
Shedding Light on the Direct and Indirect Impact of the COVID-19 Pandemic on the Lebanese Radiographers or Radiologic Technologists: A Crisis within Crises


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Minimal Sample Size Calculation
2.3. Questionnaire and Variables
2.4. Statistical Analysis
3. Results
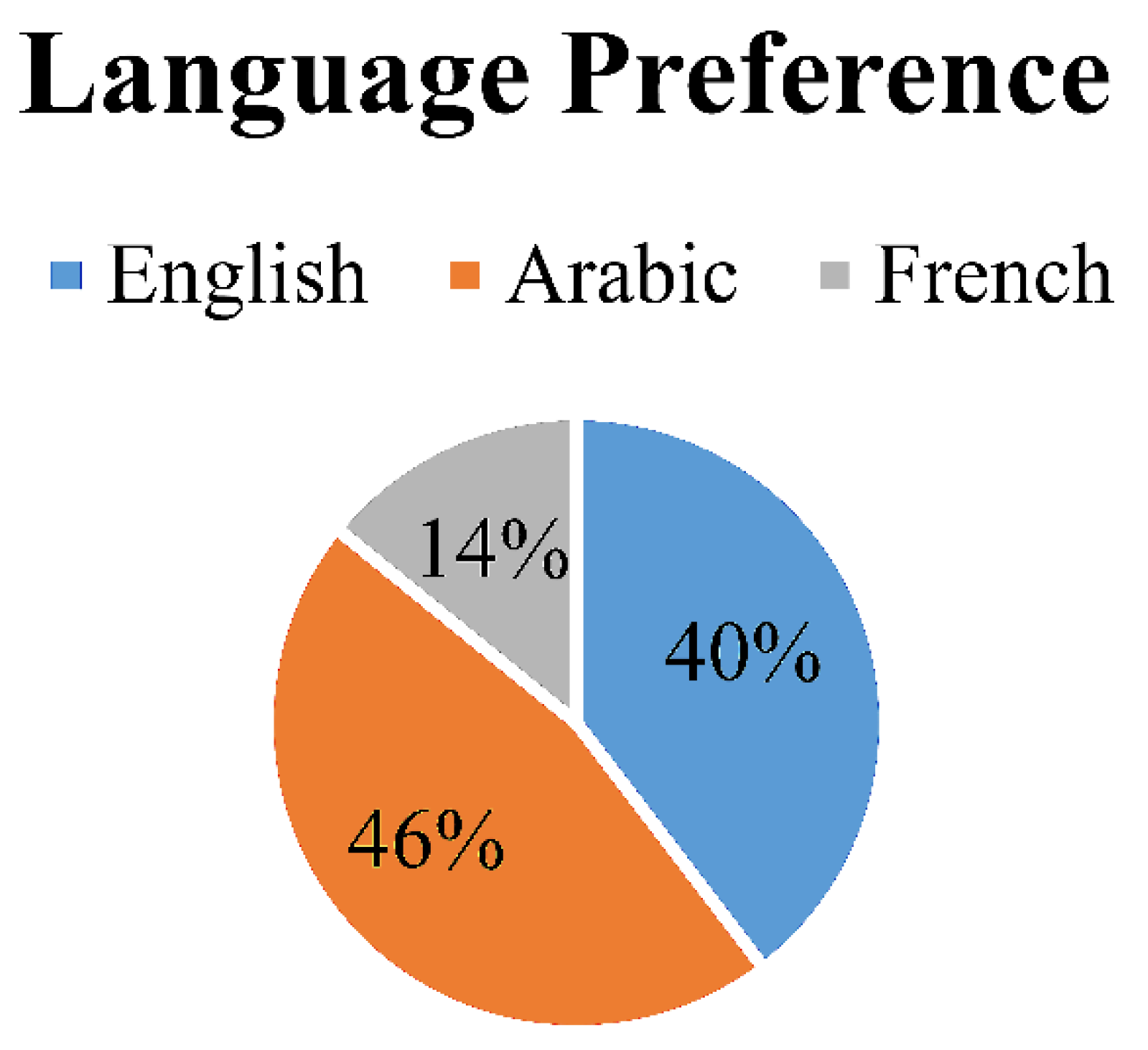
3.1. General Questions
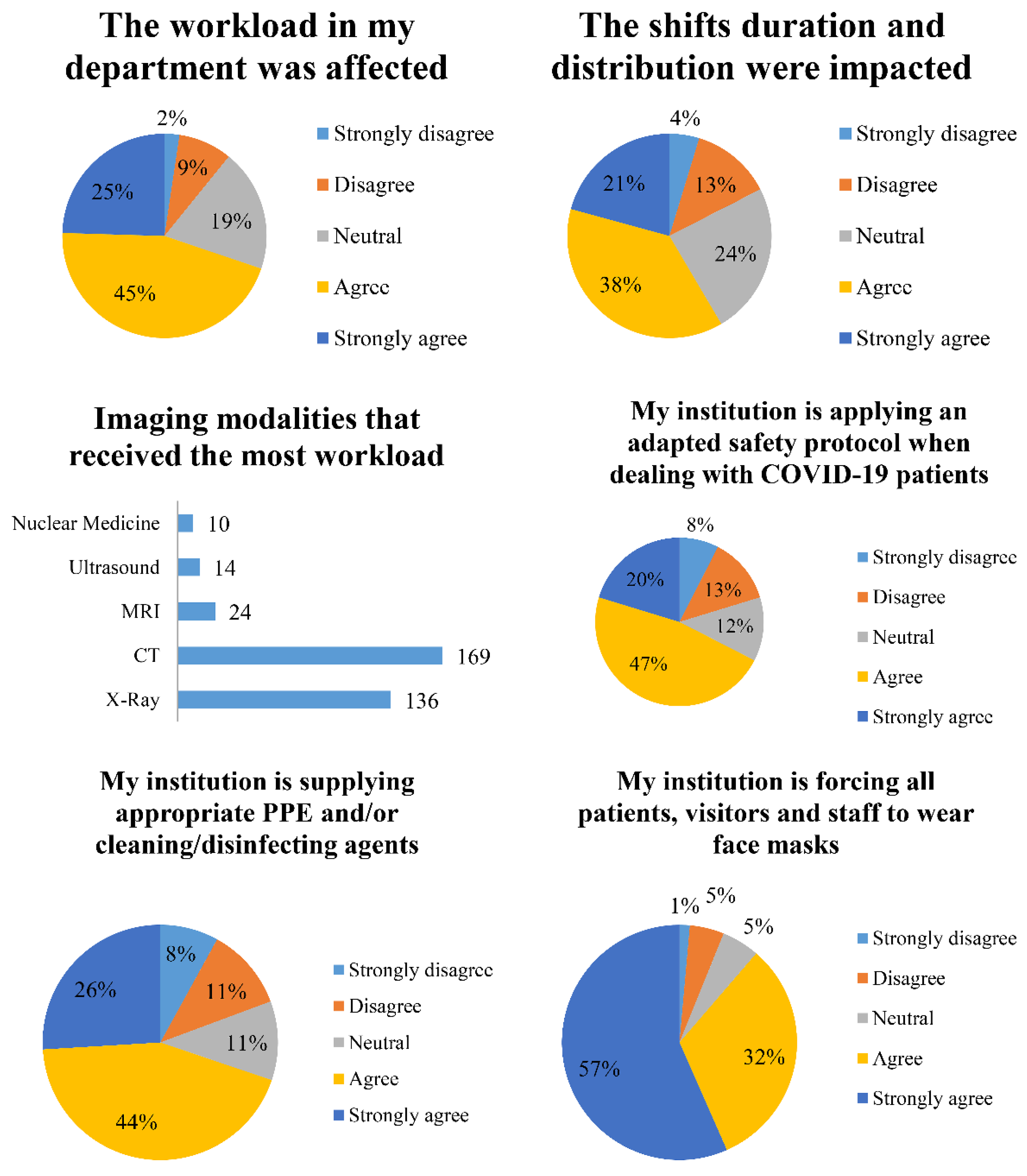
3.2. Workplace Conditions during the Pandemic
3.3. Health and Safety
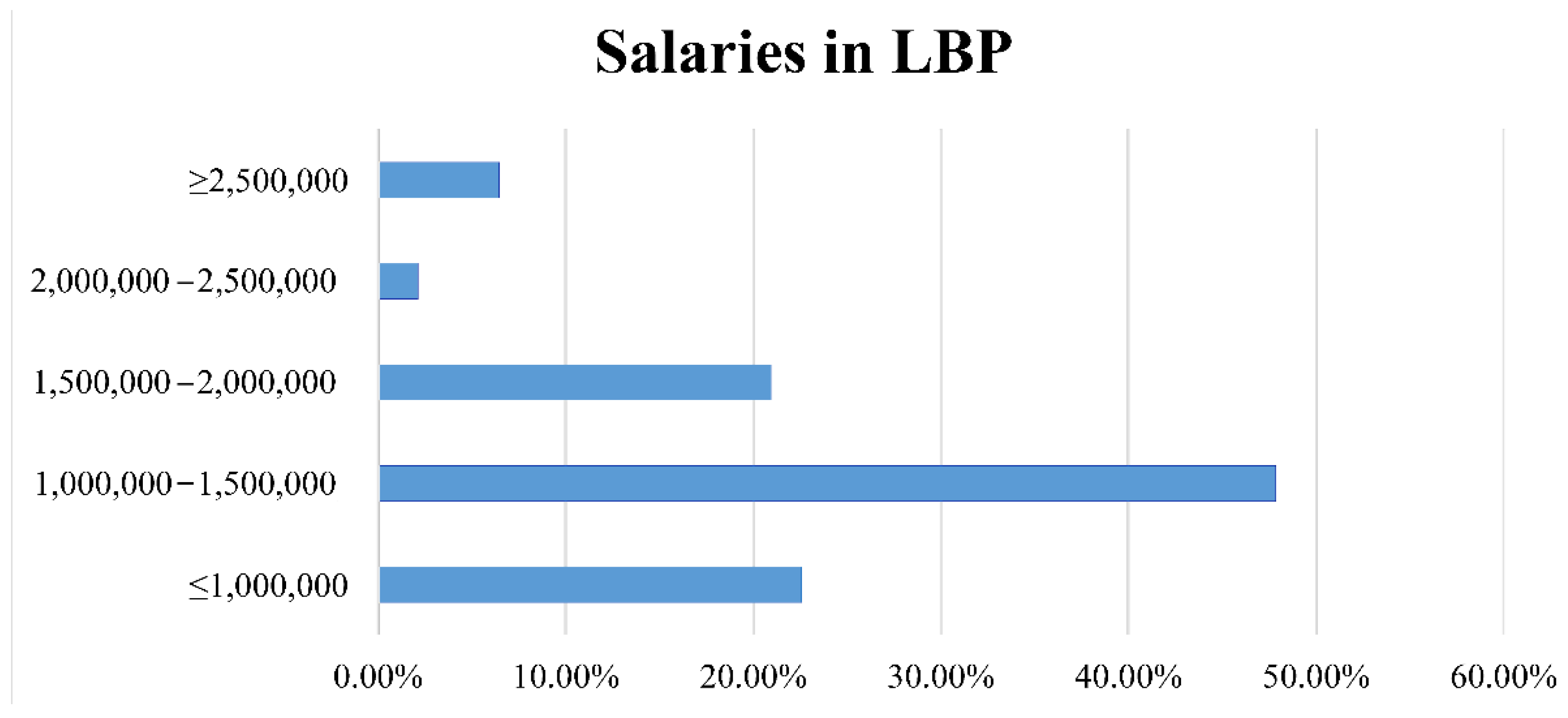
3.4. Financial Questions
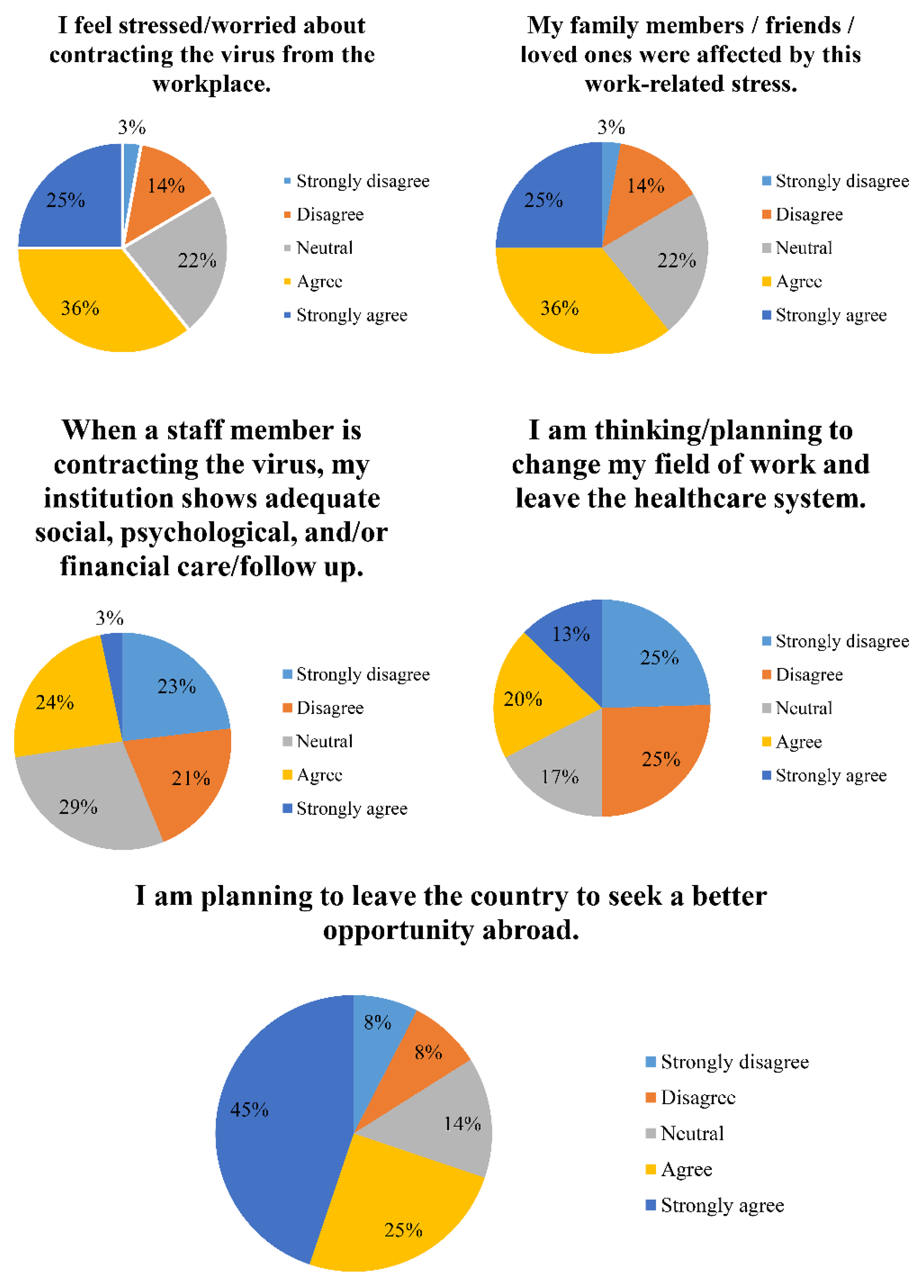
3.5. Mental/Psychological Questions
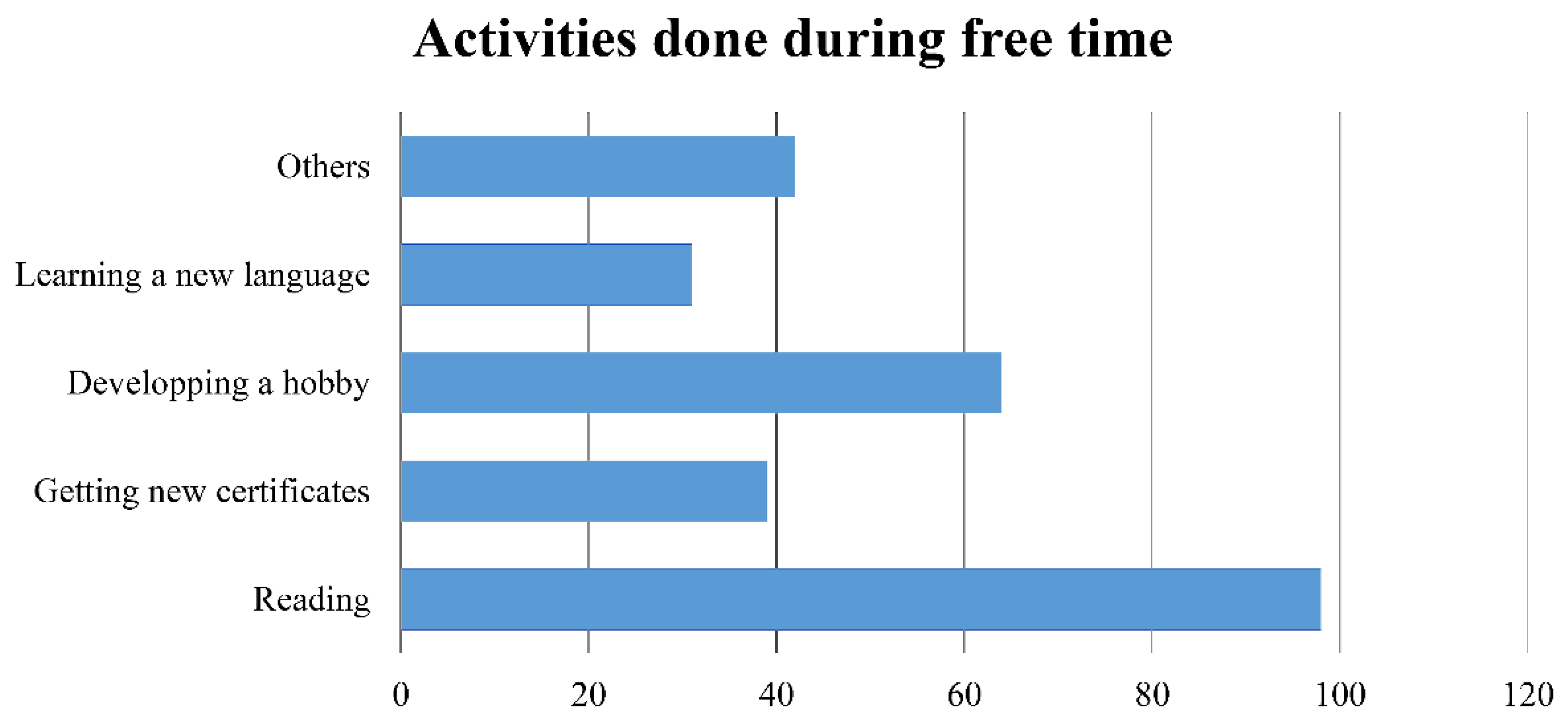
3.6. Skill/Knowledge Development
3.7. Bivariate Analysis
3.8. Multivariable Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Fani, M.; Teimoori, A.; Ghafari, S. Comparison of the COVID-2019 (SARS-CoV-2) pathogenesis with SARS-CoV and MERS-CoV infections. Future Virol. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Reports-Weekly Epidemiological Update-5 January 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Mishra, S.K.; Tripathi, T. One year update on the COVID-19 pandemic: Where are we now? Acta Trop. 2020, 214, 105778. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Andrew Rambaut, N.L.; Pybus, O.; Barclay, W.; Barrett, J.; Carabelli, A.; Connor, T.; Peacock, T.; Robertson, D.L.; Volz, E. Preliminary Genomic Characterisation of an Emergent SARS-CoV-2 Lineage in the UK Defined by a Novel Set of Spike Mutations. Available online: https://virological.org/t/preliminary-genomic-characterisation-of-an-emergent-sars-cov-2-lineage-in-the-uk-defined-by-a-novel-set-of-spike-mutations/563 (accessed on 1 February 2021).
- Volz, E.; Hill, V.; McCrone, J.T.; Price, A.; Jorgensen, D.; O’Toole, Á.; Southgate, J.; Johnson, R.; Jackson, B.; Nascimento, F.F.; et al. Evaluating the Effects of SARS-CoV-2 Spike Mutation D614G on Transmissibility and Pathogenicity. Cell 2021, 184, 64–75.e11. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Cavallo, J.J.; Forman, H.P. The Economic Impact of the COVID-19 Pandemic on Radiology Practices. Radiology 2020, 296, E141–E144. [Google Scholar] [CrossRef] [Green Version]
- Azam, S.A.; Myers, L.; Fields, B.K.K.; Demirjian, N.L.; Patel, D.; Roberge, E.; Gholamrezanezhad, A.; Reddy, S. Coronavirus disease 2019 (COVID-19) pandemic: Review of guidelines for resuming non-urgent imaging and procedures in radiology during Phase II. Clin. Imaging 2020, 67, 30–36. [Google Scholar] [CrossRef]
- Kerbage, A.; Matta, M.; Haddad, S.; Daniel, P.; Tawk, L.; Gemayel, S.; Amine, A.; Warrak, R.; Germanos, M.; Haddad, F.; et al. Challenges facing COVID-19 in rural areas: An experience from Lebanon. Int. J. Disaster. Risk Reduct. 2021, 53, 102013. [Google Scholar] [CrossRef]
- Tandon, A.; Murray, C.; Lauer, J.; Evans, D. Measuring Overall Health System Performance for 191 Countries. Available online: https://www.who.int/healthinfo/paper30.pdf (accessed on 1 February 2021).
- Miller, L.; Lu, W. These Are the Economies With the Most (and Least) Efficient Health Care. Bloomberg, 19 September 2018. [Google Scholar]
- Devi, S. Lebanon faces humanitarian emergency after blast. Lancet 2020, 396, 456. [Google Scholar] [CrossRef]
- Abouzeid, M.; Habib, R.R.; Jabbour, S.; Mokdad, A.H.; Nuwayhid, I. Lebanon’s humanitarian crisis escalates after the Beirut blast. Lancet 2020, 396, 1380–1382. [Google Scholar] [CrossRef]
- Hanke, S.H. Hanke’s Inflation Dashboard: Measurements vs. Forecasts-Lebanon Hyperinflates. Available online: https://www.cato.org/publications/commentary/hankes-inflation-dashboard-measurements-vs-forecasts (accessed on 1 February 2021).
- The United Nations Economic and Social Commission for Western Asia (ESCWA). Poverty in Lebanon: Solidarity is Vital to Address the Impact of Multiple Overlapping Shocks. Available online: https://www.unescwa.org/sites/www.unescwa.org/files/20-00268_pb15_beirut-explosion-rising-poverty-en.pdf (accessed on 1 February 2021).
- Kwee, T.C.; Kwee, R.M. Chest CT in COVID-19: What the Radiologist Needs to Know. Radiographics 2020, 40, 1848–1865. [Google Scholar] [CrossRef] [PubMed]
- Long, C.; Xu, H.; Shen, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiss, R.; Grodzki, D.M.; Horger, W.; Uder, M.; Nagel, A.M.; Bickelhaupt, S. High-performance low field MRI enables visualization of persistent pulmonary damage after COVID-19. Magn. Reson. Imaging 2020, 76, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 4080. [Google Scholar] [CrossRef] [PubMed]
- Akudjedu, T.N.; Botwe, B.O.; Wuni, A.R.; Mishio, N.A. Impact of the COVID-19 pandemic on clinical radiography practice in low resource settings: The Ghanaian radiographers’ perspective. Radiography 2020. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Epi Info™. Available online: https://www.cdc.gov/epiinfo/index.html (accessed on 1 February 2021).
- Tan, B.S.; Dunnick, N.R.; Gangi, A.; Goergen, S.; Jin, Z.-Y.; Neri, E.; Nomura, C.H.; Pitcher, R.D.; Yee, J.; Mahmood, U. RSNA International Trends: A Global Perspective on the COVID-19 Pandemic and Radiology in Late 2020. Radiology 2020, 204267. [Google Scholar] [CrossRef]
- Shi, J.; Giess, C.S.; Martin, T.; Lemaire, K.A.; Curley, P.J.; Bay, C.; Mayo-Smith, W.W.; Boland, G.W.; Khorasani, R. Radiology Workload Changes During the COVID-19 Pandemic: Implications for Staff Redeployment. Acad. Radiol. 2021, 28, 1–7. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement From the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef]
- Yu, J.; Ding, N.; Chen, H.; Liu, X.-J.; He, W.-j.; Dai, W.-c.; Zhou, Z.-G.; Lin, F.; Pu, Z.-h.; Li, D.-f.; et al. Infection Control against COVID-19 in Departments of Radiology. Acad. Radiol. 2020, 27, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Foley, S.J.; O’Loughlin, A.; Creedon, J. Early experiences of radiographers in Ireland during the COVID-19 crisis. Insights Imaging 2020, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Choices and Percentages | ||||
|---|---|---|---|---|---|
| Age | 20–29 47.17% | 30–39 31.13% | 40–49 11.79% | 50–59 8.02% | 60+ 1.89% |
| Gender | Males 51.42% | Females 48.58% | |||
| Marital Status | Single 38.21% | Engaged 8.02% | Married 52.36% | Divorced 1.41% | |
| Highest Degree | T.S./L.T. 36.32% | Diploma 16.98% | B.S. 33.96% | M.S. 8.02% | Others 4.72% |
| Work Location | Private Hospital 71.23% | Public Hospital 10.85% | Lab/Medical Imaging Center 14.62% | Others 3.30% | |
| Question | Choices and Percentages | ||||
|---|---|---|---|---|---|
| My institution is providing regular/periodic, free PCR testing for staff. | Strongly Disagree 39.15% | Disagree 25.00% | Neutral 9.91% | Agree 16.04% | Strongly Agree 9.90% |
| Have you contracted the virus? | Yes 12.26% | No 74.53% | I am not sure 13.21% | ||
| Is it from the workplace? | Yes 61.54% | No 11.54% | I am not sure 26.92% | ||
| What was the severity of the disease? | No symptoms 7.69% | Mild symptoms 34.62% | Moderate symptoms 30.77% | Severe symptoms 26.92% | |
| Were you admitted to the hospital? | Yes 8.02% | No 25.94% | |||
| Did you transmit the virus to any family member/friend/colleague? | Yes 30.77% | No 50.00% | I am not sure 19.23% | ||
| Question | Choices and Percentages | ||||
|---|---|---|---|---|---|
| To what extent did the institution modify/decrease the monthly salary provided to you in accordance with the economic situation? | Severely (>50% reduction) 6.13% | Moderately (25–50% reduction) 24.06% | No Change 60.85% | My salary was modified but what was reduced will be paid later on 4.72% | I am not getting paid my monthly salary 4.24% |
| I am considering leaving job/staying home, as it is not worth it. | Strongly Disagree 24.69% | Disagree 36.42% | Neutral 3.09% | Agree 25.31% | Strongly Agree 10.49% |
| Variable | Stress/Worry about Contracting COVID-19 from the Workplace | p | ||
|---|---|---|---|---|
| Neutral | Strongly Disagree/Disagree | Agree/Strongly Agree | ||
| Age categories (in years) | 0.145 | |||
| 20–29 | 27 (26.5%) | 22 (21.6%) | 53 (52.0%) | |
| 30–39 | 16 (24.2%) | 9 (13.6%) | 41 (62.1%) | |
| 40–49 | 4 (16.0%) | 3 (12.0%) | 18 (72.0%) | |
| 50 and above | 1 (4.8%) | 3 (14.3%) | 17 (81.0%) | |
| Gender | 0.238 | |||
| Male | 29 (26.6%) | 20 (18.3%) | 60 (55.0%) | |
| Female | 19 (18.1%) | 17 (16.2%) | 69 (65.7%) | |
| Marital status | 0.841 | |||
| Single/engaged/divorced | 25 (24.3%) | 17 (16.5%) | 61 (59.2%) | |
| Married | 23 (20.7%) | 20 (18.0%) | 68 (61.3%) | |
| Workload affected by the pandemic | 0.034 | |||
| Strongly disagree/disagree | 12 (29.3%) | 6 (14.6%) | 23 (56.1%) | |
| Neutral | 0 (0%) | 5 (21.7%) | 18 (78.3%) | |
| Agree/strongly agree | 36 (24.0%) | 26 (17.3%) | 88 (58.7%) | |
| Shift duration distribution impacted during the pandemic | 0.204 | |||
| Strongly disagree/disagree | 12 (23.5%) | 4 (7.8%) | 35 (68.6%) | |
| Neutral | 8 (21.6%) | 5 (13.5%) | 24 (64.9%) | |
| Agree/strongly agree | 28 (22.2%) | 28 (22.2%) | 70 (55.6%) | |
| Institution applies adapted safety protocol | 0.268 | |||
| Strongly disagree/disagree | 4 (15.4%) | 2 (7.7%) | 20 (76.9%) | |
| Neutral | 8 (18.6%) | 6 (14.0%) | 29 (67.4%) | |
| Agree/strongly agree | 36 (24.8%) | 29 (20.0%) | 80 (55.2%) | |
| Institution supplying cleaning agents | 0.224 | |||
| Strongly disagree/disagree | 4 (17.4%) | 4 (17.4%) | 15 (65.2%) | |
| Neutral | 6 (14.6%) | 4 (9.8%) | 31 (75.6%) | |
| Agree/strongly agree | 38 (25.3%) | 29 (19.3%) | 83 (55.3%) | |
| Institution forces mask wearing | 0.083 | |||
| Strongly disagree/disagree | 4 (36.4%) | 0 (0%) | 7 (63.6%) | |
| Neutral | 0 (0%) | 2 (15.4%) | 11 (84.6%) | |
| Agree/strongly agree | 44 (23.2%) | 35 (18.4%) | 111 (58.4%) | |
| Stress/Worry About Contracting COVID-19 from the Workplace (Agree/Strongly Agree vs. Neutral) | |||
|---|---|---|---|
| Variable | aOR | p | 95% CI |
| Age categories (in years) | 0.182 | ||
| 20–29 | 1 | ||
| 30–39 | 1.28 | 0.531 | 0.59–2.79 |
| 40–49 | 1.69 | 0.407 | 0.49–5.81 |
| 50 and above | 9.53 | 0.036 | 1.16–78.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Itani, R.; Alnafea, M.; Tannoury, M.; Hallit, S.; Al Faraj, A. Shedding Light on the Direct and Indirect Impact of the COVID-19 Pandemic on the Lebanese Radiographers or Radiologic Technologists: A Crisis within Crises. Healthcare 2021, 9, 362. https://doi.org/10.3390/healthcare9030362
Itani R, Alnafea M, Tannoury M, Hallit S, Al Faraj A. Shedding Light on the Direct and Indirect Impact of the COVID-19 Pandemic on the Lebanese Radiographers or Radiologic Technologists: A Crisis within Crises. Healthcare. 2021; 9(3):362. https://doi.org/10.3390/healthcare9030362
Chicago/Turabian StyleItani, Rasha, Mohammed Alnafea, Maya Tannoury, Souheil Hallit, and Achraf Al Faraj. 2021. "Shedding Light on the Direct and Indirect Impact of the COVID-19 Pandemic on the Lebanese Radiographers or Radiologic Technologists: A Crisis within Crises" Healthcare 9, no. 3: 362. https://doi.org/10.3390/healthcare9030362