inorg. Chem. 2003, 8, 866–880. [Google Scholar] [CrossRef]
- Palomino, J.; Martin, A.; Camacho, M.; Guerra, H.; Swings, J.; Portaels, F. Resazurin Microtiter Assay Plate: Simple and Inexpensive Method for Detection of Drug Resistance in Mycobacterium Tuberculosis Resazurin Microtiter Assay Plate: Simple and Inexpensive Method for Detection of Drug Resistance in Mycobacterium Tuberculosis. Antimicrobail Agents Chemother. 2002, 46, 2720–2722. [Google Scholar] [CrossRef]
- Wayne, L.G.; Sohaskey, C.D. Nonreplicanting Persistence of Mycobacterium Tuberculosis. Annu. Rev. Microbiol. 2001, 55, 139–163. [Google Scholar] [CrossRef]
- Solcia, M.C.; Campos, D.L.; Grecco, J.A.; Paiva Silva, C.S.; Bento da Silva, P.; Cristiane da Silva, I.; Balduino da Silva, A.P.; Silva, J.; Oda, F.B.; Gonzaga dos Santos, A.; et al. Growth-Inhibitory Effects of Tris-(1,10-Phenanthroline) Iron (II) against Mycobacterium Tuberculosis in Vitro and in Vivo. Tuberculosis 2021, 128, 102087. [Google Scholar] [CrossRef]
- Cho, S.H.; Warit, S.; Wan, B.; Hwang, C.H.; Pauli, G.F.; Franzblau, S.G. Low-Oxygen-Recovery Assay for High-Throughput Screening of Compounds against Nonreplicating Mycobacterium Tuberculosis. Antimicrob. Agents Chemother. 2007, 51, 1380–1385. [Google Scholar] [CrossRef]
- Campos, D.L.; Machado, I.; Ribeiro, C.M.; Gambino, D.; Pavan, F.R. Bactericidal Effect of Pyridine-2-Thiol 1-Oxide Sodium Salt and Its Complex with Iron against Resistant Clinical Isolates of Mycobacterium Tuberculosis. J. Antibiot. 2020, 73, 120–124. [Google Scholar] [CrossRef]
- Dos Santos Fernandes, G.F.; De Souza, P.C.; Moreno-Viguri, E.; Santivañez-Veliz, M.; Paucar, R.; Pérez-Silanes, S.; Chegaev, K.; Guglielmo, S.; Lazzarato, L.; Fruttero, R.; et al. Design, Synthesis, and Characterization of N-Oxide-Containing Heterocycles with in Vivo Sterilizing Antitubercular Activity. J. Med. Chem. 2017, 60, 8647–8660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Steenwinkel, J.E.M.; de Knegt, G.J.; ten Kate, M.T.; van Belkum, A.; Verbrugh, H.A.; Kremer, K.; van Soolingen, D.; Bakker-Woudenberg, I.A.J.M. Time-Kill Kinetics of Anti-Tuberculosis Drugs, and Emergence of Resistance, in Relation to Metabolic Activity of Mycobacterium Tuberculosis. J. Antimicrob. Chemother. 2010, 65, 2582–2589. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institure. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Clinical and Laboratory Standards Institure: Wayne, PA, USA, 2018; Volume 11, ISBN 1-56238-836-3. [Google Scholar]
- Volynets, G.P.; Tukalo, M.A.; Bdzhola, V.G.; Derkach, N.M.; Gumeniuk, M.I.; Tarnavskiy, S.S.; Yarmoluk, S.M. Novel Isoniazid Derivative as Promising Antituberculosis Agent. Future Microbiol. 2020, 15, 869–879. [Google Scholar] [CrossRef]
- Silva, P.B.; De Souza, P.C.; Maria, G.; Calixto, F.; Lopes, E.D.O.; Frem, R.C.G.; Netto, A.V.G.; Mauro, A.E.; Pavan, F.R.; Chorilli, M. In Vitro Activity of Copper (II) Complexes, Loaded or Unloaded into a Nanostructured Lipid System, against Mycobacterium Tuberculosis. Int. J. Mol. Sci. 2016, 17, 745. [Google Scholar] [CrossRef] [PubMed]
- Pankey, G.A.; Sabath, L.D. Clinical Relevance of Bacteriostatic versus Bactericidal Mechanisms of Action in the Treatment of Gram-Positive Bacterial Infections. Clin. Infect. Dis. 2004, 38, 864–870. [Google Scholar] [CrossRef]
- Huaman, M.A.; Sterling, T.R. Treatment of Latent Tuberculosis Infection—An Update. Clin. Chest Med. 2019, 40, 839–848. [Google Scholar] [CrossRef]
- Paton, N.I.; Borand, L.; Benedicto, J.; Kyi, M.M.; Mahmud, A.M.; Norazmi, M.N.; Sharma, N.; Chuchottaworn, C.; Huang, Y.W.; Kaswandani, N.; et al. Diagnosis and Management of Latent Tuberculosis Infection in Asia: Review of Current Status and Challenges. Int. J. Infect. Dis. 2019, 87, 21–29. [Google Scholar] [CrossRef]
- Henry Boom, W.; Schaible, U.E.; Achkar, J.M. The Knowns and Unknowns of Latent Mycobacterium Tuberculosis Infection. J. Clin. Investig. 2021, 131, 20–22. [Google Scholar] [CrossRef]
- Behr, M.A.; Kaufmann, E.; Duffin, J.; Edelstein, P.H.; Ramakrishnan, L. Latent Tuberculosis: Two Centuries of Confusion. Am. J. Respir. Crit. Care Med. 2021, 204, 142–148. [Google Scholar] [CrossRef]
- Dhar, G.C. Treatment of Latent Tuberculosis Infection. Ann. Intern. Med. 2015, 162, 394. [Google Scholar] [CrossRef]
- Peddireddy, V.; Doddam, S.N.; Ahmed, N. Mycobacterial Dormancy Systems and Host Responses in Tuberculosis. Front. Immunol. 2017, 8, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilchèze, C.; Jacobs, W.R., Jr. The Mechanism of Isoniazid Killing: Clarity Through the Scope of Genetics. Annu. Rev. Microbiol. 2007, 61, 35–50. [Google Scholar] [CrossRef]
- Heianza, Y.; Ma, W.; Li, X.; Cao, Y.; Chan, A.T.; Rimm, E.B.; Hu, F.B.; Rexrode, K.M.; Manson, J.E.; Qi, L. Duration and Life-Stage of Antibiotic Use and Risks of All-Cause and Cause-Specific Mortality: Prospective Cohort Study. Circ. Res. 2020, 126, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Cadena, A.M.; Fortune, S.M.; Flynn, J.L. Heterogeneity in Tuberculosis. Nat. Rev. Immunol. 2017, 17, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Ferluga, J.; Yasmin, H.; Al-Ahdal, M.N.; Bhakta, S.; Kishore, U. Natural and Trained Innate Immunity against Mycobacterium Tuberculosis. Immunobiology 2020, 225, 151951. [Google Scholar] [CrossRef] [PubMed]
- Grada, A.; Bunick, C.G. Spectrum of Antibiotic Activity and Its Relevance to the Microbiome. JAMA Netw. Open 2021, 4, e215357. [Google Scholar] [CrossRef]
- Alliance, G.; Development, T.B.D.; Street, B.; York, N. Handbook of Anti-Tuberculosis Agents. Introduction. Tuberculosis 2008, 88, 85–86. [Google Scholar] [CrossRef]
- Met, T.; Ei-bahnasawy, R.M.; Ei-kom, S. Benzoylacetone Isonicotinoyl Hydrazone Complexes of Divalent Transition Metals. Transit. Met. Chem. 1993, 18, 505–509. [Google Scholar]
- Hosseini-Monfared, H.; Bikas, R.; Sanchiz, J.; Lis, T.; Siczek, M.; Tucek, J.; Zboril, R.; Mayer, P. Syntheses, Structures and Magnetic Properties of Azido- and Phenoxo-Bridged Complexes of Manganese Containing Tridentate Aroylhydrazone Based Ligands. Polyhedron 2013, 61, 45–55. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compounds | MIC90 1 Replicating | MIC90 Non-Replicating | ||
|---|---|---|---|---|
| μM | μg/mL | μM | μg/mL | |
| Hydrazone 14 | 1.23 ± 0.53 | 0.35 ± 0.15 | 6.31 ± 5.72 | 1.77 ± 1.61 |
| Hydrazone 16 | 6.01 ± 0.22 | 1.82 ± 0.68 | 7.76 ± 5.70 | 2.35 ± 1.73 |
| Rifampicin | 0.05 ± 0.001 | 0.04 ± 0.01 | <0.36 | <0.3 |
| Isoniazid | 0.44 ± 0.29 | 0.06 ± 0.04 | >328.13 | >45.0 |
| IC50 (μg/mL) | IS | ||||||
|---|---|---|---|---|---|---|---|
| Cells | Time | H14 | H16 | INH | H14 | H16 | INH |
| J774A.1 | 24 h | >100 | >100 | >100 | >289.02 | >54.85 | >1666.66 |
| 48 h | 83.34 ± 28.85 | 95.60 ± 7.61 | >100 | 240.88 | 52.44 | >1666.66 | |
| 72 h | 81.81 ± 31.50 | 72.29 ± 47.99 | >100 | 236.46 | 39.65 | >1666.66 | |
| MRC-5 | 24 h | >100 | >100 | >100 | >289.02 | >54.85 | >1666.66 |
| 48 h | >100 | 96.23 ± 6.53 | >100 | >289.02 | 52.79 | >1666.66 | |
| 72 h | >100 | 67.43 ± 28.66 * | >100 | >289.02 | 36.99 | >1666.66 | |
| Molecules | S. typhimurium | P. aeruginosa | S. aureus | E. coli | M. smegmatis |
|---|---|---|---|---|---|
| 14 | >100 | >100 | >100 | >100 | >25.0 |
| 16 | >100 | >100 | >100 | >100 | n.d. |
| Gentamicin | 1.16 ± 0.38 | 2.02 ± 0.66 | 3.97 ± 2.35 | 5.07 ± 0.14 | n.d. |
| Rifampicin | n.d. * | n.d. | n.d. | n.d. | 2.4 ± 1.5 |
| Scheme Treatment | Treatment Period | Efficacy |
|---|---|---|
| Isoniazid monotherapy | 6–9 months | 90% |
| Rifampicin monotherapy | 4 months | ~90% |
| Isoniazid and Rifampicin | 3–4 months | n.p. |
| Isoniazid and Rifapentine | 3 months | n.p. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos, D.L.; Demarqui, F.M.; Solcia, M.C.; de Souza, P.C.; da Silva Maia, P.I.; Deflon, V.M.; Pavan, F.R. Latent Tuberculosis: A Promising New Compound to Treat Non-Replicating and Intramacrophagic Mycobacteria. Biomedicines 2022, 10, 2398. https://doi.org/10.3390/biomedicines10102398
Campos DL, Demarqui FM, Solcia MC, de Souza PC, da Silva Maia PI, Deflon VM, Pavan FR. Latent Tuberculosis: A Promising New Compound to Treat Non-Replicating and Intramacrophagic Mycobacteria. Biomedicines. 2022; 10(10):2398. https://doi.org/10.3390/biomedicines10102398
Chicago/Turabian StyleCampos, Débora Leite, Fernanda Manaia Demarqui, Mariana Cristina Solcia, Paula Carolina de Souza, Pedro Ivo da Silva Maia, Victor Marcelo Deflon, and Fernando Rogério Pavan. 2022. "Latent Tuberculosis: A Promising New Compound to Treat Non-Replicating and Intramacrophagic Mycobacteria" Biomedicines 10, no. 10: 2398. https://doi.org/10.3390/biomedicines10102398