
Early Spatiotemporal Patterns and Population Characteristics of the COVID-19 Pandemic in Southeast Asia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Compilation
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
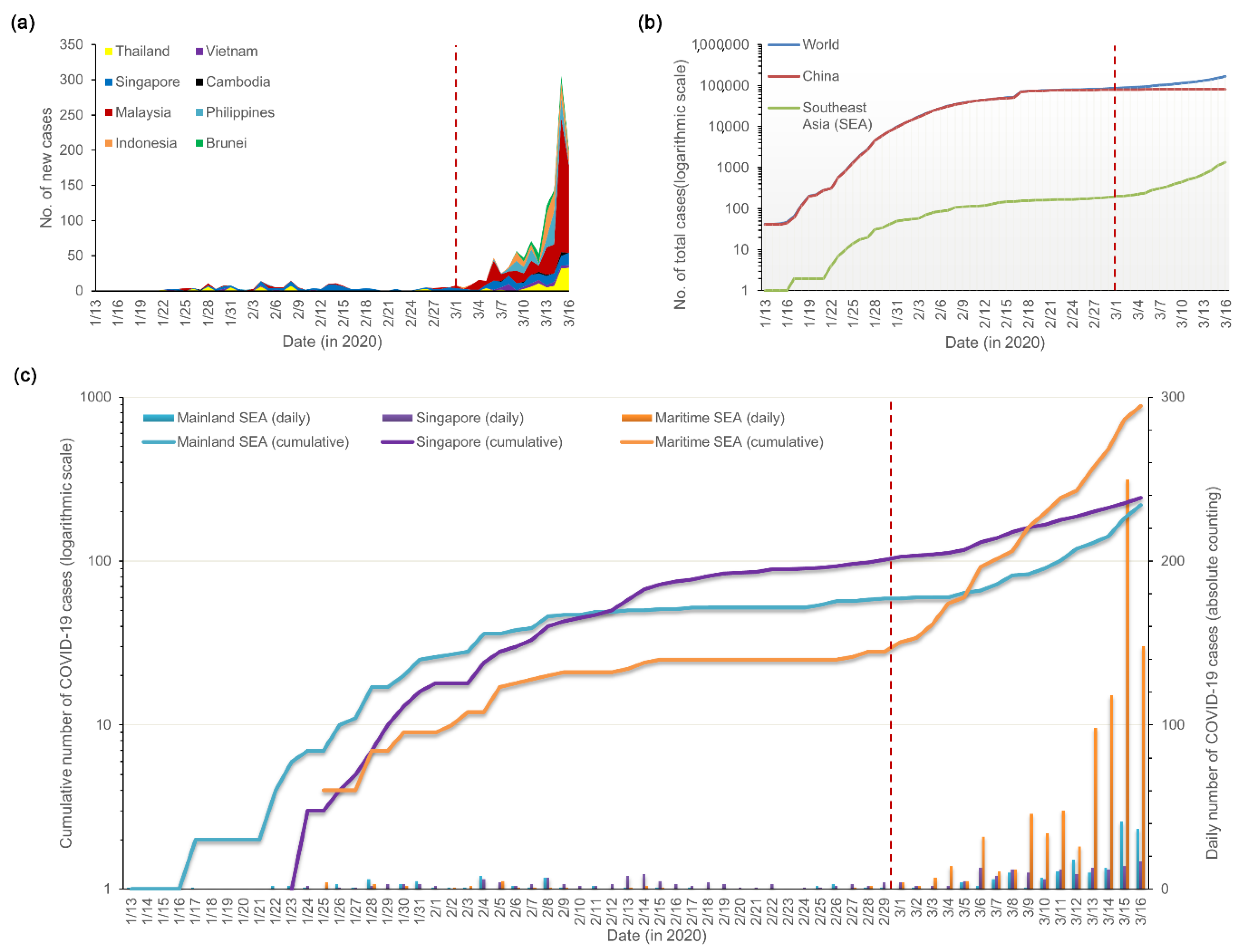
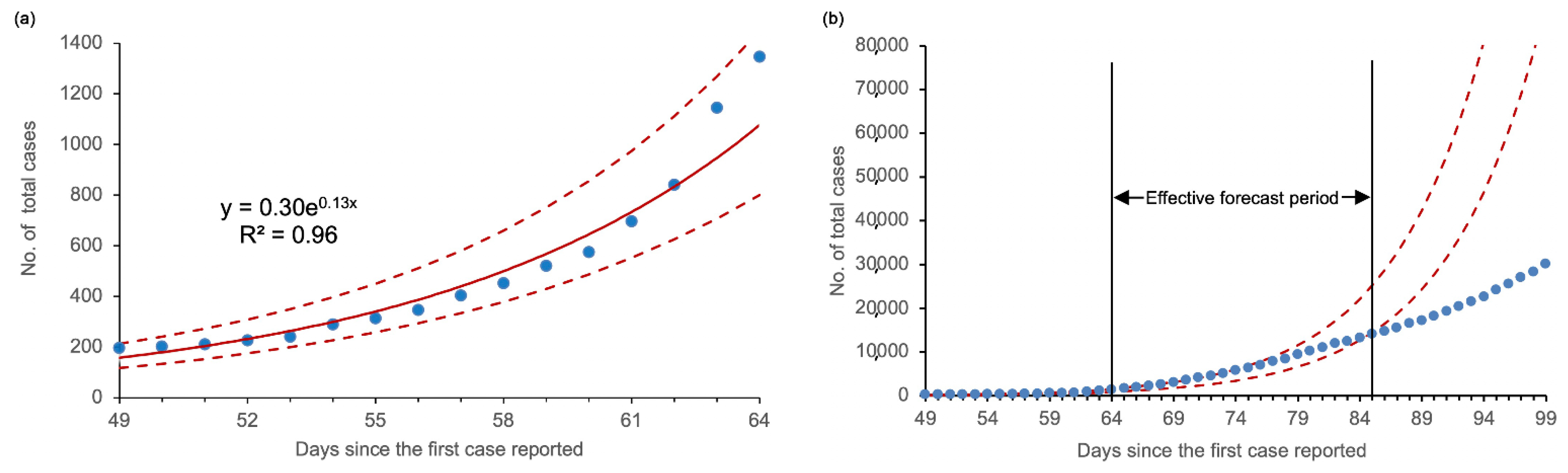
3.1. Temporal Distribution and Incidence Trends
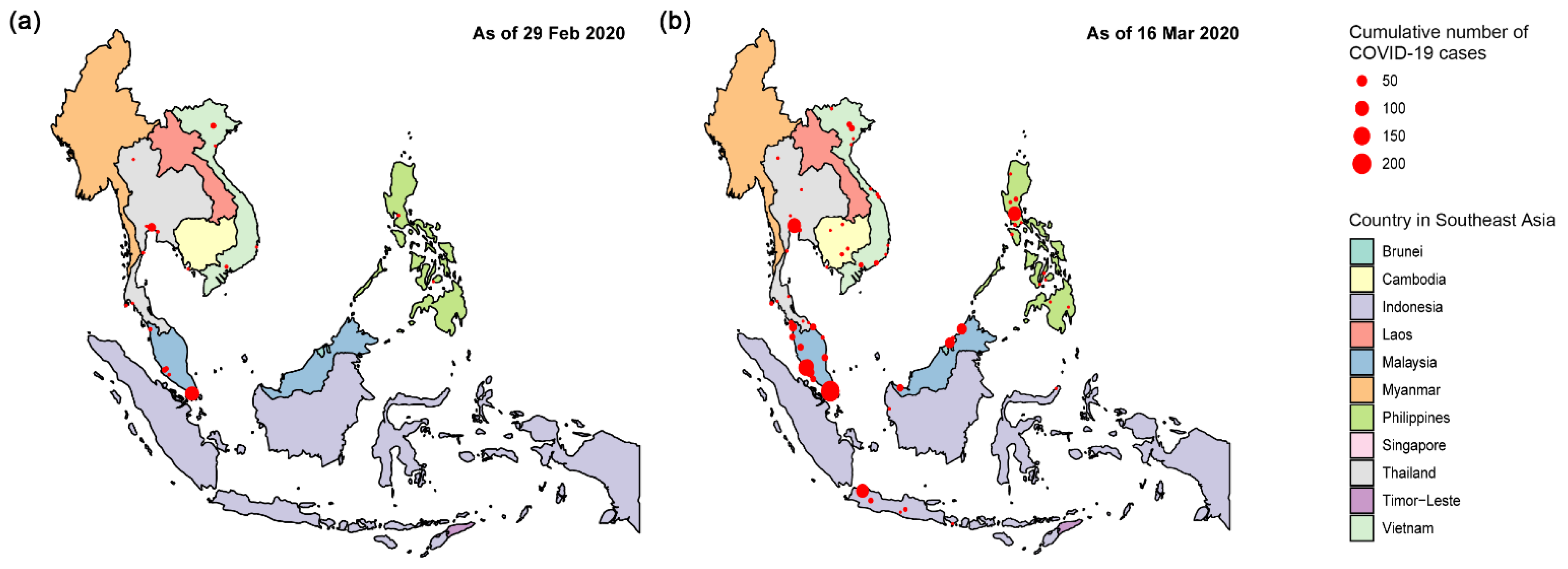
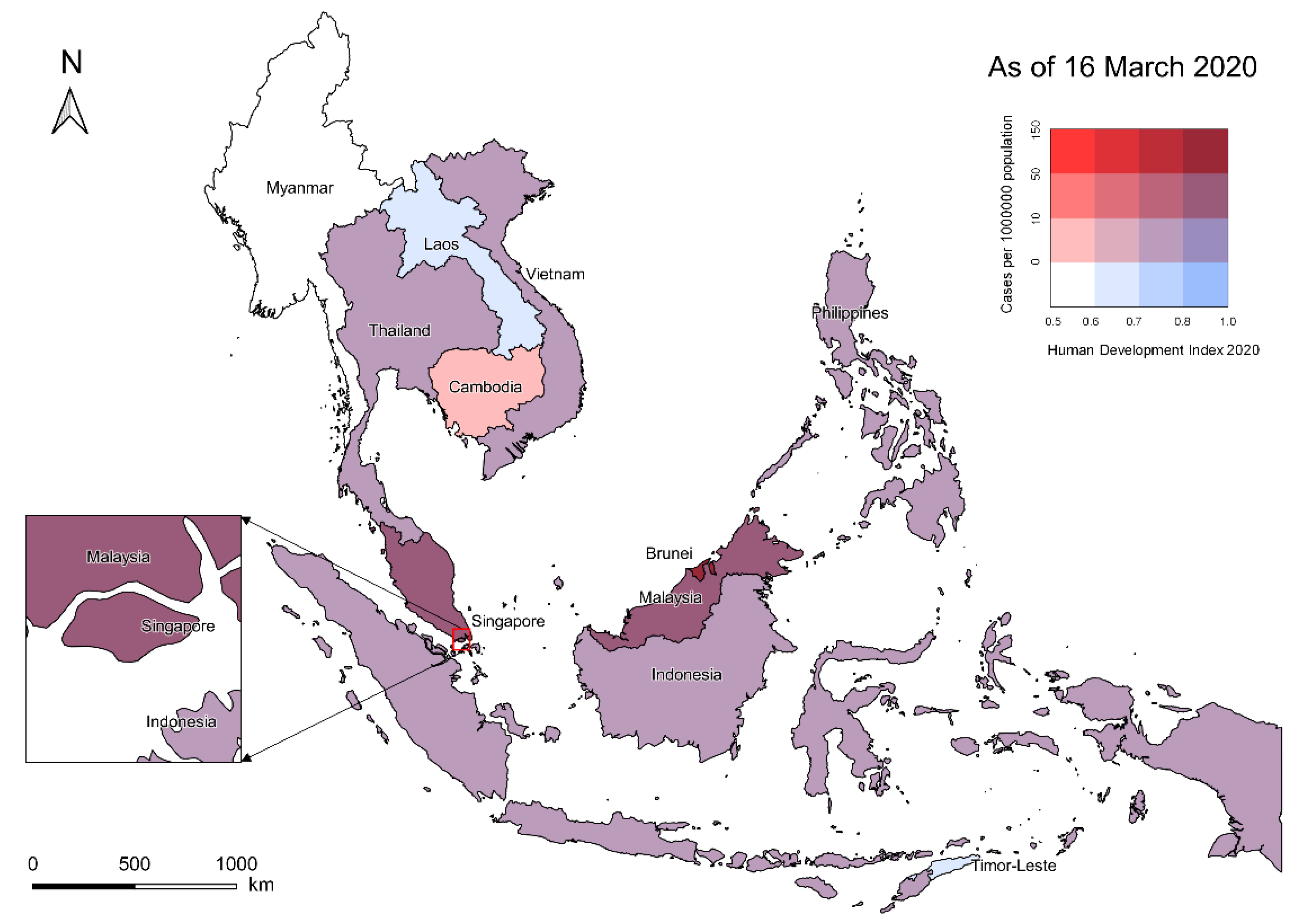
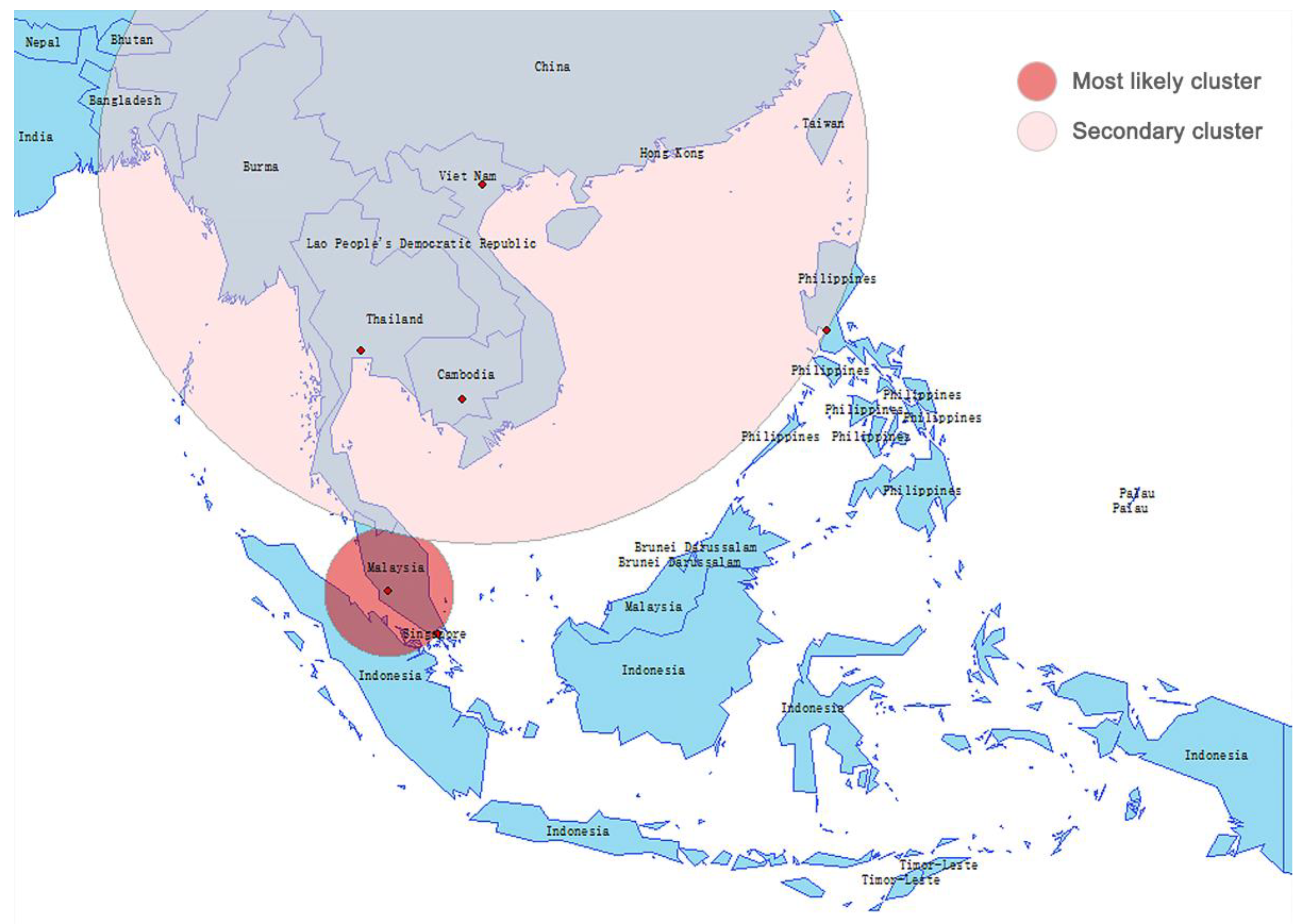
3.2. Spatial Distribution and Spatiotemporal Clusters
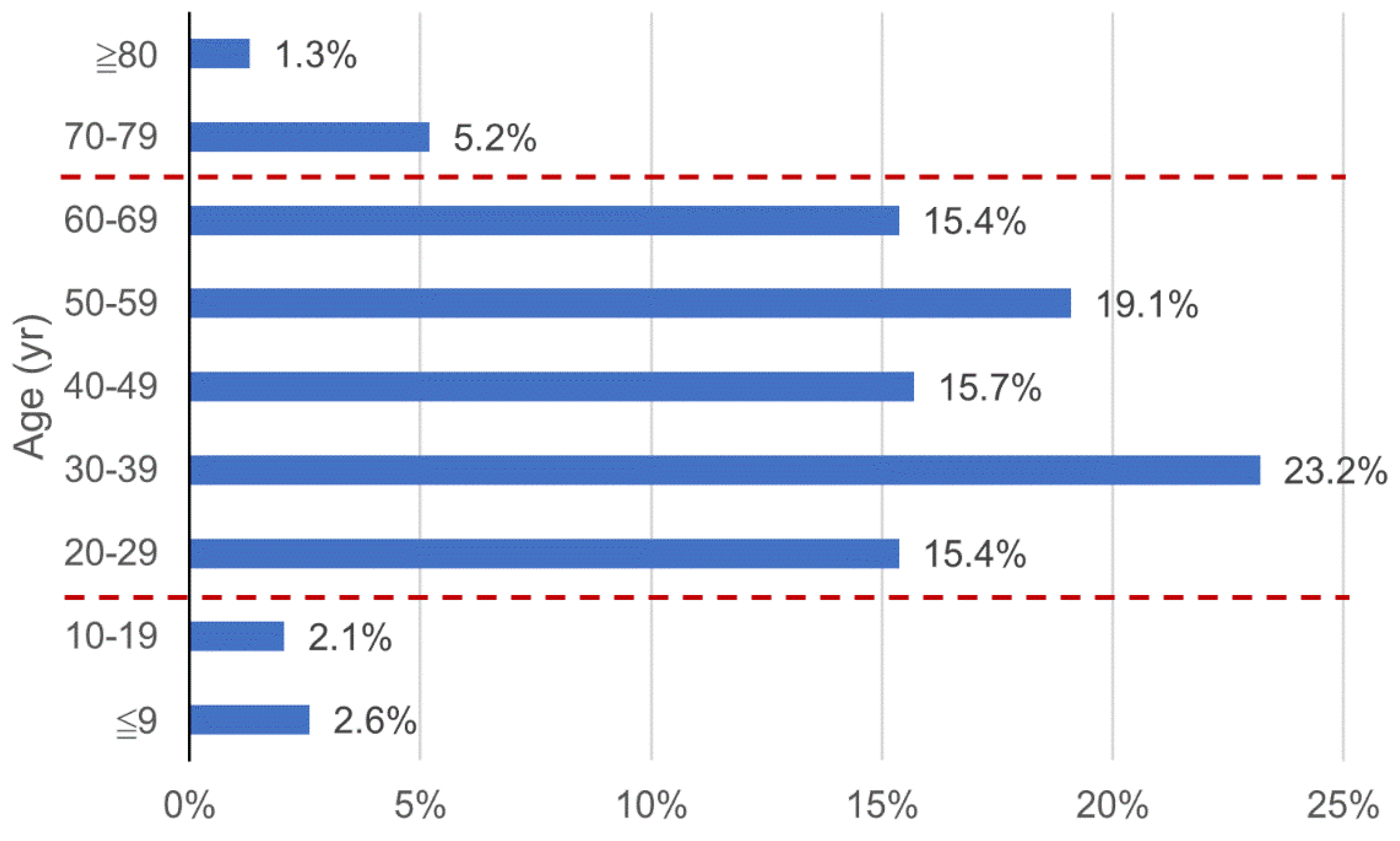
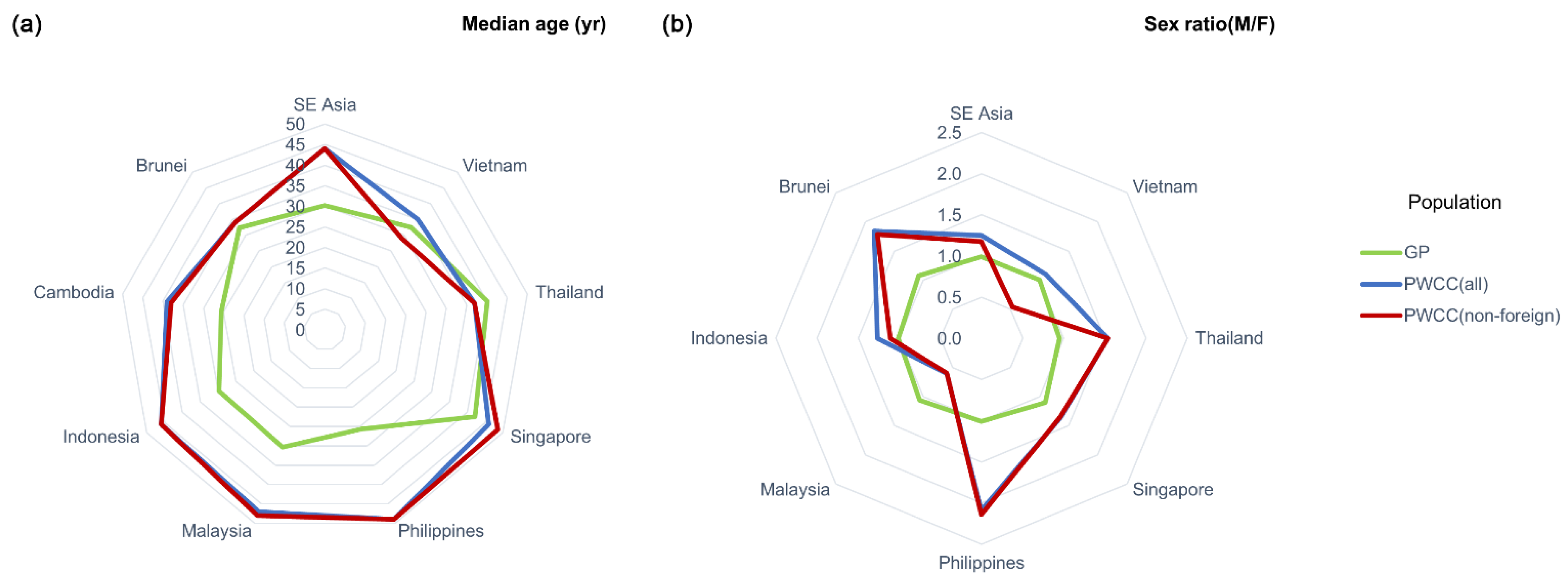
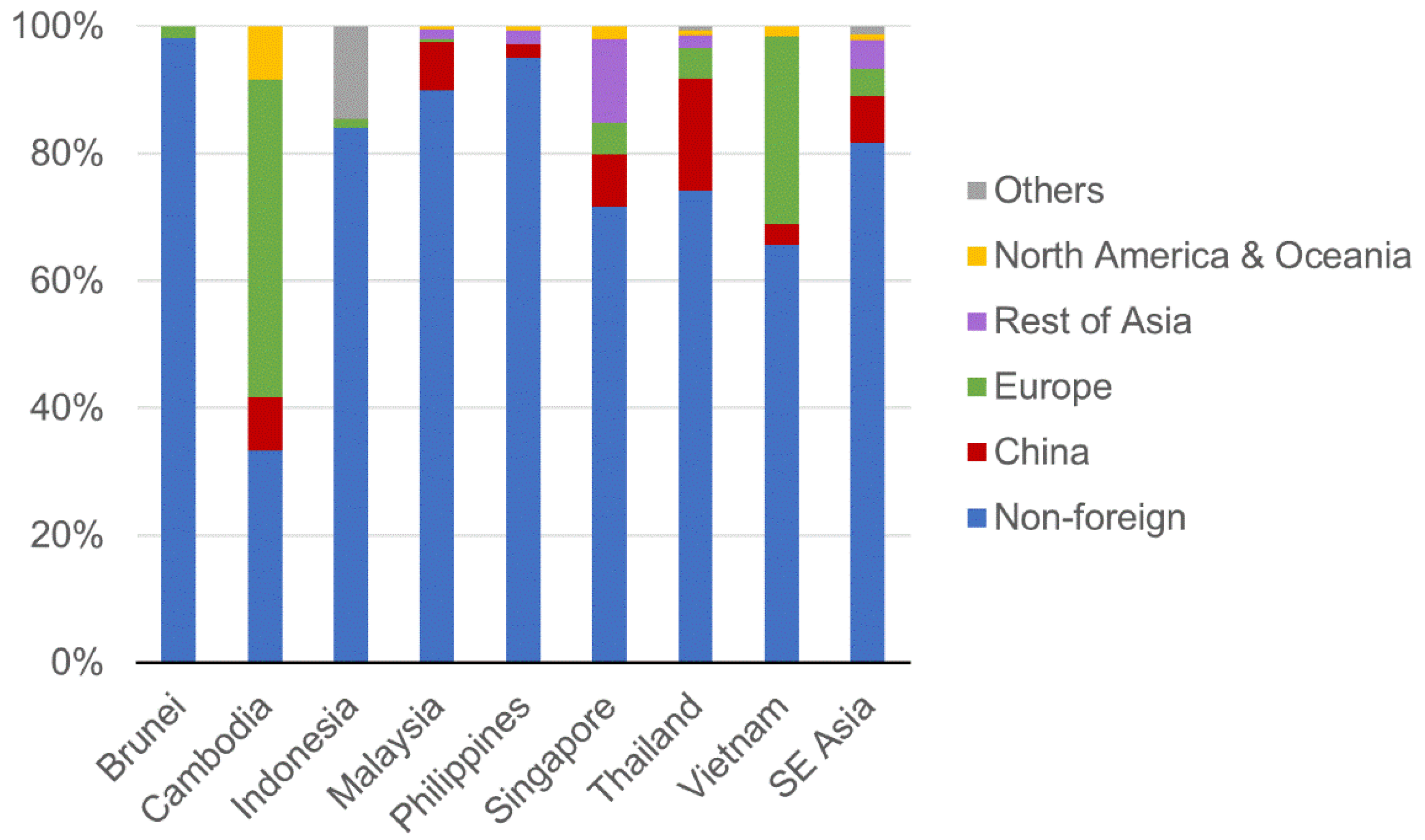
3.3. Demographic Characteristics and Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 12 March 2020).
- Priyadarshini, I.; Mohanty, P.; Kumar, R.; Son, L.H.; Chau, H.; Nhu, V.H.; Thi, N.P.; Tien, B.D. Analysis of Outbreak and Global Impacts of the COVID-19. Healthcare 2020, 8, 148. [Google Scholar] [CrossRef] [PubMed]
- Joob, B.; Wiwanitkit, V. Outbreak of COVID-19 in Thailand: Time serial analysis on imported and local transmission cases. Int. J. Prev. Med. 2020, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Edrada, E.M.; Lopez, E.B.; Villarama, J.B.; Salva Villarama, E.P.; Dagoc, B.F.; Smith, C.; Sayo, A.R.; Verona, J.A.; Trifalgar-Arches, J.; Lazaro, J.; et al. First COVID-19 infections in the Philippines: A case report. Trop. Med. Health 2020, 48, 21. [Google Scholar] [CrossRef] [Green Version]
- Gaynor, J. Maritime Southeast Asia: Not Just a Crossroads. Educ. Asia 2014, 19, 14–19. [Google Scholar]
- Hoang, M.; Nguyen, P.; Tran, T.; Khuong, L.A. The COVID-19 pandemic in the ASEAN: A preliminary report on the spread, burden and medical capacities. Asian Pac. J. Trop Med. 2020, 13, 247–251. [Google Scholar] [CrossRef]
- Bond, K.C.; Macfarlane, S.B.; Burke, C.; Ungchusak, K.; Wibulpolprasert, S. The evolution and expansion of regional disease surveillance networks and their role in mitigating the threat of infectious disease outbreaks. Emerg. Health Threat. J. 2013, 6, 19913. [Google Scholar] [CrossRef] [Green Version]
- Amodio, E.; Vitale, F.; Cimino, L.; Casuccio, A.; Tramuto, F. Outbreak of Novel Coronavirus (SARS-Cov-2): First Evidences From International Scientific Literature and Pending Questions. Healthcare 2020, 8, 51. [Google Scholar] [CrossRef] [Green Version]
- Pung, R.; Chiew, C.J.; Young, B.E.; Chin, S.; Chen, M.I.; Clapham, H.E.; Cook, A.R.; Maurer-Stroh, S.; Toh, M.; Poh, C.; et al. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- Supramanian, R.K.; Sivaratnam, L.; Rahim, A.A.; Abidin, N.D.I.Z.; Richai, O.; Zakiman, Z.; Taib, S.M.; Soo, L.; Jamalullai, S.H.S.I.; Khirusalleh, M.N.A.; et al. Descriptive epidemiology of the first wave of COVID-19 in Petaling District, Malaysia: Focus on asymptomatic transmission. West. Pac. Surveill Response J. 2021, 2. [Google Scholar] [CrossRef]
- Nguyen, T.V.; Tran, Q.D.; Phan, L.T.; Vu, L.N.; Truong, D.T.T.; Truong, H.C.; Le, T.N.; Vien, L.D.K.; Nguyen, T.V.; Luong, Q.C.; et al. In the interest of public safety: Rapid response to the COVID-19 epidemic in Vietnam. BMJ Glob. Health 2021, 6, e004100. [Google Scholar] [CrossRef] [PubMed]
- Galvani, A.P.; Lei, X.; Jewell, N.P. Severe acute respiratory syndrome: Temporal stability and geographic variation in case-fatality rates and doubling times. Emerg. Infect. Dis. 2003, 9, 991–994. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Jia, Y.; Chen, L.; Guo, L.; Shu, B.; Long, E. COVID-19 epidemic prediction and the impact of public health interventions: A review of COVID-19 epidemic models. Infect. Dis. Model. 2021, 6, 324–342. [Google Scholar]
- Obadia, T.; Haneef, R.; Boëlle, P. The R0 package: A toolbox to estimate reproduction numbers for epidemic outbreaks. BMC Med. Inf. Decis 2012, 12, 147. [Google Scholar] [CrossRef] [PubMed]
- Ganyani, T.; Kremer, C.; Chen, D.; Torneri, A.; Faes, C.; Wallinga, J.; Hens, N. Estimating the generation interval for coronavirus disease (COVID-19) based on symptom onset data, March 2020. Eurosurveillance 2020, 25, 2000257. [Google Scholar] [CrossRef]
- Jones, S.G.; Kulldorff, M.; Bejon, P. Influence of spatial resolution on space-time disease cluster detection. PLoS ONE 2012, 7, e48036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malaysia-D-GoH KPK Press Statement 13 March 2020—Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/03/13/kenyataan-akhbar-kpk-13-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 14 March 2020).
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—42. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200302-sitrep-42-covid-19.pdf?sfvrsn=224c1add_2 (accessed on 3 March 2020).
- UNDP. Human Development Indices and Indicators: 2018 Statistical Update. Available online: http://hdr.undp.org/sites/default/files/hdr2018_technical_notes.pdf (accessed on 24 August 2020).
- Sigler, T.; Mahmuda, S.; Kimpton, A.; Loginova, J.; Wohland, P.; Charles-Edwards, E.; Corcoran, J. The socio-spatial determinants of COVID-19 diffusion: The impact of globalisation, settlement characteristics and population. Glob. Health 2021, 17, 56. [Google Scholar] [CrossRef]
- Sirkeci, I.; Yüceşahin, M. Coronavirus and Migration: Analysis of Human Mobility and the Spread of COVID-19. Migr. Lett. 2020, 17, 379–398. [Google Scholar] [CrossRef] [Green Version]
- UNDP. Human Development Report 2020. Available online: https://report.hdr.undp.org (accessed on 1 March 2021).
- Chen, J.I.; Yap, J.C.; Hsu, L.Y.; Teo, Y.Y. COVID-19 and Singapore: From Early Response to Circuit Breaker. Ann. Acad. Med. Singap. 2020, 49, 561–572. [Google Scholar] [CrossRef]
- Wong, D.; Li, Y. Spreading of COVID-19: Density matters. PLoS ONE 2020, 15, e242398. [Google Scholar] [CrossRef]
- van Empel, G.; Mulyanto, J.; Wiratama, B.S. Undertesting of COVID-19 in Indonesia: What has gone wrong? J. Glob. Health 2020, 10, 20306. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 in the Philippines Situation Report 06. Available online: https://www.who.int/philippines/internal-publications-detail/covid-19-in-the-philippines-situation-report-06 (accessed on 23 March 2020).
- Zhu, Y.; Chen, Y.Q. On a Statistical Transmission Model in Analysis of the Early Phase of COVID-19 Outbreak. Stat. Biosci. 2020, 13, 1–17. [Google Scholar] [CrossRef]
- Majumder, M.S.; Mandl, K.D. Early Transmissibility Assessment of a Novel Coronavirus in Wuhan, China. SSRN 2020, 3524675. [Google Scholar] [CrossRef] [PubMed]
- Imai, N.; Cori, A.; Dorigatti, I.; Baguelin, M.; Donnelly, C.A.; Riley, S.; Ferguson, N.M. Report 3—Transmissibility of 2019-nCoV. Available online: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-3-transmissibility-of-covid-19/ (accessed on 23 March 2020).
- Lai, A.; Bergna, A.; Acciarri, C.; Galli, M.; Zehender, G. Early phylogenetic estimate of the effective reproduction number of SARS-CoV-2. J. Med. Virol. 2020, 92, 675–679. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Li, M.; Lv, G.; Lu, Z.K. Monitoring transmissibility and mortality of COVID-19 in Europe. Int. J. Infect. Dis. 2020, 95, 311–315. [Google Scholar] [CrossRef]
- Adegboye, O.A.; Adekunle, A.I.; Gayawan, E. Early Transmission Dynamics of Novel Coronavirus (COVID-19) in Nigeria. Int. J. Environ. Res. Public Health 2020, 17, 3054. [Google Scholar] [CrossRef]
- Malaysia-D-GoH KPK Press Statement 18 March 2020—Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/03/18/kenyataan-akhbar-kpk-18-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 19 March 2020).
- Zhao, S.; Zhuang, Z.; Ran, J.; Lin, J.; Yang, G.; Yang, L.; He, D. The association between domestic train transportation and novel coronavirus (2019-nCoV) outbreak in China from 2019 to 2020: A data-driven correlational report. Travel Med. Infect. Dis. 2020, 33, 101568. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore, Y.P.A.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Anthamatten, P.; Hazen, H. An Introduction to the Geography of Health, 1st ed.; Routledge: London, UK, 2011; pp. 42–45. [Google Scholar]
- Linka, K.; Peirlinck, M.; Sahli, C.F.; Kuhl, E. Outbreak dynamics of COVID-19 in Europe and the effect of travel restrictions. Comput. Methods Biomech. Biomed. Engin. 2020, 23, 710–717. [Google Scholar] [CrossRef]
- Fortaleza, C.; Guimaraes, R.B.; Catao, R.C.; Ferreira, C.P.; Berg, D.A.G.; Nogueira, V.T.; Pugliesi, E. The use of health geography modeling to understand early dispersion of COVID-19 in Sao Paulo, Brazil. PLoS ONE 2021, 16, e245051. [Google Scholar] [CrossRef]
- Zhu, M.; Shen, J.; Zeng, Q.; Tan, J.W.; Kleepbua, J.; Chew, I.; Law, J.X.; Chew, S.P.; Tangathajinda, A.; Latthitham, N.; et al. Molecular Phylogenesis and Spatiotemporal Spread of SARS-CoV-2 in Southeast Asia. Front. Public Health 2021, 9, 685315. [Google Scholar] [CrossRef]
- Adegboye, O.A.; Adekunle, A.I.; Pak, A.; Gayawan, E.; Leung, D.H.; Rojas, D.P.; Elfaki, F.; McBryde, E.S.; Eisen, D.P. Change in outbreak epicentre and its impact on the importation risks of COVID-19 progression: A modelling study. Travel Med. Infect. Dis 2021, 40, 101988. [Google Scholar] [CrossRef] [PubMed]
- Gayawan, E.; Awe, O.O.; Oseni, B.M.; Uzochukwu, I.C.; Adekunle, A.; Samuel, G.; Eisen, D.P.; Adegboye, O.A. The spatio-temporal epidemic dynamics of COVID-19 outbreak in Africa. Epidemiol. Infect. 2020, 148, e212. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus Disease 2019 (COVID-19) Situation Report—50. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200310-sitrep-50-covid-19.pdf?sfvrsn=55e904fb_2 (accessed on 28 August 2021).
- Ke, R.; Sanche, S.; Severson, E.R.; Hengartner, N. Fast spread of COVID-19 in Europe and the US and its implications: Even modest public health goals require comprehensive intervention. medRxiv 2020. preprint. [Google Scholar]
- Sun, K.; Chen, J.; Viboud, C. Early epidemiological analysis of the coronavirus disease 2019 outbreak based on crowdsourced data: A population-level observational study. Lancet Digit. Health 2020, 2, e201–e208. [Google Scholar] [CrossRef]
- Lee, P.I.; Hu, Y.L.; Chen, P.Y.; Huang, Y.C.; Hsueh, P.R. Are children less susceptible to COVID-19? J. Microbiol. Immunol. Infect. 2020, 53, 371–372. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Livingston, E.; Bucher, K. Coronavirus Disease 2019 (COVID-19) in Italy. JAMA 2020, 323, 1335. [Google Scholar] [CrossRef] [Green Version]
- Report on the Epidemiological Features of Coronavirus Disease 2019 (COVID-19) Outbreak in the Republic of Korea from January 19 to March 2, 2020. J. Korean Med. Sci. 2020, 35, e112. [CrossRef]
- Wang, Y.; Wang, Y.; Chen, Y.; Qin, Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020, 92, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Coronavirus Disease 2019 (COVID-19) Situation Report—56. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200316-sitrep-56-covid-19.pdf?sfvrsn=9fda7db2_6 (accessed on 17 March 2020).
- Indonesia-MoH Current Situation of Coronavirus Disease 2019 (COVID-19) in Indonesia. Available online: https://covid19.kemkes.go.id/situasi-infeksi-emerging/info-corona-virus/situasi-terkini-perkembangan-coronavirus-disease-covid-19-18-march-2020/ (accessed on 19 March 2020).
- Thailand-MoPH Press Statement 1 March 2020—Current Situation of Coronavirus Disease 2019 (COVID-19) in Thailand. Available online: https://pr.moph.go.th/?url=pr/detail/2/04/139295 (accessed on 2 March 2020).
- Yan, G.; Lee, C.K.; Lam, L.; Yan, B.; Chua, Y.X.; Lim, A.; Phang, K.F.; Kew, G.S.; Teng, H.; Ngai, C.H.; et al. Covert COVID-19 and false-positive dengue serology in Singapore. Lancet Infect. Dis 2020, 20, 536. [Google Scholar] [CrossRef] [Green Version]
- Webb, J.J. The historical epidemiology of global disease challenges. Lancet 2015, 385, 322–323. [Google Scholar] [CrossRef]
- Webb, J.J. Historical epidemiology and global health history. História Ciências Saúde-Manguinhos 2020, 27, 13–28. [Google Scholar] [CrossRef]
- Aspinall, E.; Curato, N.; Fossati, D.; Warburton, E.; Weiss, M.L. COVID-19 in Southeast Asia: Public Health, Social Impacts, and Political Attitudes. Available online: https://www.newmandala.org/wp-content/uploads/2021/08/SEARBO_COVID-19-in-Southeast-Asia_Public-health-social-impacts-and-political-attitudes_final.pdf (accessed on 30 August 2021).
- Chookajorn, T.; Kochakarn, T.; Wilasang, C.; Kotanan, N.; Modchang, C. Southeast Asia is an emerging hotspot for COVID-19. Nat. Med. 2021. [Google Scholar] [CrossRef]
- Asean, B.V.C. COVID-19 Situational Report in the ASEAN Region—As of July 21, 2021. Available online: https://aseanphe.org/wp-content/uploads/2021/07/COVID-19_Situational-Report_ASEAN-BioDiaspora-Regional-Virtual-Center_21July2021.pdf (accessed on 30 August 2021).
- WHO. S.A.R.O. COVID-19 Weekly Situation Report 26. Available online: https://cdn.who.int/media/docs/default-source/searo/whe/coronavirus19/sear-weekly-reports/searo-weekly-situation-report-26-2021-.pdf?sfvrsn=93e63c23_5 (accessed on 30 August 2021).
- Bian, L.; Gao, F.; Zhang, J.; He, Q.; Mao, Q.; Xu, M.; Liang, Z. Effects of SARS-CoV-2 variants on vaccine efficacy and response strategies. Expert Rev. Vaccines 2021, 20, 365–373. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Longini, I.M.; Peto, R.; Briand, S.; Heymann, D.L.; Beral, V.; Snape, M.D.; Rees, H.; Ropero, A.M.; et al. SARS-CoV-2 Variants and Vaccines. N. Engl. J. Med. 2021, 385, 179–186. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region/Subregion | Cumulative Incidence 1 (per 1,000,000 Population) | Exponential Growth Rate 2 (per Day) | Doubling Time (Day) | Basic Reproduction Number, R0 (95% Confidence Interval) |
|---|---|---|---|---|
| Southeast Asia (SEA) | 2.03 | 0.13 | 6.16 | 2.51 (2.31, 2.73) |
| Mainland SEA | 0.90 | 0.08 | 8.22 | 3.14 (2.44, 3.97) |
| Singapore | 41.87 | 0.06 | 6.81 | 1.37 (1.14, 1.63) |
| Maritime SEA | 2.14 | 0.22 | 6.68 | 4.16 (3.75, 4.61) |
| Characteristic | Total (n = 925) | Mainland SEA (n = 220) | Singapore (n = 243) | Maritime SEA (n = 462) | p-Value 1 |
|---|---|---|---|---|---|
| Age, year, median (IQR 2) | 44(31–58) | 37(29–51) | 46(34–58) | 46(32–59) | <0.001 |
| Sex, n (%) 3 Male Female | 514(55.6) | 131(59.5) | 140(57.6) | 243(52.6) | 0.188 |
| 410(44.3) | 89(40.5) | 103(42.4) | 218(47.2) | ||
| Nationality, n (%) | <0.001 | ||||
| Foreign | 168(18.2) | 67(30.5) | 69(28.4) | 32(6.9) | |
| Non-foreign | 750(81.1) | 153(69.5) | 174(71.6) | 423(91.6) | |
| Unknown | 7(0.7) | 0 | 0 | 7(1.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, M.; Kleepbua, J.; Guan, Z.; Chew, S.P.; Tan, J.W.; Shen, J.; Latthitham, N.; Hu, J.; Law, J.X.; Li, L. Early Spatiotemporal Patterns and Population Characteristics of the COVID-19 Pandemic in Southeast Asia. Healthcare 2021, 9, 1220. https://doi.org/10.3390/healthcare9091220
Zhu M, Kleepbua J, Guan Z, Chew SP, Tan JW, Shen J, Latthitham N, Hu J, Law JX, Li L. Early Spatiotemporal Patterns and Population Characteristics of the COVID-19 Pandemic in Southeast Asia. Healthcare. 2021; 9(9):1220. https://doi.org/10.3390/healthcare9091220
Chicago/Turabian StyleZhu, Mingjian, Jirapat Kleepbua, Zhou Guan, Sien Ping Chew, Joanna Weihui Tan, Jian Shen, Natthjija Latthitham, Jianxiong Hu, Jia Xian Law, and Lanjuan Li. 2021. "Early Spatiotemporal Patterns and Population Characteristics of the COVID-19 Pandemic in Southeast Asia" Healthcare 9, no. 9: 1220. https://doi.org/10.3390/healthcare9091220