
Different Roles of Telehealth and Telemedicine on Medical Tourism: An Empirical Study from Azerbaijan


 , , , and
, , , and
Abstract
:1. Introduction
2. Literature Review and Related Works
2.1. Differences between Telehealth and Telemedicine
2.2. The Role of Telehealth in Medical Tourism
2.3. The Role of Telemedicine in Medical Tourism
- (1)
- finding a professional specialist to discuss the problem; and
- (2)
- paying an amount (within a certain time period).
- (1)
- When a patient decides to pursue medical tourism, the first business process of telemedicine as it relates to medical tourism begins. The first step is to decide how to search for a location; the patient may peruse websites of companies advertising medical tourism or that of medical tourism providers themselves. Alternatively, the patient may simply browse the Internet. In such a period of development, telecommunications technologies have become an integral part of the life and work process of patients and healthcare providers. In this way, the business role of telemedicine in medical tourism includes medical tourism companies advertising on the Internet to reach and inform people all over the world, in addition to direct communications between patients and doctors before and after the tourist visit.
- (2)
- The second telemedicine process is the patient’s local physician actively attending the procedure, including making observations as a principal part of the recovery process.
- (3)
- The third telemedicine process is the follow-up. Telemedicine allows virtual face-to-face communication in which the patient can contact healthcare physicians at any time, and physicians can actively participate in post-procedure and follow-up care.
2.4. Medical Tourism in Azerbaijan
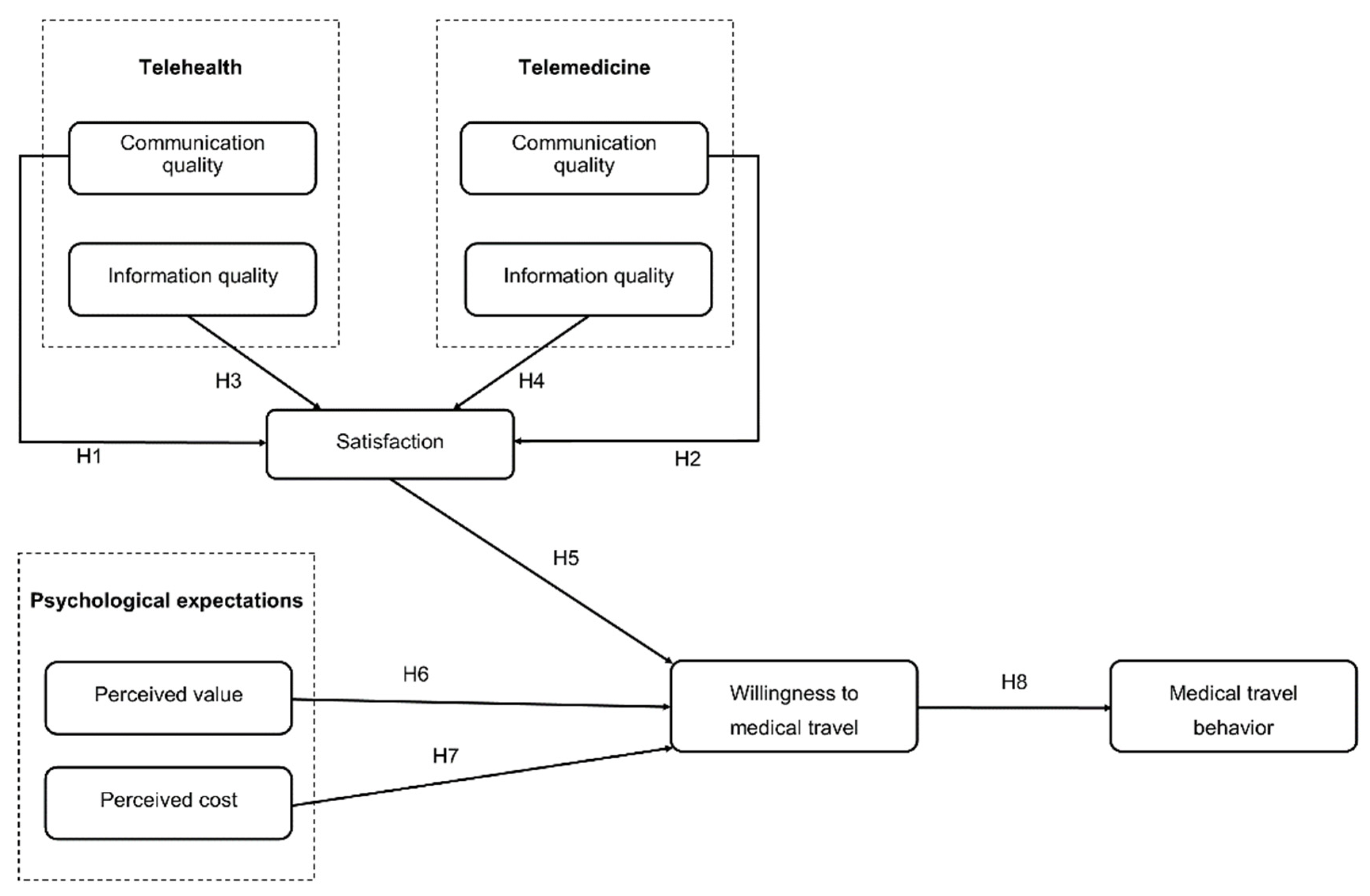
3. Research Model and Development of Hypotheses
3.1. Relationship between Communication Quality of Telehealth and of Telemedicine and Satisfaction
3.2. Relationship between Information Quality of Telehealth and of Telemedicine and Satisfaction
3.3. Satisfaction and Willingness to Undertake Medical Travel
3.4. Psychological Expectation and Willingness to Undertake Medical Travel
3.5. Willingness to Undertake Medical Travel and Medical Travel Behaviour
4. Data and Methodology
4.1. Sampling and Data Collection
4.2. Measures
5. Results
5.1. Measurement Model
5.2. Structural Model
6. Discussion and Conclusions
6.1. Theoretical and Practical Implications
6.2. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carrera, P.M.; Bridges, J.F. Globalization and healthcare: Understanding health and medical tourism. Expert Rev. Pharmacoecon. Outcomes Res. 2006, 6, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Connell, J. Medical tourism: Sea, sun, sand and surgery. Tour. Manag. 2006, 27, 1093–1100. [Google Scholar] [CrossRef]
- Lunt, N.; Carrera, P. Medical tourism: Assessing the evidence on treatment abroad. Maturitas 2010, 66, 27–32. [Google Scholar] [CrossRef] [PubMed]
- VSee. What Is Telemedicine? Available online: https://vsee.com/what-is-telemedicine/ (accessed on 10 July 2021).
- World Health Organization. Telemedicine: Opportunities and Developments in Member States. Report on the Second Global Survey on EHealth; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- CHIRON. Telemedicine vs. Telehealth: What’s the Difference? Available online: https://chironhealth.com/blog/telemedicine-vs-telehealth-whats-the-difference/ (accessed on 10 July 2021).
- Garshnek, V.; Hassell, L.H. Rethinking telemedicine evaluation for a new technological era. Int. J. Healthc. Technol. Manag. 2000, 2, 271–280. [Google Scholar] [CrossRef]
- Parajuli, R.; Doneys, P. Exploring the role of telemedicine in improving access to healthcare services by women and girls in rural Nepal. Telemat. Inform. 2017, 34, 1166–1176. [Google Scholar] [CrossRef]
- Stowe, S.; Harding, S. Telecare, telehealth and telemedicine. Eur. Geriatr. Med. 2010, 1, 193–197. [Google Scholar] [CrossRef]
- Darkins, A.; Darkins, A.W.; Cary, M.A.; Cary, M. Telemedicine and Telehealth: Principles, Policies, Performances and Pitfalls; Springer Publishing Company: New York, NY, USA, 2000. [Google Scholar]
- Hsu, W.-Y. Segmentation-based compression: New frontiers of telemedicine in telecommunication. Telemat. Inform. 2015, 32, 475–485. [Google Scholar] [CrossRef]
- Swanepoel, D.W.; Hall, J.W., III. A systematic review of telehealth applications in audiology. Telemed. E-Health 2010, 16, 181–200. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S. A DIY Guide to Telemedicine for Clinicians; Springer: Singapore, 2017. [Google Scholar]
- Brebner, J.; Brebner, E.; Ruddick-Bracken, H.; Wootton, R. The development of a pilot telemedicine network in Scotland: Lessons learned. J. Telemed. Telecare 2001, 7, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Von Wangenheim, A.; de Souza Nobre, L.F.; Tognoli, H.; Nassar, S.M.; Ho, K. User satisfaction with asynchronous telemedicine: A study of users of Santa Catarina’s system of telemedicine and telehealth. Telemed. E-Health 2012, 18, 339–346. [Google Scholar] [CrossRef]
- Binder, W.J.; Cook, J.L.; Gramze, N.; Airhart, S. Telemedicine in the intensive care unit: Improved access to care at what cost? Crit. Care Nurs. Clin. North. Am. 2018, 30, 289–296. [Google Scholar] [CrossRef] [PubMed]
- AZERNEWS. Azerbaijan in Top 5 Health Tourism Destinations. Available online: https://www.azernews.az/travel/119920.html (accessed on 10 July 2021).
- Gu, D.; Li, K.; Wang, X.; Li, X.; Liu, F.; Jiang, L.; Zhang, F. Discovering and visualizing knowledge evolution of chronic disease research driven by emerging technologies. IEEE Access 2019, 7, 72994–73003. [Google Scholar] [CrossRef]
- Perednia, D.A.; Allen, A. Telemedicine technology and clinical applications. JAMA 1995, 273, 483–488. [Google Scholar] [CrossRef]
- Gudes, O.; Kendall, E.; Yigitcanlar, T.; Pathak, V.; Baum, S. Rethinking health planning: A framework for organising information to underpin collaborative health planning. Health Inf. Manag. J. 2010, 39, 18–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glassman, D.; Puri, A.; Weingarten, S.; Hollander, J.; Stepchin, A.; Trabulsi, E.; Gomella, L. A single institution’s initial experience with telemedicine. Urol. Pract. 2017, 5, 367–371. [Google Scholar] [CrossRef]
- Nord, G.; Rising, K.L.; Band, R.A.; Carr, B.G.; Hollander, J.E. On-demand synchronous audio video telemedicine visits are cost effective. Am. J. Emerg. Med. 2019, 37, 890–894. [Google Scholar] [CrossRef]
- Wigfield, A.; Eccles, J.S. Expectancy–value theory of achievement motivation. Contemp. Educ. Psychol. 2000, 25, 68–81. [Google Scholar] [CrossRef]
- Montano, D.E.; Kasprzyk, D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In Health Behavior: Theory, Research, and Practice; Karen, G., Barbara, R., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 95–124. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Alwood, J. An activity-Based Approach to Pragmatics. In Abduction, Belief and Context in Dialogue; Studies in Computational Pragmatic; Gothenburg Papers in Theoretical Linguistics; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2000. [Google Scholar]
- Kardes, F.R.; Steckel, J.H. Consumer Behavior and Managerial Decision Making; Prentice Hall: Upper Saddle River, NJ, USA, 2002. [Google Scholar]
- Oliver, R.L.; Rust, R.T.; Varki, S. Customer delight: Foundations, findings, and managerial insight. J. Retail. 1997, 73, 311–336. [Google Scholar] [CrossRef]
- Szymanski, D.M.; Hise, R.T. E-satisfaction: An initial examination. J. Retail. 2000, 76, 309–322. [Google Scholar] [CrossRef]
- Chung, K.H.; Shin, J.I. The antecedents and consequents of relationship quality in internet shopping. Asia Pac. J. Market. Logist. 2010. [Google Scholar] [CrossRef]
- Fang, Y.H.; Chiu, C.M.; Wang, E.T. Understanding customers’ satisfaction and repurchase intentions: An integration of IS success model, trust, and justice. Internet Res. 2011. [Google Scholar] [CrossRef]
- Roca, J.C.; Chiu, C.-M.; Martínez, F.J. Understanding e-learning continuance intention: An extension of the Technology Acceptance Model. Int. J. Hum. Comput. Stud. 2006, 64, 683–696. [Google Scholar] [CrossRef] [Green Version]
- Reibstein, D.J. What attracts customers to online stores, and what keeps them coming back? J. Acad. Mark. Sci. 2002, 30, 465–473. [Google Scholar] [CrossRef]
- Mithas, S.; Ramasubbu, N.; Krishnan, M.S.; Fornell, C. Designing web sites for customer loyalty across business domains: A multilevel analysis. J. Manag. Inform. Syst. 2006, 23, 97–127. [Google Scholar] [CrossRef] [Green Version]
- Ghasemaghaei, M.; Hassanein, K. Online information quality and consumer satisfaction: The moderating roles of contextual factors–A meta-analysis. Inf. Manag. 2015, 52, 965–981. [Google Scholar] [CrossRef]
- Anderson, R.E.; Srinivasan, S.S. E-satisfaction and e-loyalty: A contingency framework. Psychol. Mark. 2003, 20, 123–138. [Google Scholar] [CrossRef]
- Lovell, N.H.; Celler, B.G. Information technology in primary health care. Int. J. Med. Inform. 1999, 55, 9–22. [Google Scholar] [CrossRef]
- Zeithaml, V.A. Consumer perceptions of price, quality, and value: A means-end model and synthesis of evidence. J. Mark. 1988, 52, 2–22. [Google Scholar] [CrossRef]
- Hellier, P.K.; Geursen, G.M.; Carr, R.A.; Rickard, J.A. Customer repurchase intention: A general structural equation model. Eur. J. Market. 2003. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.L.; Ben-Akiva, M.E. Consumer response to traveler information systems: Laboratory simulation of information searches using multimedia technology. J. Intell. Transport. Syst. 1996, 3, 1–20. [Google Scholar] [CrossRef]
- Park, J.-W.; Robertson, R.; Wu, C.-L. The effect of airline service quality on passengers’ behavioural intentions: A Korean case study. J. Air Transp. Manag. 2004, 10, 435–439. [Google Scholar] [CrossRef]
- Carpenter, J.M. Consumer shopping value, satisfaction and loyalty in discount retailing. J. Retail. Consum. Serv. 2008, 15, 358–363. [Google Scholar] [CrossRef]
- Zhang, H.; Fu, X.; Cai, L.A.; Lu, L. Destination image and tourist loyalty: A meta-analysis. Tour. Manag. 2014, 40, 213–223. [Google Scholar] [CrossRef]
- Xiao, N.; Sharman, R.; Rao, H.R.; Upadhyaya, S. Factors influencing online health information search: An empirical analysis of a national cancer-related survey. Decis. Support. Syst. 2014, 57, 417–427. [Google Scholar] [CrossRef]
- Kim, H.-W.; Xu, Y.; Koh, J. A comparison of online trust building factors between potential customers and repeat customers. J. Assoc. Inf. Syst. 2004, 5, 13. [Google Scholar] [CrossRef]
- Kim, D.J.; Steinfield, C.; Lai, Y.-J. Revisiting the role of web assurance seals in business-to-consumer electronic commerce. Decis. Support. Syst. 2008, 44, 1000–1015. [Google Scholar] [CrossRef]
- Ma, M.; Agarwal, R. Through a glass darkly: Information technology design, identity verification, and knowledge contribution in online communities. Inf. Syst. Res. 2007, 18, 42–67. [Google Scholar] [CrossRef] [Green Version]
- Flavián, C.; Guinalíu, M.; Gurrea, R. The role played by perceived usability, satisfaction and consumer trust on website loyalty. Inf. Manag. 2006, 43, 1–14. [Google Scholar] [CrossRef]
- Ravichandran, T.; Rai, A. Quality management in systems development: An organizational system perspective. MIS Q. 2000, 381–415. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, V.; Karahanna, E. The relative advantage of electronic channels: A multidimensional view. MIS Q. 2008, 179–200. [Google Scholar] [CrossRef] [Green Version]
- Luarn, P.; Lin, H.-H. Toward an understanding of the behavioral intention to use mobile banking. Comput. Hum. Behav. 2005, 21, 873–891. [Google Scholar] [CrossRef]
- Bennett, R.; Vijaygopal, R.; Kottasz, R. Willingness of people with mental health disabilities to travel in driverless vehicles. J. Transp. Health 2019, 12, 1–12. [Google Scholar] [CrossRef]
- Wu, K.-W.; Huang, S.Y.; Yen, D.C.; Popova, I. The effect of online privacy policy on consumer privacy concern and trust. Comput. Hum. Behav. 2012, 28, 889–897. [Google Scholar] [CrossRef]
- Sharma, P.; Nayak, J. The role of destination image as a mediator between tourists’ emotional experiences and behavioral intentions: A study of wellness tourism. J. Destin. Mark. Manag. 2019, 16. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Ringle, C.M.; Mena, J.A. An assessment of the use of partial least squares structural equation modeling in marketing research. J. Acad. Mark. Sci. 2012, 40, 414–433. [Google Scholar] [CrossRef]
- Ringle, C.M.; Sarstedt, M.; Straub, D.W. Editor’s comments: A critical look at the use of PLS-SEM in “MIS Quarterly”. MIS Q. 2012, 36, iii–xiv. [Google Scholar] [CrossRef] [Green Version]
- Lu, I.R.; Kwan, E.; Thomas, D.R.; Cedzynski, M. Two new methods for estimating structural equation models: An illustration and a comparison with two established methods. Int. J. Res. Mark. 2011, 28, 258–268. [Google Scholar] [CrossRef]
- Azimi, R.; Mahmoudi, G.; Esmaeili, H.-A. A study of the effect of advertising on attracting medical tourism. Int. J. Travel Med. Glob. Health 2017, 5, 89–93. [Google Scholar] [CrossRef]
- Song, K.; Choi, H.; Moon, S. A study on the U-health policy to promote medical tourism industry. Int. J. Bio-Sci. Bio-Technol. 2013, 5, 175–180. [Google Scholar]
- Goldbach, A.R.; West, D.J., Jr. Medical tourism: A new venue of healthcare. J. Glob. Bus. Issues 2010, 4, 43. [Google Scholar]
- Herrick, D.M. Medical Tourism: Global Competition in Health Care. 2007. Available online: https://www.ncpathinktank.org/pdfs/st304.pdf (accessed on 20 August 2021).
- Dávalos, M.E.; French, M.T.; Burdick, A.E.; Simmons, S.C. Economic evaluation of telemedicine: Review of the literature and research guidelines for benefit–cost analysis. Telemed. E-Health 2009, 15, 933–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Usage Technologies | Value | Timeline | Health Consultation Service Providers | |
|---|---|---|---|---|
| Telemedicine | Telecommunication technologies: videoconference; voice call; online chat | Fee/Paid | Stipulated | Professional aid: specialists/doctors |
| Telehealth | Information technologies: social websites; interviews | Free/Unpaid | Timely | Doctor interviews: knowledge/experience shared by patients with similar diseases |
| Indicator | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|---|---|---|---|
| Azerbaijan Citizens Traveling Abroad | |||||||||
| Leisure, recreation tourism (1000 people) | 729.3 | 513.1 | 897.6 | 1053.9 | 1014.7 | 1045.2 | 1096.1 | 1054.9 | 1126.3 |
| Medical tourism (1000 people) | 43.7 | 92.6 | 116.5 | 169.0 | 169.8 | 140.0 | 192.7 | 189.6 | 288.6 |
| Other purpose (1000 people) | 19.0 | 144.1 | 132.8 | 130.5 | 174.3 | 159.6 | 190.7 | 190.2 | 691.8 |
| Foreigners Traveling to Azerbaijan | |||||||||
| Leisure, recreation tourism (1000 people) | 661.7 | 519.8 | 687.8 | 705.2 | 709.9 | 668.8 | 697.1 | 839.3 | 1042.4 |
| Medical tourism (1000 people) | 14.1 | 33.3 | 43.0 | 46.2 | 46.3 | 36.5 | 41.5 | 49.1 | 63.1 |
| Other purpose (1000 people) | 46.2 | 31.7 | 38.8 | 41.8 | 42.2 | 30.8 | 39.8 | 41.6 | 45.5 |
| Category | Number (%) | |
|---|---|---|
| Gender | Male | 232 (46.4%) |
| Female | 268 (53.6%) | |
| Age | <25 years | 192 (38.4%) |
| 26–35 years | 201 (40.2%) | |
| 36–45 years | 50 (10%) | |
| 46–55 years | 36 (7.2%) | |
| 56–65 years | 15 (3%) | |
| >66 years | 6 (1.2%) | |
| Education | Junior high school or below | 17 (3.4%) |
| School | 75 (15%) | |
| High school | 249 (49.8%) | |
| Master’s degree | 117 (23.4%) | |
| PhD | 42 (8.4%) | |
| Telehealth or telemedicine user | Yes | 335 (67%) |
| No | 165 (33%) | |
| Number of times telemedicine or telehealth has been used | <5 times | 65 (13%) |
| 5–10 times | 43 (8.6%) | |
| >10 times | 227 (45.4%) | |
| Never | 165 (33%) | |
| Income (RMB) | <2000 CNY | 144 (28.8%) |
| 2000–4000 CNY | 136 (27.2%) | |
| 4000–6000 CNY | 85 (17%) | |
| 6000–8000 CNY | 53 (10.6%) | |
| 8000–10,500 CNY | 27 (5.4%) | |
| 10,500–12,500 CNY | 25 (5%) | |
| >12,500 CNY | 30 (6%) | |
| Occupation | Student | 167 (33.4%) |
| Corporate employee | 40 (8%) | |
| Civil servant | 46 (9.2%) | |
| Institution | 13 (2.6%) | |
| Freelancer | 88 (17.6%) | |
| Other | 146 (29.2%) | |
| Preferred countries for medical tourism | Turkey | 92 (18.4%) |
| Russia | 21 (4.2%) | |
| China | 114 (22.8%) | |
| United States | 57 (11.4%) | |
| Germany | 110 (22%) | |
| France | 5 (1%) | |
| United Kingdom | 9 (1.8%) | |
| Canada | 14 (2.8%) | |
| Other American countries (United States and Canada not included) | 2 (0.4%) | |
| Other Asian countries (China not included) | 15 (3%) | |
| Other European countries (Russia, Germany, France, United Kingdom and Turkey not included) | 24 (4.8%) | |
| Other | 37 (7.4%) |
| Factor | Item | Loading | Cronbach’s Alpha | Composite Reliability | AVE |
|---|---|---|---|---|---|
| Communication Quality of Telehealth | CQTh1 | 0.868 | 0.901 | 0.931 | 0.77 |
| CQTh2 | 0.889 | ||||
| CQTh3 | 0.895 | ||||
| CQTh4 | 0.858 | ||||
| Communication Quality of Telemedicine | CQTm1 | 0.867 | 0.866 | 0.909 | 0.714 |
| CQTm2 | 0.869 | ||||
| CQTm3 | 0.843 | ||||
| CQTm4 | 0.801 | ||||
| Information Quality of Telehealth | IQTh1 | 0.856 | 0.874 | 0.914 | 0.726 |
| IQTh2 | 0.84 | ||||
| IQTh3 | 0.833 | ||||
| IQTh4 | 0.879 | ||||
| Information Quality of Telemedicine | IQTm1 | 0.846 | 0.912 | 0.934 | 0.74 |
| IQTm2 | 0.872 | ||||
| IQTm3 | 0.869 | ||||
| IQTm4 | 0.863 | ||||
| IQTm5 | 0.851 | ||||
| Medical Travel Behaviour | MTB1 | 0.905 | 0.885 | 0.921 | 0.746 |
| MTB2 | 0.9 | ||||
| MTB3 | 0.886 | ||||
| MTB4 | 0.756 | ||||
| Willingness to Undertake Medical Travel | WMT1 | 0.885 | 0.825 | 0.896 | 0.741 |
| WMT2 | 0.872 | ||||
| WMT3 | 0.824 | ||||
| Perceived Cost | PC1 | 0.701 | 0.727 | 0.828 | 0.547 |
| PC2 | 0.731 | ||||
| PC3 | 0.798 | ||||
| PC4 | 0.726 | ||||
| Perceived Value | PV1 | 0.815 | 0.769 | 0.866 | 0.683 |
| PV2 | 0.823 | ||||
| PV3 | 0.842 | ||||
| Satisfaction | S1 | 0.893 | 0.891 | 0.925 | 0.754 |
| S2 | 0.903 | ||||
| S3 | 0.823 | ||||
| S4 | 0.852 |
| Construct | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Communication Quality of Telehealth | 0.878 | ||||||||
| 2. Communication Quality of Telemedicine | 0.77 | 0.845 | |||||||
| 3. Information Quality of Telehealth | 0.843 | 0.781 | 0.852 | ||||||
| 4. Information Quality of Telemedicine | 0.838 | 0.848 | 0.843 | 0.86 | |||||
| 5. Medical Travel Behaviour | 0.677 | 0.703 | 0.69 | 0.693 | 0.864 | ||||
| 6. Willingness to Undertake Medical Travel | 0.583 | 0.62 | 0.595 | 0.616 | 0.784 | 0.861 | |||
| 7. Perceived Cost | 0.595 | 0.583 | 0.608 | 0.635 | 0.595 | 0.551 | 0.74 | ||
| 8. Perceived Value | 0.766 | 0.697 | 0.768 | 0.733 | 0.755 | 0.641 | 0.605 | 0.827 | |
| 9. Satisfaction | 0.834 | 0.8 | 0.839 | 0.842 | 0.707 | 0.625 | 0.641 | 0.76 | 0.868 |
| Hypothesis Relationship | t-Value | Decision | |
|---|---|---|---|
| H1 | Communication Quality of Telehealth -> Satisfaction | 4.58 ** | Supported |
| H2 | Communication Quality of Telemedicine -> Satisfaction | 2.773 ** | Supported |
| H3 | Information Quality of Telehealth -> Satisfaction | 4.354 ** | Supported |
| H4 | Information Quality of Telemedicine -> Satisfaction | 3.043 ** | Supported |
| H5 | Satisfaction -> Willingness to Undertake Medical Travel | 3.099 ** | Supported |
| H6 | Perceived Value -> Willingness to Undertake Medical Travel | 4.863 ** | Supported |
| H7 | Perceived Cost -> Willingness to Undertake Medical Travel | 3.306 ** | Supported |
| H8 | Willingness to Undertake Medical Travel -> Medical Travel Behaviour | 31.09 ** | Supported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, D.; Humbatova, G.; Xie, Y.; Yang, X.; Zolotarev, O.; Zhang, G. Different Roles of Telehealth and Telemedicine on Medical Tourism: An Empirical Study from Azerbaijan. Healthcare 2021, 9, 1073. https://doi.org/10.3390/healthcare9081073
Gu D, Humbatova G, Xie Y, Yang X, Zolotarev O, Zhang G. Different Roles of Telehealth and Telemedicine on Medical Tourism: An Empirical Study from Azerbaijan. Healthcare. 2021; 9(8):1073. https://doi.org/10.3390/healthcare9081073
Chicago/Turabian StyleGu, Dongxiao, Gunay Humbatova, Yi Xie, Xuejie Yang, Oleg Zolotarev, and Gongrang Zhang. 2021. "Different Roles of Telehealth and Telemedicine on Medical Tourism: An Empirical Study from Azerbaijan" Healthcare 9, no. 8: 1073. https://doi.org/10.3390/healthcare9081073