
Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
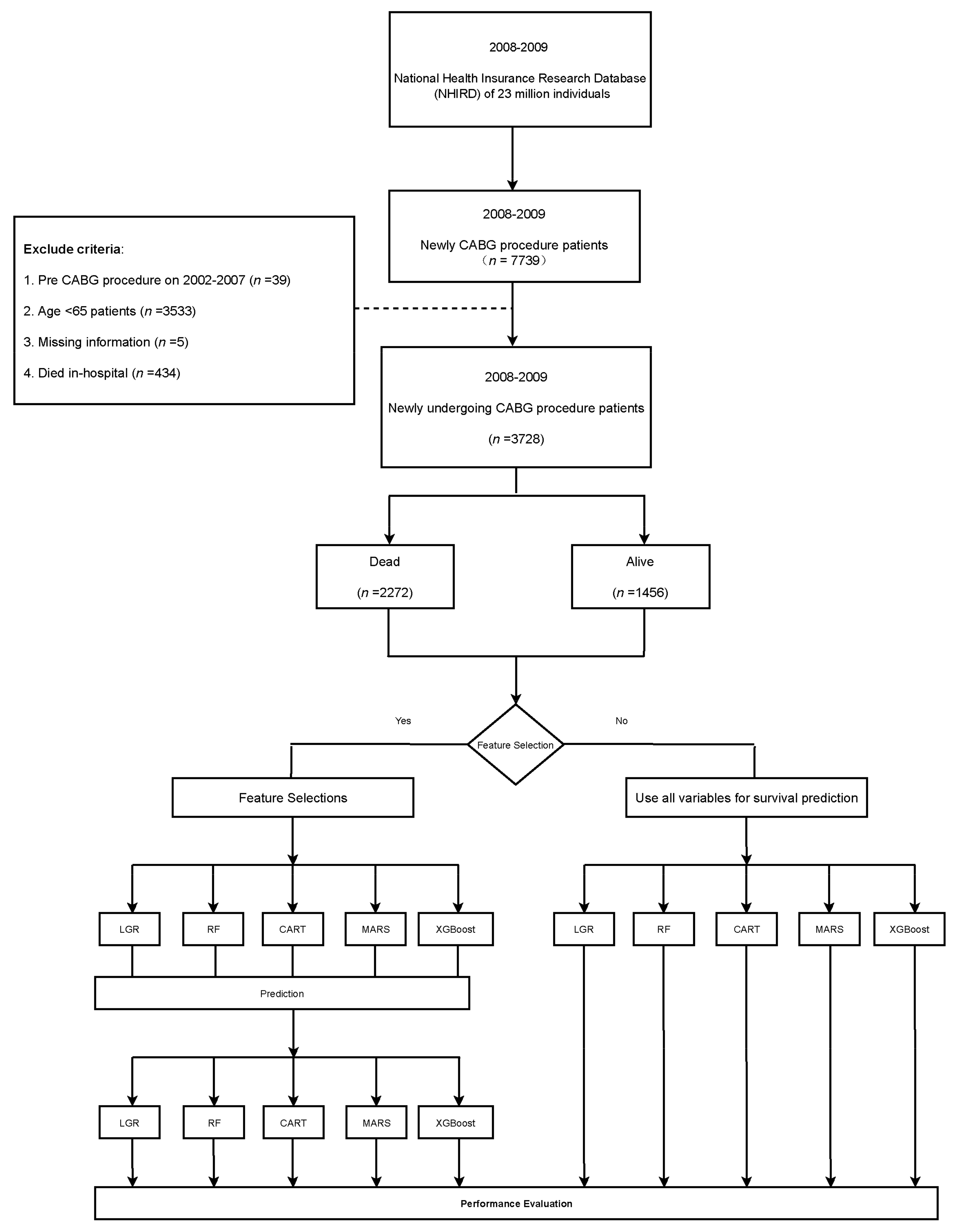
2.1. Data Source
2.2. Study Population
2.3. Comorbidities and Variable Definitions
2.4. Feature-Selection and Machine-Learning Prediction Models
2.4.1. LGR
2.4.2. RF
2.4.3. MARS
2.4.4. CART
2.4.5. XGBoost
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Study Population
3.2. Results of Feature Selection on CABG
3.3. Performance of Different Prediction Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, G.; Zhang, Y.; Zhang, W.; Hu, L.; Lv, T.; Cheng, H.; Hu, Y.; Huang, J. Risk Prediction Model of Readmission after Coronary Artery Bypass Grafting (CABG) in China. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Malmberg, M.; Gunn, J.; Rautava, P.; Sipilä, J.; Kytö, V. Outcome of Acute Myocardial Infarction Versus Stable Coronary Artery Disease Patients Treated with Coronary Bypass Surgery. Ann. Med. 2021, 53, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-C.; Chiang, J.-H.; Lay, I.-S.; Lee, Y.-C. Increased Risk of Coronary Artery Disease in People with a Previous Diagnosis of Carpal Tunnel Syndrome: A Nationwide Retrospective Population-Based Case-Control Study. BioMed Res. Int. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.-S.; Li, S.-J.; Jiang, Y.; Shia, B.-C.; Chen, M. Cost Analysis of Coronary Artery Bypass Grafting Surgery under Single-Payer Reimbursement in Taiwan. Int. J. Appl. Sci. Eng. 2020, 17, 419–428. [Google Scholar] [CrossRef]
- Chen, S.-W.; Chang, C.-H.; Lin, Y.-S.; Wu, V.C.-C.; Chen, D.-Y.; Tsai, F.-C.; Hung, M.-J.; Chu, P.-H.; Lin, P.-J.; Chen, T.-H. Effect of Dialysis Dependence and Duration on Post-Coronary Artery Bypass Grafting Outcomes in Patients with Chronic Kidney Disease: A Nationwide Cohort Study in Asia. Int. J. Cardiol. 2016, 223, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-L.; Hsieh, T.-C.; Wang, C.-H.; Hung, T.-H.; Lai, Y.-H.; Chen, Y.-Y.; Lin, Y.-L.; Kuo, C.-H.; Wu, Y.-J.; Fang, T.-C. Long-term Outcomes of Dialysis Patients After Coronary Revascularization: A Population-based Cohort Study in Taiwan. Arch. Med. Res. 2014, 45, 188–194. [Google Scholar] [CrossRef]
- Milojevic, M.; Head, S.J.; Parasca, C.A.; Serruys, P.W.; Mohr, F.W.; Morice, M.-C.; Mack, M.J.; Ståhle, E.; Feldman, T.E.; Dawkins, K.D.; et al. Causes of Death Following PCI Versus CABG in Complex CAD. J. Am. Coll. Cardiol. 2016, 67, 42–55. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kolm, P.; Grau-Sepulveda, M.V.; Ponirakis, A.; O’Brien, S.M.; Klein, L.W.; Shaw, R.E.; McKay, C.; Shahian, D.M.; Grover, F.L.; et al. Cost-Effectiveness of Revascularization Strategies. J. Am. Coll. Cardiol. 2015, 65, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.-S.; Lu, C.-W.; Chang, Y.-K.; Yang, K.-C.; Hung, S.-H.; Yang, M.-C.; Chang, H.-H.; Huang, C.-T.; Hsu, C.-C.; Huang, K.-C. Effectiveness of 23-Valent Pneumococcal Polysaccharide Vaccine on Diabetic Elderly. Medicine 2016, 95, e4064. [Google Scholar] [CrossRef]
- Tian, Y.; Yang, C.; Liu, H. CHA2DS2-VASc Score as Predictor of Ischemic Stroke in Patients Undergoing Coronary Artery Bypass Grafting and Percutaneous Coronary Intervention. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef]
- Yin, L.; Ling, X.; Zhang, Y.; Shen, H.; Min, J.; Xi, W.; Wang, J.; Wang, Z. CHADS2 and CHA2DS2-VASc Scoring Systems for Predicting Atrial Fibrillation following Cardiac Valve Surgery. PLoS ONE 2015, 10, e0123858. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.T.; Petrović, S.; Franke, K. A Comparison of Feature-Selection Methods For intrusion Detection. In Proceedings of the International Conference on Mathematical Methods, Models, and Architectures for Computer Network Security, St. Petersburg, Russia, 8–10 September 2010; pp. 242–255. [Google Scholar]
- Hu, Y.-H.; Chen, K.; Chang, I.-C.; Shen, C.-C. Critical Predictors for the Early Detection of Conversion from Unipolar Major Depressive Disorder to Bipolar Disorder: Nationwide Population-Based Retrospective Cohort Study. JMIR Med. Inform. 2020, 8, e14278. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Lee, M.T.-S.; Huang, Y.-C.; Liu, C.-K.; Li, Y.-T.; Chen, M. Prediction of Recurrence-Associated Death from Localized Prostate Cancer with a Charlson Comorbidity Index–Reinforced Machine Learning Model. Open Med. 2019, 14, 593–606. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Lin, C.-S.; Hong, C.-F.; Lee, D.-J.; Sun, C.; Lin, H.-H. Design of a Clinical Decision Support System for Predicting Erectile Dysfunction in Men Using NHIRD Dataset. IEEE J. Biomed. Health Inform. 2018, 23, 2127–2137. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Kapeleshh, K.S.; Dovgan, E.; Luštrek, M.; Gradišek Piletič, B.; Srinivasan, K.; Li, Y.-C.; Gradišek, A.; Syed-Abdul, S. Machine Learning Prediction Models for Chronic Kidney Disease using National Health Insurance Claim Data in Taiwan. medRxiv 2020. [Google Scholar] [CrossRef]
- Hosmer, J.D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Almustafa, K.M. Prediction of Heart Disease and Classifiers’ Sensitivity Analysis. BMC Bioinform. 2020, 21, 1–18. [Google Scholar] [CrossRef]
- Austin, P.C.; Ghali, W.A.; Tu, J.V. A Comparison of Several Regression Models for Analysing Cost of CABG Surgery. Stat. Med. 2003, 22, 2799–2815. [Google Scholar] [CrossRef]
- Peng, C.-Y.J.; Lee, K.L.; Ingersoll, G.M. An Introduction to Logistic Regression Analysis and Reporting. J. Educ. Res. 2002, 96, 3–14. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.-E.; Chen, H.-A.; Jhou, M.-J.; Chen, Y.-N.; Chang, T.-J.; Lu, C.-J. Evaluating the Effect of Topical Atropine Use for Myopia Control on Intraocular Pressure by Using Machine Learning. J. Clin. Med. 2020, 10, 111. [Google Scholar] [CrossRef]
- Friedman, J.H. Multivariate Adaptive Regression Splines. Ann. Stat. 1991, 19, 1–67. [Google Scholar] [CrossRef]
- Breiman, L.F.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees; Chapman and Hall: Pacific Grove, CA, USA, 1984. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA,, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Carr, B.M.; Romeiser, J.; Ruan, J.; Gupta, S.; Seifert, F.C.; Zhu, W.; Shroyer, A.L. Long-Term Post-CABG Survival: Performance of Clinical Risk Models Versus Actuarial Predictions. J. Card. Surg. 2015, 31, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, W.-H.; Chu, C.-Y.; Hsu, P.-C.; Lee, W.-H.; Su, H.-M.; Lin, T.-H.; Yen, H.-W.; Voon, W.-C.; Lai, W.-T.; Sheu, S.-H. The Effects of Secondary Prevention after Coronary Revascularization in Taiwan. PLoS ONE 2019, 14, e0215811. [Google Scholar] [CrossRef]
- Raza, S.; Sabik, J.F.; Ainkaran, P.; Blackstone, E.H. Coronary Artery Bypass Grafting in Diabetics: A Growing Health Care Cost Crisis. J. Thorac. Cardiovasc. Surg. 2015, 150, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Liao, K.-M.; Kuo, L.-T.; Lu, H.-Y. Hospital Costs and Prognosis in End-Stage Renal Disease Patients Receiving Coronary Artery Bypass Grafting. BMC Nephrol. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Fengsrud, E.; Englund, A.; Ahlsson, A. Pre- and Postoperative Atrial Fibrillation in CABG Patients have Similar Prognostic Impact. Scand. Cardiovasc. J. 2016, 51, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Pollock, B.D.; Filardo, G.; Da Graca, B.; Phan, T.K.; Ailawadi, G.; Thourani, V.; Damiano, J.R.J.; Edgerton, J.R. Predicting New-Onset Post-Coronary Artery Bypass Graft Atrial Fibrillation with Existing Risk Scores. Ann. Thorac. Surg. 2018, 105, 115–121. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | ≥65 Dead (n = 2272) | ≥65 Alive (n = 1456) | p-Value | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Sex | Female | 682 | 30.02 | 421 | 28.91 | 0.471 |
| Male | 1590 | 69.98 | 1035 | 71.09 | ||
| Age, mean (SD), y | 74.30 (5.60) | 71.27 (4.78) | <0.001 | |||
| Follow up years, Mean (SD) | 4.42(3.14) | 10.05 (0.57) | <0.001 | |||
| Follow up years, Median | 4.22 | 10.02 | - | |||
| CHA2DS score, mean (SD) | 4.21 (1.67) | 3.30 (1.57) | <0.001 | |||
| Comorbidities | ||||||
| DM | 1477 | 65.01 | 739 | 50.76 | <0.0001 | |
| Hypertension | 624 | 27.46 | 379 | 26.03 | 0.335 | |
| Hyperlipidemia | 1522 | 66.99 | 1056 | 72.53 | <0.001 | |
| MI | 1182 | 52.02 | 560 | 38.46 | <0.001 | |
| Liver cirrhosis | 50 | 2.2 | 10 | 0.69 | <0.001 | |
| CHF | 1385 | 60.96 | 563 | 38.67 | <0.001 | |
| CAD | 2222 | 97.8 | 1435 | 98.56 | 0.098 | |
| PVD | 541 | 23.81 | 248 | 17.03 | <0.0001 | |
| Acute pancreatitis | 43 | 1.89 | 21 | 1.44 | 0.301 | |
| Malignant dysrhythmia | 104 | 4.58 | 58 | 3.98 | 0.385 | |
| Intracranial bleeding | 53 | 2.33 | 14 | 0.96 | 0.002 | |
| AF | 348 | 15.32 | 159 | 10.92 | <0.001 | |
| TIA | 951 | 41.86 | 424 | 29.12 | <0.0001 | |
| CKD | 572 | 25.18 | 129 | 8.86 | <0.0001 | |
| ACS | 1490 | 65.58 | 810 | 55.63 | <0.0001 | |
| COPD | 1043 | 45.91 | 558 | 38.32 | <0.0001 | |
| Stroke | 947 | 41.68 | 423 | 29.05 | <0.0001 | |
| Cancer | 164 | 7.22 | 66 | 4.53 | <0.001 | |
| CCIS scores | 0 | 75 | 3.3 | 139 | 9.55 | <0.0001 |
| 1 | 269 | 11.84 | 330 | 22.66 | ||
| 2 | 383 | 16.86 | 362 | 24.86 | ||
| 3 | 424 | 18.66 | 239 | 16.41 | ||
| 4 | 341 | 15.01 | 165 | 11.33 | ||
| 5 | 275 | 12.1 | 115 | 7.9 | ||
| 6+ | 505 | 22.23 | 106 | 7.28 | ||
| Mean (SD) | 3.86 (2.40) | 2.59 (1.93) | <0.0001 | |||
| Surgical Variables | ||||||
| Anastomosis vessels, mean (SD) | 2.64 (0.72) | 2.79 (0.77) | <0.001 | |||
| Length of stay (LOS), mean (SD) | 25.59 (14.77) | 18.29 (9.15) | <0.001 | |||
| Blood transfusion, (Bag), mean (SD) | 10.89 (14.68) | 7.23 (5.31) | <0.001 | |||
| Mechanical ventilation, (Day), mean (SD) | 7.16 (13.90) | 2.76 (3.09) | <0.001 | |||
| Surgical cost | 611,701 (488,753) | 394,843 (165,389) | <0.001 | |||
| One Year Before Surgery | ||||||
| Outpatient visits, mean (SD) | 37.70 (23.34) | 32.36 (20.13) | <0.001 | |||
| Hospitalization, mean (SD) | 1.91 (1.34) | 1.45 (0.82) | <0.001 | |||
| ED visits, mean (SD) | 58 | 2.55 | 14 | 0.96 | <0.001 | |
| Blood transfusion, (Bag), mean (SD) | 3.83 (3.69) | 4.09 (4.87) | 0.636 | |||
| Mechanical ventilation, (Day), mean (SD) | 5.55 (13.48) | 3.93 (4.05) | 0.373 | |||
| Medical cost (related cardiology department), mean (SD) (thousand NT$) | 81,957 (107,098) | 60,969 (80,674) | <0.0001 | |||
| Medical cost (thousand NT$) | 155,186 (197087) | 91,439 (98,235) | <0.0001 | |||
| Variables | LGR (17 Variables) | RF (11 Variables) | CART (9 Variables) | MARS (7 Variables) | XGBoost (7 Variables) |
|---|---|---|---|---|---|
| Surgical Variables | |||||
| Blood transfusion, (Bag), mean | 1 | ||||
| Length of stay (LOS), mean | 4 | ||||
| Surgical cost | 3 | 1 | 1 | ||
| One Year Before Surgery | |||||
| ED visits, mean | 4 | 6 | |||
| Outpatient visits, mean | 15 | ||||
| Hospitalization, mean | 3 | ||||
| Mechanical ventilation, (Day), mean | 16 | 7 | 7 | ||
| Blood transfusion, (Bag), mean | 1 | ||||
| Medical cost | 8 | 6 | |||
| Baseline | |||||
| Age | 11 | 5 | 3 | 2 | |
| CHF | 7 | 4 | 6 | 5 | |
| CKD | 7 | ||||
| ACS | 12 | ||||
| CAD | 2 | ||||
| CCI score | 9 | 2 | 3 | ||
| COPD | 11 | ||||
| PVD | 14 | ||||
| Diabetes mellitus | 5 | 5 | |||
| Renal disease | 1 | 4 | 4 | ||
| Major illness | 8 | ||||
| Ischemic stroke | 3 | ||||
| CHA2DS2 scores | 2 | ||||
| Ulcer disease | 17 | 7 | |||
| Hypertension | 6 | ||||
| Hyperlipidemia | 2 | ||||
| AKF | 13 | ||||
| Acute pancreatitis | 10 | ||||
| Connective tissue disease | 9 | 8 | |||
| Moderate or severe renal disease | 5 | 9 | 6 | ||
| Moderate or severe liver disease | 10 | ||||
| Method | Accuracy | Kappa | Sensitivity | Specificity | AUC | |
|---|---|---|---|---|---|---|
| Overall (72 variables) | LGR | 0.7198 | 0.4427 | 0.6711 | 0.7939 | 0.7926 |
| RF | 0.7077 | 0.3965 | 0.7355 | 0.6655 | 0.7784 | |
| MARS | 0.7104 | 0.4294 | 0.6444 | 0.8108 | 0.7890 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.7225 | 0.4394 | 0.7044 | 0.7500 | 0.7934 | |
| LGR selection (17 variables) | LGR | 0.6179 | 0.2752 | 0.4888 | 0.8141 | 0.6981 |
| RF | 0.6260 | 0.2829 | 0.5177 | 0.7905 | 0.6912 | |
| MARS | 0.6219 | 0.2771 | 0.5088 | 0.7939 | 0.6917 | |
| CART | 0.5911 | 0.2292 | 0.4533 | 0.8006 | 0.6576 | |
| XGBoost | 0.6246 | 0.2845 | 0.5044 | 0.8074 | 0.6977 | |
| RF selection (11 variables) | LGR | 0.6876 | 0.3960 | 0.5866 | 0.8412 | 0.7784 |
| RF | 0.6916 | 0.3937 | 0.6244 | 0.7939 | 0.7637 | |
| MARS | 0.6890 | 0.3817 | 0.6444 | 0.7567 | 0.7675 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.6983 | 0.4161 | 0.5977 | 0.8513 | 0.7790 | |
| CART selection (9 variables) | LGR | 0.7091 | 0.4009 | 0.7311 | 0.6756 | 0.7624 |
| RF | 0.6554 | 0.3464 | 0.5200 | 0.8614 | 0.7557 | |
| MARS | 0.7091 | 0.3954 | 0.7488 | 0.6486 | 0.7653 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.7131 | 0.4062 | 0.7444 | 0.6655 | 0.7652 | |
| MARS selection (7 variables) | LGR | 0.6876 | 0.3960 | 0.5866 | 0.8412 | 0.7784 |
| RF | 0.6916 | 0.3937 | 0.6244 | 0.7939 | 0.7637 | |
| MARS | 0.6890 | 0.3817 | 0.6444 | 0.7567 | 0.7675 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.6983 | 0.4161 | 0.5977 | 0.8513 | 0.7790 | |
| XGBoost selection (7 variables) | LGR | 0.7184 | 0.4186 | 0.7444 | 0.6790 | 0.7739 |
| RF | 0.6903 | 0.3800 | 0.6600 | 0.7364 | 0.7453 | |
| MARS | 0.7131 | 0.4096 | 0.7333 | 0.6824 | 0.7683 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.7104 | 0.4212 | 0.6733 | 0.7668 | 0.7763 | |
| XGBoost selection and 3 risk factors (10 variables) | LGR | 0.6890 | 0.3937 | 0.6044 | 0.8175 | 0.7807 |
| RF | 0.7037 | 0.4008 | 0.6911 | 0.7229 | 0.7727 | |
| MARS | 0.7225 | 0.4233 | 0.7600 | 0.6665 | 0.7831 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.6970 | 0.4069 | 0.6200 | 0.8141 | 0.7845 | |
| MARS selection and 3 risk factors (10 variables) | LGR | 0.6916 | 0.3964 | 0.6155 | 0.8074 | 0.7780 |
| RF | 0.6836 | 0.3806 | 0.6088 | 0.7972 | 0.7629 | |
| MARS | 0.7024 | 0.3998 | 0.6844 | 0.7297 | 0.7722 | |
| CART | 0.6930 | 0.3360 | 0.8111 | 0.5135 | 0.7031 | |
| XGBoost | 0.7077 | 0.4190 | 0.6600 | 0.7804 | 0.7806 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Li, S.-J.; Chen, M.; Lee, T.-S.; Chien, Y.-N. Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients. Healthcare 2021, 9, 547. https://doi.org/10.3390/healthcare9050547
Huang Y-C, Li S-J, Chen M, Lee T-S, Chien Y-N. Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients. Healthcare. 2021; 9(5):547. https://doi.org/10.3390/healthcare9050547
Chicago/Turabian StyleHuang, Yen-Chun, Shao-Jung Li, Mingchih Chen, Tian-Shyug Lee, and Yu-Ning Chien. 2021. "Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients" Healthcare 9, no. 5: 547. https://doi.org/10.3390/healthcare9050547