
Effect of Physical Activity on Adolescent Obesity Status over Time: A Latent Growth Modeling Approach


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurements
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics of PA and Obesity Status over Time
3.2. Unconditional Models of PA and Obesity Status
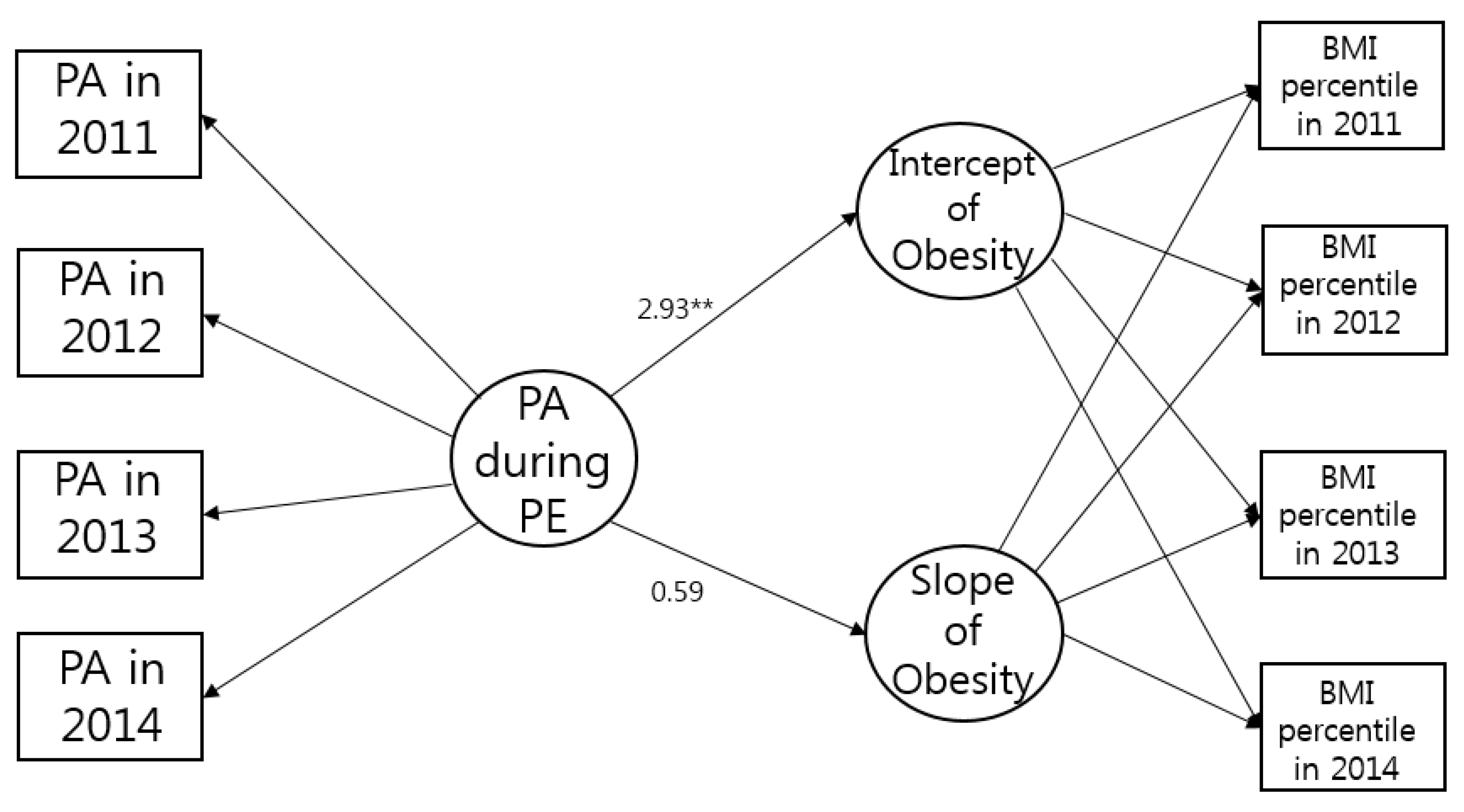
3.3. Conditional Model of Obesity Status
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.G.; Factor-Litvak, P.; Suglia, S.F.; Susser, E.S.; Kezios, K.L.; Lovasi, G.S.; Cirillo, P.M.; Cohn, B.A.; Link, B.G. Tracking of obesity in childhood into adulthood: Effects on body mass index and fat mass index at age 50. Child. Obes. 2020, 16, 226–233. [Google Scholar] [CrossRef]
- Bjerregaard, L.G.; Jensen, B.W.; Ängquist, L.; Osler, M.; Sørensen, T.I.; Baker, J.L. Change in overweight from childhood to early adulthood and risk of type 2 diabetes. N. Engl. J. Med. 2018, 378, 1302–1312. [Google Scholar] [CrossRef] [PubMed]
- Faienza, M.F.; Chiarito, M.; Molina-Molina, E.; Shanmugam, H.; Lammert, F.; Krawczyk, M.; D’Amato, G.; Portincasa, P. Childhood obesity, cardiovascular and liver health: A growing epidemic with age. World J. Pediatr. 2020, 16, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.; Danielsson, P.; Persson, M.; Marcus, C.; Hagman, E. Association of childhood obesity with risk of early all-cause and cause-specific mortality: A Swedish prospective cohort study. PLoS Med. 2020, 17, e1003078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.M.; Shiroma, E.J.; Lebelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable disease worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Gibson, L.Y.; Allen, K.L.; Davis, E.; Blair, E.; Zubrick, S.R.; Byrne, S.M. The psychosocial burden of childhood overweight and obesity: Evidence for persisting difficulties in boys and girls. Eur. J. Pediatr. 2017, 176, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Sutaria, S.; Devakumar, D.; Yasuda, S.S.; Das, S.; Saxena, S. Is obesity associated with depression in children? Systematic review and meta-analysis. Arch. Dis. Child. 2019, 104, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Noncommunicable Disease: Childhood Overweight and Obesity. Available online: https://www.who.int/news-room/q-a-detail/noncommunicable-diseases-childhood-overweight-and-obesity (accessed on 12 March 2021).
- Ash, T.; Agaronov, A.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions: A systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–12. [Google Scholar] [CrossRef]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef]
- Weihrauch-Blüher, S.; Kromeyer-Hauschild, K.; Graf, C.; Widhalm, K.; Korsten-Reck, U.; Jödicke, B.; Markert, J.; Müller, M.J.; Moss, A.; Wabitsch, M.; et al. Current guidelines for obesity prevention in childhood and adolescence. Obes. Facts 2018, 11, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Adolescent Obesity and Related Behaviours: Trends and Inequalities in the WHO European Region, 2002–2014. Available online: https://www.euro.who.int/__data/assets/pdf_file/0019/339211/WHO_ObesityReport_2017_v3.pdf (accessed on 28 June 2021).
- Buru, K.; Emeto, T.; Malau-Aduli, A.E.; Malau-Aduli, B.S. The efficacy of school-based interventions in preventing adolescent obesity in Australia. Healthcare 2020, 8, 514. [Google Scholar] [CrossRef] [PubMed]
- Cawley, J.; Frisvold, D.; Meyerhoefer, C. The impact of physical education on obesity among elementary school children. J. Health Econ. 2013, 32, 743–755. [Google Scholar] [CrossRef] [Green Version]
- Telford, R.D.; Cunningham, R.B.; Fitzgerald, R.; Olive, L.S.; Prosser, L.; Jiang, X.; Telford, R.M. Physical education, obesity, and academic achievement: A 2-year longitudinal investigation of Australian elementary school children. Am. J. Public Health 2012, 102, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Korean Children and Youth Panel Survey. Available online: https://www.nypi.re.kr/archive/board?menuId=MENU00329 (accessed on 19 March 2021).
- Growth Charts. Available online: https://knhanes.kdca.go.kr/knhanes/sub08/sub08_01.do (accessed on 25 March 2021).
- Little, T.D. Longitudinal Structural Equation Modeling; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage Publications: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled anlaysis of 298 population-based surveys with 1.6 million participants. Lancet Child. Adolesc. 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Fullmer, M.O.; Wilkinson, C.; Prusak, K.A.; Eggett, D.; Pennington, T. Adolescent activity and motivational profiles while keeping a physical activity record. J. Teach. Phys. Educ. 2018, 37, 1–11. [Google Scholar] [CrossRef]
- Schmidt, S.C.E.; Henn, A.; Albrecht, C.; Woll, A. Physical activity of German children and adolescents 2003–2012: The MoMo-study. Int. J. Envrion. Res. 2017, 13, 1375. [Google Scholar]
- Kokko, S.; Martin, L.; Geidne, S.; van Hoye, A.; Lane, A.; Meganck, J. Does sport club participation contribute to physical activity among children and adolescents? A comparison across six European countries. Scand. J. Public Health 2019, 47, 851–858. [Google Scholar] [CrossRef]
- Ward, Z.J.; Long, M.W.; Resch, S.C.; Giles, C.M.; Cradock, A.L.; Gortmaker, S.L. Simulation of growth trajectories of childhood obesity into adulthood. N. Engl. J. Med. 2017, 377, 2145–2153. [Google Scholar] [CrossRef]
- Hayes, G.; Dowd, K.P.; MacDonncha, C.; Donnelly, A.E. Tracking of physical activity and sedentary behavior from adolescence to young adulthood: A systematic literature review. J. Adolesc. Health 2019, 65, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Ekblom-Bak, E.; Ekblom, Ö.; Andersson, G.; Wallin, P.; Ekblom, B. Physical education and leisure-time physical activity in youth are both important for adulthood activity, physical performance, and health. J. Phys. Act. Health 2018, 15, 661–670. [Google Scholar] [CrossRef]
- Daly, C.M.; Foote, S.J.; Wadsworth, D.D. Physical activity, sedentary behavior, fruit and vegetable consumption and access: What influences obesity in rural children? J. Community Health 2017, 42, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Erfle, S.E.; Gamble, A. Effects of daily physical education on physical fitness and weight status in middle school adolescents. J. Sch. Health 2015, 85, 27–35. [Google Scholar] [CrossRef] [PubMed]
- So, W.Y.; Sung, D.J.; Swearingin, B.; Baek, S.I.; Rhi, S.Y.; Webb, D.; Fuller, T.M. Prevalence of obesity in Korean adolescents and its relationship with the weekly frequency of the physical education classes. J. Sports Sci. Med. 2011, 10, 679. [Google Scholar]
- Drake, K.M.; Beach, M.L.; Longacre, M.R.; MacKenzie, T.; Titus, L.J.; Rundle, A.G.; Dalton, M.A. Influence of sports, physical education, and active commuting to school on adolescent weight status. Pediatrics 2012, 130, e296–e304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahan, D.; McKenzie, T.L. The potential and reality of physical education in controlling overweight and obesity. Am. J. Public Health 2015, 105, 653–659. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; LCC BY-NC-SA 3.0 IGO. [Google Scholar]
- Lee, E.Y.; Carson, V.; Jeon, J.Y.; Spence, J.C. Prevalence of physical activity and sitting time among South Korean adolescents: Results from the Korean National Health and Nutrition Examination Survey, 2013. Asia. Pac. J. Public Health 2016, 28, 498–506. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. 1st obesity | ||||||||
| 2. 2nd obesity | 0.76 *** | |||||||
| 3. 3rd obesity | 0.69 *** | 0.76 *** | ||||||
| 4. 4th obesity | 0.65 *** | 0.74 *** | 0.82 *** | |||||
| 5. 1st PA | 0.02 | 0.03 | 0.04 | 0.03 | ||||
| 6. 2nd PA | 0.00 | 0.03 | 0.03 | 0.04 * | 0.38 *** | |||
| 7. 3rd PA | 0.08 ** | 0.10 ** | 0.09 *** | 0.08 *** | 0.28 *** | 0.31 *** | ||
| 8. 4th PA | 0.06 * | 0.08 * | 0.08 ** | 0.08 *** | 0.24 *** | 0.32 *** | 0.38 *** | |
| Mean | 38.32 | 37.55 | 41.06 | 42.38 | 2.03 | 1.95 | 1.60 | 1.49 |
| Standard deviation | 23.07 | 24.46 | 26.29 | 27.28 | 1.23 | 1.35 | 1.12 | 1.15 |
| Skewness | 0.36 | 0.49 | 0.40 | 0.39 | −0.07 | 0.13 | 0.31 | 0.47 |
| Kurtosis | −1.08 | −0.79 | −0.95 | −0.96 | −1.10 | −1.18 | 10.51 | −0.41 |
| Variables | Model | χ2 (df) | CFI | TLI | RMSEA | Intercept | Slope | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Variance | Mean | Variance | ||||||
| PA | Non | 48.44(5) *** | 0.94 | 0.92 | 0.08 | 2.03 *** | 0.45 *** | ||
| Linear | 100.11(8) *** | 0.88 | 0.91 | 0.09 | 2.06 *** | 0.68 *** | −0.59 *** | 0.36 *** | |
| Obesity Status | Non | 279.87(5) *** | 0.93 | 0.92 | 0.20 | 38.32 *** | 471.24 *** | ||
| Linear | 46.47(8) *** | 0.99 | 0.99 | 0.07 | 37.48 *** | 423.95 *** | 4.71** | 228.05 *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, S.J. Effect of Physical Activity on Adolescent Obesity Status over Time: A Latent Growth Modeling Approach. Healthcare 2021, 9, 1018. https://doi.org/10.3390/healthcare9081018
Chung SJ. Effect of Physical Activity on Adolescent Obesity Status over Time: A Latent Growth Modeling Approach. Healthcare. 2021; 9(8):1018. https://doi.org/10.3390/healthcare9081018
Chicago/Turabian StyleChung, Sophia Jihey. 2021. "Effect of Physical Activity on Adolescent Obesity Status over Time: A Latent Growth Modeling Approach" Healthcare 9, no. 8: 1018. https://doi.org/10.3390/healthcare9081018