
The Prediction Model of Medical Expenditure Appling Machine Learning Algorithm in CABG Patients


Abstract
:1. Introduction
2. Materials and Methods
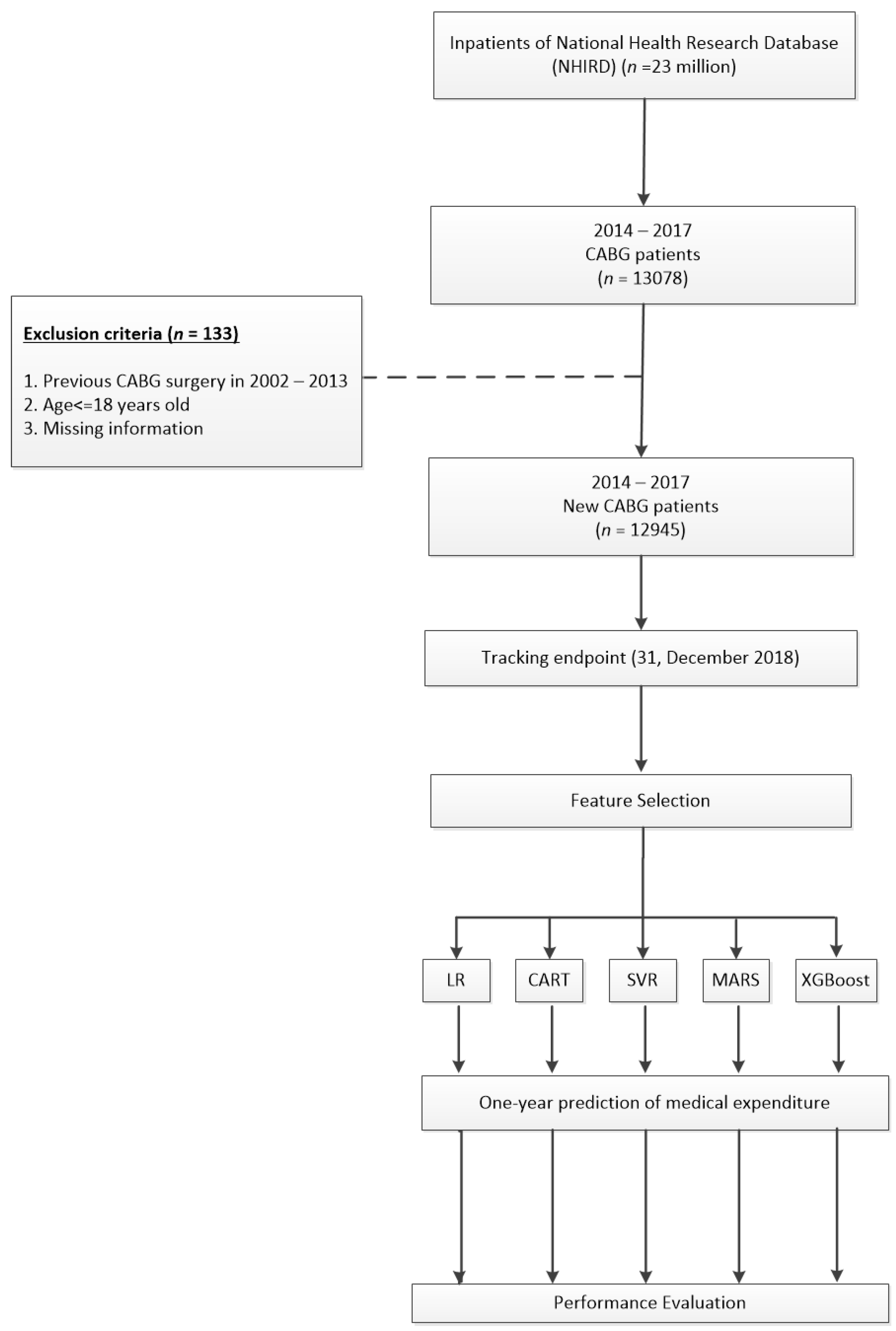
2.1. Data Source
2.2. Study Population
2.3. Comorbidities and Risk Factors
2.4. Variable and Outcome Definitions
2.5. Feature Selection and Prediction Models Implementation
2.5.1. Linear Regression (LR)
2.5.2. Classification and Regression Tree (CART)
2.5.3. Support Vector Regression (SVR)
2.5.4. Multi-variate Adaptive Regression Splines (MARS)
2.5.5. XGBoost (Extreme Gradient Boosting)
2.6. Validation Index
2.7. Statistical Analysis
2.7.1. Hardware Equipment
2.7.2. Software
3. Results
3.1. Demographic Characteristics of Study Population
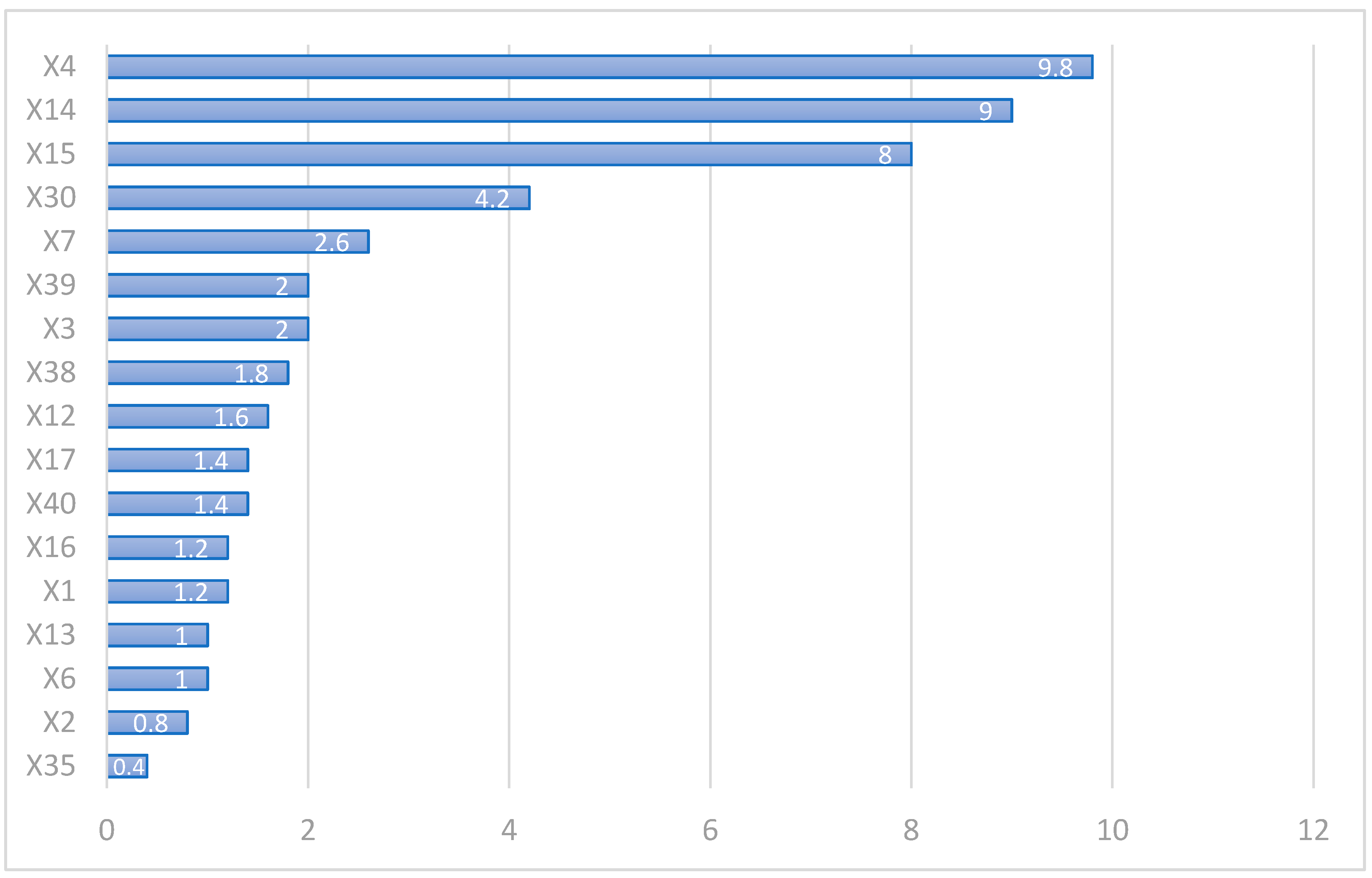
3.2. The Ranking Number of Feature Selection on CABG
3.3. Performance of 5 Different Prediction Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Febriani, V.; Lestari, D.; Mardiyati, S.; Devila, S. Predicting readmission risk after coronary artery bypass graft surgery using logistic regression model. J. Phys. Conf. Ser. 2021, 1725, 012083. [Google Scholar] [CrossRef]
- Hannan, E.L.; Racz, M.J.; Walford, G.; Ryan, T.J.; Isom, O.W.; Bennett, E.; Jones, R.H. Predictors of Readmission for Complications of Coronary Artery Bypass Graft Surgery. JAMA 2003, 290, 773–780. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.M.; Zhang, Q.; Chatterjee, S.; Cheema, F.; Loor, G.; Lemaire, S.A.; Wall, M.J.; Coselli, J.S.; Rosengart, T.K.; Ghanta, R.K. Incidence, Cost, and Risk Factors for Readmission After Coronary Artery Bypass Grafting. Ann. Thorac. Surg. 2019, 107, 1782–1789. [Google Scholar] [CrossRef] [PubMed]
- Zea-Vera, R.; Zhang, Q.; Amin, A.; Shah, R.M.; Chatterjee, S.; Wall, M.J.; Rosengart, T.K.; Ghanta, R.K. Development of a Risk Score to Predict 90-Day Readmission After Coronary Artery Bypass Graft. Ann. Thorac. Surg. 2021, 111, 488–494. [Google Scholar] [CrossRef]
- Huang, Y.-C.; Li, S.-J.; Chen, M.; Lee, T.-S.; Chien, Y.-N. Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients. Health 2021, 9, 547. [Google Scholar] [CrossRef]
- Raza, S.; Sabik, J.F.; Ainkaran, P.; Blackstone, E.H. Coronary artery bypass grafting in diabetics: A growing health care cost crisis. J. Thorac. Cardiovasc. Surg. 2015, 150, 304–312.e2. [Google Scholar] [CrossRef] [Green Version]
- Liao, K.-M.; Kuo, L.-T.; Lu, H.-Y. Hospital costs and prognosis in end-stage renal disease patients receiving coronary artery bypass grafting. BMC Nephrol. 2020, 21, 333. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Yeh, H.-Y.; Wu, J.-C.; Haschler, I.; Chen, T.-J.; Wetter, T. Taiwan’s National Health Insurance Research Database: Administrative health care database as study object in bibliometrics. Science 2011, 86, 365–380. [Google Scholar] [CrossRef]
- Tsai, M.-Y.; Hu, W.-L.; Chiang, J.-H.; Huang, Y.-C.; Chen, S.-Y.; Hung, Y.-C.; Chen, Y.-H. Improved medical expenditure and survival with integration of traditional Chinese medicine treatment in patients with heart failure: A nationwide population-based cohort study. Oncotarget 2017, 8, 90465–90476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Yang, C.; Liu, H. CHA2DS2-VASc score as predictor of ischemic stroke in patients undergoing coronary artery bypass grafting and percutaneous coronary intervention. Sci. Rep. 2017, 7, 11404. [Google Scholar] [CrossRef]
- Yin, L.; Ling, X.; Zhang, Y.; Shen, H.; Min, J.; Xi, W.; Wang, J.; Wang, Z. CHADS2 and CHA2DS2-VASc Scoring Systems for Predicting Atrial Fibrillation following Cardiac Valve Surgery. PLoS ONE 2015, 10, e0123858. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Liu, H. Feature Selection for High-Dimensional Data: A Fast Correlation-Based Filter Solution. In Proceedings of the 20th International Conference on Machine Learning (ICML-03), Washington, DC, USA, 21–24 August 2003; pp. 856–863. [Google Scholar]
- Chandrashekar, G.; Sahin, F. A survey on feature selection methods. Comput. Electr. Eng. 2014, 40, 16–28. [Google Scholar] [CrossRef]
- Kuo, C.-Y.; Yu, L.-C.; Chen, H.-C.; Chan, C.-L. Comparison of Models for the Prediction of Medical Costs of Spinal Fusion in Taiwan Diagnosis-Related Groups by Machine Learning Algorithms. Healthc. Informatics Res. 2018, 24, 29–37. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, Y.; Zhang, W.; Hu, L.; Lv, T.; Cheng, H.; Hu, Y.; Huang, J. A Risk Prediction Model of Readmission after coronary artery bypass grafting (CABG) in China. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Hamdi, T.; Ben Ali, J.; Di Costanzo, V.; Fnaiech, F.; Moreau, E.; Ginoux, J.-M. Accurate prediction of continuous blood glucose based on support vector regression and differential evolution algorithm. Biocybern. Biomed. Eng. 2018, 38, 362–372. [Google Scholar] [CrossRef]
- Friedman, J.H. Multivariate Adaptive Regression Splines. Ann. Stat. 1991, 19, 1–67. [Google Scholar] [CrossRef]
- Lee, T.S.; Dai, W.; Huang, B.L.; Lu, C.J. Data mining techniques for forecasting the medical resource consumption of patients with diabetic nephropathy. Int. J. Manag. Econ. Soc. Sci. 2017, 6, 293–306. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Dovgan, E.; Gradišek, A.; Luštrek, M.; Uddin, M.; Nursetyo, A.A.; Annavarajula, S.K.; Li, Y.-C.; Syed-Abdul, S. Using machine learning models to predict the initiation of renal replacement therapy among chronic kidney disease patients. PLoS ONE 2020, 15, e0233976. [Google Scholar] [CrossRef] [PubMed]
- Hudaverdi, T.; Akyildiz, O. Investigation of the site-specific character of blast vibration prediction. Environ. Earth Sci. 2017, 76, 138. [Google Scholar] [CrossRef]
- Popoola, S.I.; Adetiba, E.; Atayero, A.A.; Faruk, N.; Calafate, C.T. Optimal model for path loss predictions using feed-forward neural networks. Cogent Eng. 2018, 5, 5. [Google Scholar] [CrossRef]
- Rodea-Montero, E.R.; Guardado-Mendoza, R.; Rodríguez-Alcántar, B.J.; Rodríguez-Nuñez, J.R.; Núñez-Colín, C.A.; Palacio-Mejía, L.S. Trends, structural changes, and assessment of time series models for forecasting hospital discharge due to death at a Mexican tertiary care hospital. PLoS ONE 2021, 16, e0248277. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-J.; Jhou, M.-J.; Lee, T.-S.; Lu, C.-J. Hybrid Basketball Game Outcome Prediction Model by Integrating Data Mining Methods for the National Basketball Association. Entropy 2021, 23, 477. [Google Scholar] [CrossRef] [PubMed]
- Juang, W.-C.; Huang, S.-J.; Huang, F.-D.; Cheng, P.-W.; Wann, S.-R. Application of time series analysis in modelling and forecasting emergency department visits in a medical centre in Southern Taiwan. BMJ Open 2017, 7, e018628. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.S.; Li, S.J.; Jiang, Y.; Shia, B.C.; Chen, M. Cost analysis of coronary artery bypass grafting surgery under single-payer reimbursement in Taiwan. Int. J. Appl. Sci. Eng. 2020, 17, 419–428. [Google Scholar] [CrossRef]
- Hyer, J.M.; White, S.; Cloyd, J.; Dillhoff, M.; Tsung, A.; Pawlik, T.M.; Ejaz, A. Can We Improve Prediction of Adverse Surgical Outcomes? Development of a Surgical Complexity Score Using a Novel Machine Learning Technique. J. Am. Coll. Surg. 2020, 230, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baciewicz, F.A. Show me the money (cost). J. Thorac. Cardiovasc. Surg. 2018, 155, 883–884. [Google Scholar] [CrossRef] [Green Version]
- Mehaffey, J.H.; Hawkins, R.; Byler, M.; Charles, E.J.; Fonner, C.; Kron, I.; Quader, M.; Speir, A.; Rich, J.; Ailawadi, G. Cost of individual complications following coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2018, 155, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Yount, K.W.; Isbell, J.M.; Lichtendahl, C.; Dietch, Z.; Ailawadi, G.; Kron, I.L.; Kern, J.A.; Lau, C.L. Bundled Payments in Cardiac Surgery: Is Risk Adjustment Sufficient to Make It Feasible? Ann. Thorac. Surg. 2015, 100, 1646–1652. [Google Scholar] [CrossRef] [Green Version]
- Riordan, C.J.; Engoren, M.; Zacharias, A.; Schwann, T.A.; Parenteau, G.L.; Durham, S.J.; Habib, R.H. Resource Utilization in Coronary Artery Bypass Operation: Does Surgical Risk Predict Cost? Ann. Thorac. Surg. 2000, 69, 1092–1097. [Google Scholar] [CrossRef]
- Benuzillo, J.; Caine, W.; Ms, R.S.E.; Roberts, C.; Lappe, D.; Doty, J. Predicting readmission risk shortly after admission for CABG surgery. J. Card. Surg. 2018, 33, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.-T.; Chen, D.-Y.; Wu, V.C.-C.; Chou, A.-H.; Chang, S.-H.; Chu, P.-H.; Chen, S.-W. Effect of Previous Coronary Stenting on Subsequent Coronary Artery Bypass Grafting Outcomes. J. Thorac. Cardiovasc. Surg. 2020. [Google Scholar] [CrossRef]
- Alghafees, M.A.; Alsubaie, N.A.; Alsadoon, L.K.; Aljafari, S.A.; Alshehri, E.A.; Suliman, I.F. Thirty-day readmission rates and associated risk factors after coronary artery bypass grafting. J. Taibah Univ. Med Sci. 2020, 15, 292–297. [Google Scholar] [CrossRef]
- Chou, C.-L.; Hsieh, T.-C.; Wang, C.-H.; Hung, T.-H.; Lai, Y.-H.; Chen, Y.-Y.; Lin, Y.-L.; Kuo, C.-H.; Wu, Y.-J.; Fang, T.-C. Long-term Outcomes of Dialysis Patients After Coronary Revascularization: A Population-based Cohort Study in Taiwan. Arch. Med Res. 2014, 45, 188–194. [Google Scholar] [CrossRef]
- Chen, S.-W.; Chang, J.C.-H.; Lin, Y.-S.; Wu, V.C.-C.; Chen, D.-Y.; Tsai, F.-C.; Hung, M.-J.; Chu, P.-H.; Lin, P.-J.; Chen, T.-H. Effect of dialysis dependence and duration on post-coronary artery bypass grafting outcomes in patients with chronic kidney disease: A nationwide cohort study in Asia. Int. J. Cardiol. 2016, 223, 65–71. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Type of Error | Metrics | Equations | |
|---|---|---|---|
| Absolute error | MAE | Mean absolute error | |
| RMSE | Root mean square error | ||
| Scaled error | MSE | Mean square error | |
| MASE | Mean absolute scaled error | ||
| Percentage error | MAPE | Mean absolute percentage error | |
| Variables | Mean ± SD | |
|---|---|---|
| Y | One-year medical expenditure after discharge (thousand NTD$) | 906,693 ± 710,020 |
| Baseline | ||
| X1 | Age | 63.72 ± 10.65 |
| X2 | CHA2DS score | 3.29 ± 1.95 |
| X3 | CCI score | 4.23 ± 2.82 |
| Surgical variables | ||
| X4 | Surgical expenditure(thousand NTD$) | 547,037 ± 436,611 |
| X5 | Length of stay (LOS) | 20.30 ± 12.02 |
| X6 | Blood transfusion, (Bag) | 7.94 ± 9.29 |
| X7 | Mechanical ventilation, (Day) | 4.67 ± 15.55 |
| X8 | Anastomosis vessels | 2.40 ± 0.80 |
| X9 | The number of PCI vessels | 1.19 ± 0.44 |
| One year before surgery | ||
| X10 | Hospitalization | 1.02 ± 1.31 |
| X11 | ED visits | 1.27 ± 0.67 |
| X12 | Blood transfusion, (Bag) | 4.08 ± 3.89 |
| X13 | Mechanical ventilation | 4.74 ± 11.44 |
| X14 | Medical expenditure (thousand NTD$) | 169,699 ± 247,396 |
| X15 | The number of HD Dialysis | 11.96 ± 5.01 |
| X16 | The number of PD Dialysis | 10.65 ± 2.91 |
| X17 | The number of PCI vessels | 1.73 ± 1.13 |
| Comorbidities | N (%) | |
| X18 | Diabetes mellitus | 8142 (62.9) |
| X19 | Hypertension | 6370 (49.21) |
| X20 | Hyperlipidemia | 10,273 (79.36) |
| X21 | Myocardial infarct | 5132 (39.64) |
| X22 | Liver cirrhosis | 367 (2.84) |
| X23 | Congestive heart failure | 6687 (51.66) |
| X24 | Coronary artery disease | 12,047 (93.06) |
| X25 | Peripheral vascular disease | 2977 (23) |
| X26 | Acute pancreatitis | 432 (3.34) |
| X27 | Malignant dysrhythmia | 763 (5.89) |
| X28 | Atrial fibrillation | 1366 (10.55) |
| X29 | Transient ischemic attack | 4139 (31.97) |
| X30 | Chronic kidney disease | 3812 (29.45) |
| X31 | Acute coronary syndrome | 7384 (57.04) |
| X32 | Chronic obstructive pulmonary disease | 5036 (38.9) |
| X33 | Stroke | 4125 (31.87) |
| X34 | Cancer | 838 (6.47) |
| X35 | Acute kidney failure | 1514 (11.7) |
| X36 | Major bleeding | 3019 (23.32) |
| X37 | Intracranial bleeding | 357 (2.76) |
| X38 | End stage renal disease | 830 (6.41) |
| X39 | Renal disease | 3731 (28.82) |
| Baseline | ||
| X40 | Gender | |
| Male | 9917 (76.61) | |
| Female | 3028 (23.39) | |
| X41 | Major illness | 2108 (16.28) |
| Hospital Variables | ||
| X42 | Hospital Area Type | |
| Central | 1958 (15.13) | |
| Northern | 8039 (62.10) | |
| Southern | 2659 (20.54) | |
| Eastern | 289 (2.23) | |
| X43 | Hospital ownership | |
| Public | 4558 (35.21) | |
| Private | 8387 (64.79) | |
| X44 | Hospital accreditation | |
| Medical center | 8012 (61.89) | |
| Non-medcial center | 4933 (38.11) | |
| Variables | LR | SVR | CART | MARS | XGBoost | Average | |
|---|---|---|---|---|---|---|---|
| X1 | Age | 1 | 0 | 0 | 0 | 5 | 1.2 |
| X2 | CHA2DS score | 0 | 1 | 2 | 0 | 1 | 0.8 |
| X3 | CCI score | 0 | 6 | 4 | 0 | 0 | 2 |
| X30 | Chronic kidney disease | 0 | 7 | 6 | 0 | 8 | 4.2 |
| X35 | AKF | 0 | 2 | 0 | 0 | 0 | 0.4 |
| X38 | ESRD | 2 | 3 | 1 | 0 | 3 | 1.8 |
| X39 | Renal Disease | 0 | 5 | 5 | 0 | 0 | 2 |
| X44 | Major illness | 3 | 4 | 0 | 0 | 0 | 1.4 |
| Surgical variables | |||||||
| X4 | Surgical expenditure | 10 | 10 | 10 | 9 | 10 | 9.8 |
| X6 | Blood transfusion | 0 | 0 | 3 | 0 | 2 | 1 |
| X7 | Mechanical ventilation | 0 | 0 | 7 | 0 | 6 | 2.6 |
| One year before surgery | |||||||
| X12 | Blood transfusion | 4 | 0 | 0 | 0 | 4 | 1.6 |
| X13 | Mechanical ventilation | 5 | 0 | 0 | 0 | 0 | 1 |
| X14 | Medical expenditure | 8 | 9 | 9 | 10 | 9 | 9 |
| X15 | The number of HD Dialysis | 9 | 8 | 8 | 8 | 7 | 8 |
| X16 | The number of PD Dialysis | 6 | 0 | 0 | 0 | 0 | 1.2 |
| X17 | The number of PCI vessels | 7 | 0 | 0 | 0 | 0 | 1.4 |
| FS Methods | ML Method | MAE | MSE | MASE | RMSE | MAPE |
|---|---|---|---|---|---|---|
| LR (10 variables) | LR | 0.1965 | 0.0813 | 0.3120 | 0.2851 | 0.0143 |
| SVR | 0.1381 | 0.0580 | 0.2192 | 0.2407 | 0.0100 | |
| MARS | 0.1663 | 0.0591 | 0.2640 | 0.2431 | 0.0121 | |
| CART | 0.2024 | 0.0815 | 0.3214 | 0.2855 | 0.0148 | |
| XGBoost | 0.1458 | 0.0491 | 0.2315 | 0.2216 | 0.0106 | |
| SVR (10 variables) | LR | 0.1987 | 0.0743 | 0.3155 | 0.2725 | 0.0145 |
| SVR | 0.1345 | 0.0542 | 0.2136 | 0.2328 | 0.0097 | |
| MARS | 0.1652 | 0.0587 | 0.2623 | 0.2422 | 0.0120 | |
| CART | 0.2024 | 0.0815 | 0.3214 | 0.2855 | 0.0148 | |
| XGBoost | 0.1449 | 0.0491 | 0.2300 | 0.2216 | 0.0105 | |
| CART (10 variables) | LR | 0.2002 | 0.0749 | 0.3178 | 0.2738 | 0.0146 |
| SVR | 0.1354 | 0.0544 | 0.2149 | 0.2331 | 0.0098 | |
| MARS | 0.1652 | 0.0587 | 0.2623 | 0.2422 | 0.0120 | |
| CART | 0.2024 | 0.0815 | 0.3214 | 0.2855 | 0.0148 | |
| XGBoost | 0.1433 | 0.0490 | 0.2275 | 0.2214 | 0.0104 | |
| MARS (3variables) | LR | 0.2070 | 0.0794 | 0.3287 | 0.2818 | 0.0151 |
| SVR | 0.1302 | 0.0532 | 0.2067 | 0.2307 | 0.0094 | |
| MARS | 0.1667 | 0.0593 | 0.2647 | 0.2436 | 0.0121 | |
| CART | 0.2024 | 0.0815 | 0.3214 | 0.2855 | 0.0148 | |
| XGBoost | 0.1466 | 0.0499 | 0.2328 | 0.2233 | 0.0107 | |
| XGBoost (10 variables) | LR | 0.1985 | 0.0739 | 0.3151 | 0.2719 | 0.0145 |
| SVR | 0.1344 | 0.0540 | 0.2134 | 0.2324 | 0.0097 | |
| MARS | 0.1652 | 0.0586 | 0.2622 | 0.2420 | 0.0120 | |
| CART | 0.2024 | 0.0815 | 0.3214 | 0.2855 | 0.0148 | |
| XGBoost | 0.1443 | 0.0492 | 0.2292 | 0.2218 | 0.0105 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Li, S.-J.; Chen, M.; Lee, T.-S. The Prediction Model of Medical Expenditure Appling Machine Learning Algorithm in CABG Patients. Healthcare 2021, 9, 710. https://doi.org/10.3390/healthcare9060710
Huang Y-C, Li S-J, Chen M, Lee T-S. The Prediction Model of Medical Expenditure Appling Machine Learning Algorithm in CABG Patients. Healthcare. 2021; 9(6):710. https://doi.org/10.3390/healthcare9060710
Chicago/Turabian StyleHuang, Yen-Chun, Shao-Jung Li, Mingchih Chen, and Tian-Shyug Lee. 2021. "The Prediction Model of Medical Expenditure Appling Machine Learning Algorithm in CABG Patients" Healthcare 9, no. 6: 710. https://doi.org/10.3390/healthcare9060710