Relationship between Sleep Duration Trajectories and Self-Rated Depressive Symptoms in South Koreans with Physical Disabilities


Abstract
:1. Introduction
2. Methods
2.1. Study Sample and Design
2.2. Independent Variables
2.3. Dependent Variables
Self-Rated Depressive Symptoms
2.4. Control Variables
2.5. Analytical Approach and Statistics
3. Results
3.1. Prevalence of Self-Rated Depressive Symptoms
3.2. Association between Sleep Duration and Depression among Physically Disabled People
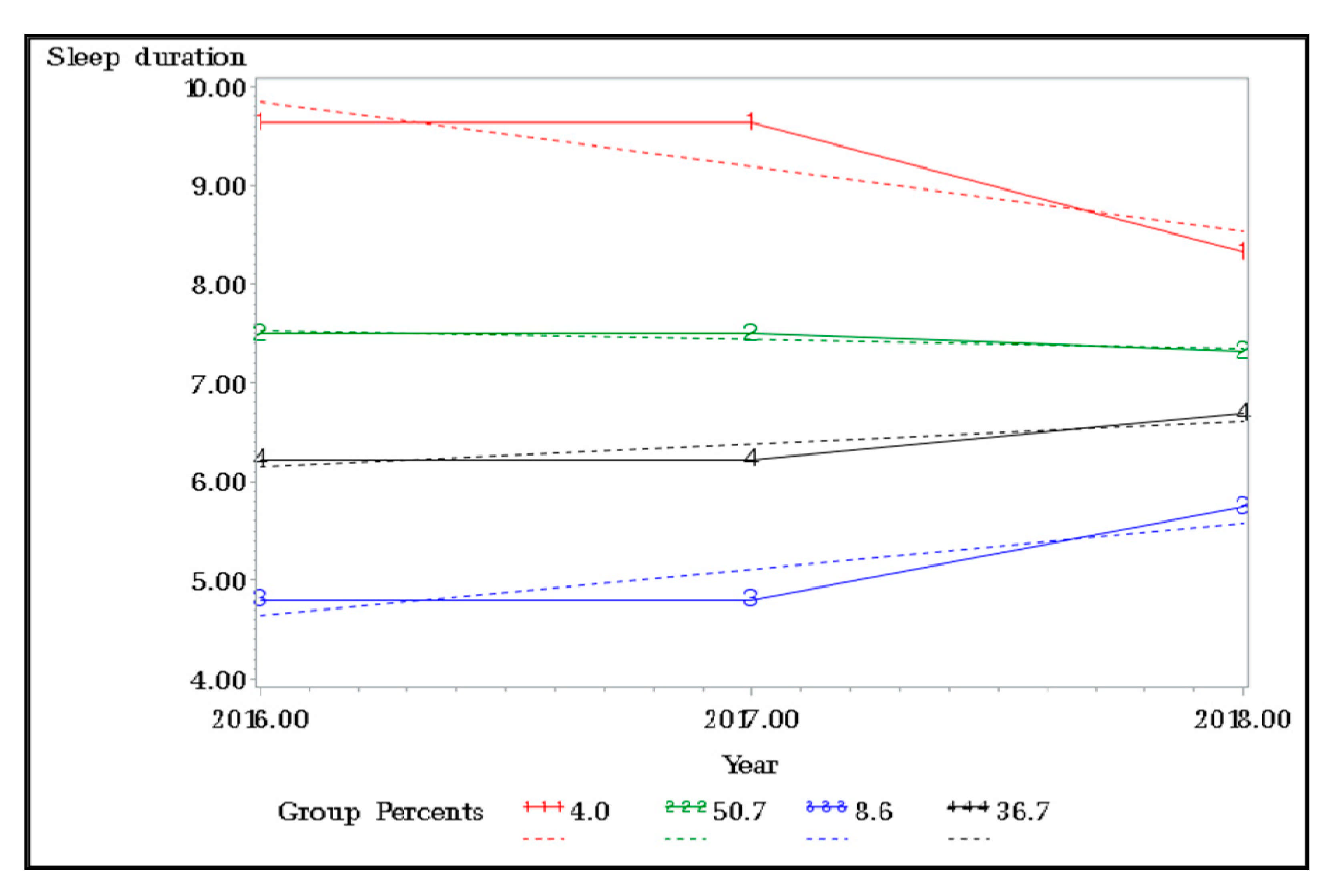
3.3. Changes in Sleep Duration over Time and Self-Rated Depressive Symptoms among the Physical Disabled
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). World Report on Disability. Available online: https://www.who.int/teams/noncommunicable-diseases/disability-and-rehabilitation/world-report-on-disability (accessed on 5 January 2021).
- Korea Employment Agency for Person with Disabilities. 2020 Statistics for the Disabled. Available online: https://www.kead.or.kr/common/comm_board_v.jsp?no=435&gotopage=1&search=4&keyword=&data_gb=007&branch_gb=B01&station_gb=000&main=4&sub1=4&sub2=0&sub3=0&option (accessed on 5 January 2021).
- Kim, Y.M.; Kim, H.R.; Choi, H.C. A longitudinal relationship between perceived social support and depressive symptoms of adults with physical disabilities. Korean J. Phys. Mult. Health Disabil. 2019, 62, 103–121. [Google Scholar] [CrossRef]
- Lee, E.W.; Song, J.Y. Factors influencing mental health status of person with physical disabilities. J. Korea Entertain. Ind. Assoc. 2019, 13, 287–295. [Google Scholar] [CrossRef]
- Won, Y.; Kim, J.T. The mediating effects of sport attitude on the relationship between the sense of loss and health promoting behaviors of persons with physical disabilities. Korean J. Phys. Educ. 2019, 58, 273–281. [Google Scholar] [CrossRef]
- National Rehabilitation Center. Healthcare for the Disabled. Available online: http://www.nrc.go.kr/research/board/boardView.do?bn=newsView&fno=37&menu_cd=05_02_00_01&no=16219&bno=16219&board_id=NRC_NOTICE_BOARD (accessed on 5 January 2021).
- Aitken, Z.; Simpson, J.A.; Gurrin, L.; Bentley, R.; Kavanagh, A.M. Do material, psychosocial and behavioural factors mediate the relationship between disability acquisition and mental health? A sequential causal mediation analysis. Int. J. Epidemiol. 2018, 47, 829–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavanagh, A.M.; Aitken, Z.; Baker, E.; LaMontagne, A.D.; Milner, A.; Bentley, R. Housing tenure and affordability and mental health following disability acquisition in adulthood. Soc. Sci. Med. 2016, 151, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. The National Survey of the Disabled Persons. 2017. Available online: http://www.mohw.go.kr/react/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=032901&CONT_SEQ=345972 (accessed on 5 January 2021).
- Disability World. Mental Issues of People with Disabilities. Available online: https://www.disabled-world.com (accessed on 5 January 2021).
- Bhattacharjee, A.; Chhetri, K. Who is more depreesed? A study among persons with disability. Indian J. Health Wellbeing 2014, 5, 1339–1341. [Google Scholar]
- Gu, S.S. The effect of discrimination experiences on depression in individual with disabilities: Focused on the moderating effect of social support. Korean J. Phys. Mult. Health Disabil. 2018, 61, 67–90. [Google Scholar] [CrossRef]
- Yoo, C. 10-Year trajectories of depressive symptoms and their predictors: Inequity between people with and without disabilities. Health Soc. Welf. Rev. 2017, 37, 150–183. [Google Scholar] [CrossRef]
- Choi, H.C. Predictors of depression trajectories in people with physical disabilities. Korean J. Phys. Mult. Health Disabil. 2020, 63, 43–64. [Google Scholar] [CrossRef]
- Choi, H.C. Reciprocal relationships between self-esteem and depressive symptoms in adults with physical disabilities. J. Phys. Mult. Health Disabil. 2019, 62, 55–74. [Google Scholar] [CrossRef]
- Im, W.G.; Hwang, S.H. Investigation of the causes of suicidal ideation of persons with severe disabilities living in S-gu-focusing on their daily activities, experience of committing suicide, and depression. Korean J. Stress Res. 2014, 22, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Kang, H.J.; Kim, J.Y. Anxiety, depression and school adaptability of university students with disabilities. J. Spec. Educ. Theory Pract. 2007, 8, 461–476. [Google Scholar]
- Kwon, T.Y. Socioeconomic status and the trajectory in depressive symptoms: The mediating role of alcohol use. Korean J. Health Educ. Promot. 2012, 29, 59–72. [Google Scholar]
- Park, H.S. A study on the influence of stress, depression, and suicide ideation by adults person with disability. Asia-Pac. J. Multimed. Serv. Converg. Art Humanit. Sociol. 2018, 8, 627–635. [Google Scholar] [CrossRef]
- Bea, S.S. Relationships between sleep duration and depression or suicidal thoughts in Korean adults. Korean J. Health Serv. Manag. 2018, 12, 219–228. [Google Scholar] [CrossRef]
- Kim, S.J. Recent Advances in diagnosis and treatment of sleep disorders. J. Korean Neuropsychiatr. Assoc. 2020, 59, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Shandra, C.L.; Kruger, A.; Hale, L. Disability and sleep duration: Evidence from the American time use survey. Disabil. Health J. 2014, 7, 325–334. [Google Scholar] [CrossRef]
- Fang, H.; Tu, S.; Sheng, J.; Shao, A. Depression in sleep disturbance: A review on a bidirectional relationship, mechanisms and treatment. J. Cell. Mol. Med. 2019, 23, 2324–2332. [Google Scholar] [CrossRef] [Green Version]
- Vgontzas, A.N.; Liao, D.; Pejovic, S.; Calhoun, S.; Karataraki, M.; Basta, M.; Ferna dez-Mendoza, J.; Bixler, E.O. Insomnia with short sleep duration and mortality: The Penn State cohort. Sleep 2010, 33, 1159–1164. [Google Scholar] [CrossRef]
- Watson, N.F.; Harden, K.P.; Buchwald, D.; Vitiello, M.V.; Pack, A.I.; Strachan, E.; Goldberg, J. Sleep duration and depressive symptoms: A gene-environment interaction. Sleep 2014, 37, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.; Kim, C.T. Effect of employment status and sleep duration on depression and suicidal ideation. Korean Public Health Res. 2019, 45, 91–103. [Google Scholar] [CrossRef]
- Hwang, E.; Park, M. The association between total sleep time and suicidal ideation in adults over the age of 20. J. Korea Contents Assoc. 2016, 16, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Okoro, C.A.; Courtney-Long, E.; Cyrus, A.C.; Zhao, G.; Wheaton, A.G. Self-reported short sleep duration among US adults by disability status and functional disability type: Results from the 2016 behavioral risk factor surveillance system. Disabil. Health J. 2020, 13. [Google Scholar] [CrossRef]
- Choi, S.J.; Park, E. The association of sleep duration and hypertension in adults in Korea. Korean J. Health Promot. 2013, 13, 141–149. [Google Scholar]
- Won, Y.I. Analysis of the effects of physically disabled people’s health promotion behaviors on sleep disorders. Korean J. Sport 2020, 18, 57–65. [Google Scholar] [CrossRef]
- Yun, H.J. Association of sleep duration and quality of sleep with depression in middle school students: Based on the Korean children and youth panel survey. J. Korean Acad. Soc. Home Health Care Nurs. 2020, 27, 189–197. [Google Scholar] [CrossRef]
- Chae, H. Relationships between sleep time and depression and suicidal ideation in middle aged women. J. Digit. Converg. 2020, 18, 263–272. [Google Scholar] [CrossRef]
- Lee, E.; Ma, R. The relationships between smart-phone addiction, sleep time and depression in female high school students. Asia-Pac. J. Multimed. Serv. Converg. Art Humanit. Sociol. 2018, 8, 533–542. [Google Scholar] [CrossRef]
- Shin, E. Association between self-reported sleep duration and depression or suicidal ideation in Korean adolescents. Anxiety Mood 2018, 14, 21–27. [Google Scholar] [CrossRef]
- Kim, H.R.; Kim, E.H. Prevalence of depression and its risk factors between elderly living alone and elderly living with others in Korea. J. Korean Data Anal. Soc. 2014, 16, 463–477. [Google Scholar]
- Lee, Y.S.; Tak, Y. Study of sleep patterns on depression and cognitive difficulties among older people living in the community. J. Korean Gerontol. Soc. 2016, 36, 548–633. [Google Scholar]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep duration and depression among adults: A meta-analysis of prospective studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef]
- Gilmour, H.; Stranges, S.; Kaplan, M.; Feeny, D.; McFarland, B.; Huguet, N.; Bernier, J. Longitudinal trajectories of sleep duration in the general population. Health Rep. 2013, 24, 14–20. [Google Scholar]
- Smagula, S.F.; Koh, W.P.; Wang, R.; Yuan, J.M. Chronic disease and lifestyle factors associated with change in sleep duration among older adults in the Singapore Chinese Health Study. J. Sleep Res. 2016, 25, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Wood, W.; Neal, D.T. Healthy through habit: Interventions for initiating & maintaining health behavior change. Behav. Sci. Policy 2016, 2, 71–83. [Google Scholar]
- Alvarez, G.G.; Ayas, N.T. The impact of daily sleep duration on health: A review of the literature. Prog. Cardiovasc. Nurs. 2004, 19, 56–59. [Google Scholar] [CrossRef]
- Kurma, V.M. Sleep and sleep disorders. Indian J. Chest Dis. Allied Sci. 2008, 50, 129–135. [Google Scholar]
- Rosmond, R.; Dallman, M.F.; Bjorntorp, P. Stress-related cortisol secretion in men: Relationships with abdominal obesity and endocrine, metabolic and hemodynamic abnormalities. J. Clin. Endocrinol. Metab. 1998, 83, 1853–1859. [Google Scholar] [CrossRef]
- Kim, M.H.; Kim, K.I. Strategies to increase participation in sports and physical activity among persons with disabilities: A review of national surveys. Korean J. Adapt. Phys. Act. 2019, 27, 61–72. [Google Scholar]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Kim, J.K.; Song, H.S.; Yeon, M.Y. The preliminary study of sleep patterns, circadian typology and depression level in Korean college students. Korean J. Health Psychol. 2009, 14, 617–632. [Google Scholar] [CrossRef]
- Jankowski, K.S. Morningness-eveningness and depressive symptoms: Test on the components level with CES-D in Polish students. J. Affect. Disord. 2016, 196, 47–53. [Google Scholar] [CrossRef]
- Merikanto, I.; Lahti, T.; Kronholm, E.; Peltonen, M.; Laatikainen, T.; Vartiainen, E.; Salomaa, V.; Partonen, T. Evening types are prone to depression. Chronobiol. Int. 2013, 30, 719–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of General Medical Sciences. Circadian Rhythms Fact Sheet. Available online: http://www.nigms.nih.gov/education/pages/Factsheet_CircadianRhythms.aspx (accessed on 9 March 2021).
- Lee, H.J. Is the circadian rhythm dysregulation a core pathogenetic mechanism of bipolar disorder? J. Korean Neuropsychiatr. Assoc. 2018, 57, 276–286. [Google Scholar] [CrossRef]
- Kim, K.H.; Hwang, E.H. Correlation among insomnia, sleep quality, depression, and circadian rhythm in nursing baccalaureate students. J. Korean Public Health Nurs. 2018, 32, 263–274. [Google Scholar] [CrossRef]
- Kim, J.I. Factor influencing depression in eco boomer. J. Digit. Converg. 2018, 16, 341–352. [Google Scholar] [CrossRef]
- Kim, J.H.; Suh, B.S.; Kim, D.I.; Yoon, K.J.; Hong, J.Y.; Lee, W.C.; Lee, J.E. Relationship between symptoms of depression and smoking and obesity in Korean office workers younger than 40 years. Korean J. Health Promot. 2013, 13, 23–33. [Google Scholar]
- Hong, H.; Huh, J. An analysis of depression of the individuals with disabilities using repeated measurement data. J. Korean Data Inf. Sci. Soc. 2017, 28, 1055–1067. [Google Scholar] [CrossRef]
- Jin, S.; Ko, G.; Cho, J.; Song, Y. Predictors of depression in disability with hearing impairment. Korean J. Rehabil. Nurs. 2020, 23, 38–47. [Google Scholar] [CrossRef]
- Kim, H. Examining depressive symptoms of visually impaired adults in Korea. J. Korea Acad. Ind. Coop. Soc. 2016, 17, 666–676. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Kim, S.Y.; Kim, M. Factors related to depression and activities of daily living in persons with disability: Using the Korean welfare panel data. Korean Public Health Res. 2014, 40, 51–62. [Google Scholar]
- Choi, H.K.; Lee, H.K. The relations of problem drinking, depressive mood, and suicidal ideation among Korean workers. Korean Public Health Res. 2016, 42, 29–40. [Google Scholar]
- Oh, D.; Kim, C.G. The factors associated with depression in the elderly male: Based on the 5th Korea national health and nutrition examination survey. Korean J. Adult Nurs. 2015, 27, 583–593. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All Variable at Baseline | Total | Self-Rated Depressive Symptom | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| N | % | N | % | N | % | ||
| Sleep duration (h) | <0.001 | ||||||
| ≤4 | 46 | 2.5 | 13 | 28.3 | 33 | 71.7 | |
| 5 | 144 | 7.8 | 41 | 28.5 | 103 | 71.5 | |
| 6 | 465 | 25.1 | 73 | 15.7 | 392 | 84.3 | |
| 7 | 656 | 35.4 | 73 | 11.1 | 583 | 88.9 | |
| 8 | 446 | 24.1 | 62 | 13.9 | 384 | 86.1 | |
| 9 | 53 | 2.9 | 10 | 18.9 | 43 | 81.1 | |
| ≥10 | 41 | 2.2 | 15 | 36.6 | 26 | 63.4 | |
| Gender | 0.211 | ||||||
| Male | 1277 | 69.0 | 189 | 14.8 | 1088 | 85.2 | |
| Female | 574 | 31.0 | 98 | 17.1 | 476 | 82.9 | |
| Age | 0.000 | ||||||
| 15–29 | 140 | 7.6 | 18 | 12.9 | 122 | 87.1 | |
| 30–39 | 445 | 24.0 | 50 | 11.2 | 395 | 88.8 | |
| 40–49 | 688 | 37.2 | 100 | 14.5 | 588 | 85.5 | |
| 50–59 | 367 | 19.8 | 83 | 22.6 | 284 | 77.4 | |
| ≥60 | 211 | 11.4 | 36 | 17.1 | 175 | 82.9 | |
| Residential region | 0.568 | ||||||
| Metropolitan | 292 | 15.8 | 49 | 16.8 | 243 | 83.2 | |
| Urban | 535 | 28.9 | 76 | 14.2 | 459 | 85.8 | |
| Rural | 1024 | 55.3 | 162 | 15.8 | 862 | 84.2 | |
| Marital status | <0.001 | ||||||
| Married | 1087 | 58.7 | 115 | 10.6 | 972 | 89.4 | |
| Single | 473 | 25.6 | 85 | 18.0 | 388 | 82.0 | |
| Divorce, separated | 291 | 15.7 | 87 | 29.9 | 204 | 70.1 | |
| Smoking status | 0.030 | ||||||
| Current smoker | 537 | 29.0 | 102 | 19.0 | 435 | 81.0 | |
| Former smoker | 415 | 22.4 | 58 | 14.0 | 357 | 86.0 | |
| Nothing | 899 | 48.6 | 127 | 14.1 | 772 | 85.9 | |
| Alcohol consumption | 0.029 | ||||||
| Drinker | 974 | 52.6 | 135 | 13.9 | 839 | 86.1 | |
| Former drinker | 353 | 19.1 | 70 | 19.8 | 283 | 80.2 | |
| Nothing | 524 | 28.3 | 82 | 15.7 | 442 | 84.4 | |
| Disability grade | 0.001 | ||||||
| 1–3 | 388 | 21.0 | 81 | 20.9 | 307 | 79.1 | |
| 4–6 | 1463 | 79.0 | 206 | 14.1 | 1257 | 85.9 | |
| Chronic disease | <0.001 | ||||||
| Yes | 479 | 25.9 | 116 | 24.2 | 363 | 75.8 | |
| No | 1372 | 74.1 | 171 | 12.5 | 1201 | 87.5 | |
| Self-rated health | <0.001 | ||||||
| Bad | 858 | 46.4 | 212 | 24.7 | 646 | 75.3 | |
| Good | 993 | 53.7 | 75 | 7.6 | 918 | 92.5 | |
| Employment | <0.001 | ||||||
| Worker in use | 818 | 44.2 | 75 | 9.2 | 743 | 90.8 | |
| Temporary worker | 266 | 14.4 | 30 | 11.3 | 236 | 88.7 | |
| Daily worker | 34 | 1.8 | 3 | 8.8 | 31 | 91.2 | |
| Self-employed | 70 | 3.8 | 16 | 22.9 | 54 | 77.1 | |
| Unpaid family volunteer | 663 | 35.8 | 163 | 24.6 | 500 | 75.4 | |
| Total | 1851 | 100.0 | 287 | 15.5 | 1564 | 84.5 | |
| Sleep Duration | Self-Rated Depressive Symptom | |||
|---|---|---|---|---|
| OR | 95% CI | p-Value | ||
| Sleep duration (h) | ||||
| ≤4 | 1.751 | 1.065 | 2.878 | |
| 5 | 1.845 | 1.346 | 2.530 | |
| 6 | 1.106 | 0.869 | 1.407 | |
| 7 | 1.000 | |||
| 8 | 1.265 | 1.008 | 1.586 | |
| 9 | 2.703 | 1.736 | 4.207 | |
| ≥10 | 4.179 | 2.616 | 6.675 | |
| Gender | ||||
| Male | 0.868 | 0.672 | 1.121 | |
| Female | 1.000 | |||
| Age | ||||
| 15–29 | 0.738 | 0.457 | 1.194 | 0.216 |
| 30–39 | 1.153 | 0.829 | 1.603 | 0.399 |
| 40–49 | 1.173 | 0.890 | 1.546 | 0.256 |
| 50–59 | 1.112 | 0.847 | 1.460 | 0.444 |
| ≥60 | 1.000 | |||
| Residential region | ||||
| Metropolitan | 0.864 | 0.674 | 1.107 | 0.247 |
| Urban | 0.764 | 0.624 | 0.935 | 0.009 |
| Rural | 1.000 | |||
| Marital status | ||||
| Married | 0.461 | 0.370 | 0.575 | <0.001 |
| Single | 0.763 | 0.586 | 0.995 | 0.046 |
| Divorce, separated | 1.000 | |||
| Smoking status | ||||
| Current smoker | 1.497 | 1.140 | 1.966 | 0.004 |
| Former smoker | 1.201 | 0.897 | 1.608 | 0.218 |
| Nothing | 1.000 | |||
| Alcohol consumption | ||||
| Drinker | 0.904 | 0.711 | 1.151 | 0.412 |
| Former drinker | 0.932 | 0.718 | 1.210 | 0.595 |
| Nothing | 1.000 | |||
| Disability grade | ||||
| 1–3 | 1.485 | 1.222 | 1.805 | <0.001 |
| 4–6 | 1.000 | |||
| Chronic disease | ||||
| Yes | 1.445 | 1.191 | 1.753 | 0.000 |
| No | 1.000 | |||
| Employment status | ||||
| Worker in use | 0.435 | 0.348 | 0.545 | <0.001 |
| Temporary worker | 0.497 | 0.373 | 0.662 | <0.001 |
| Daily worker | 0.184 | 0.057 | 0.596 | 0.005 |
| Self-employed | 0.857 | 0.528 | 1.393 | 0.534 |
| Unpaid family volunteer | 1.000 | |||
| Self-rated health | ||||
| Bad | 2.329 | 1.893 | 2.865 | <0.001 |
| Good | 1.000 | |||
| Perceived stress | ||||
| Yes | 3.149 | 2.566 | 3.865 | <0.001 |
| No | 1.000 | |||
| Year | ||||
| 2016 | 1.346 | 1.091 | 1.659 | 0.006 |
| 2017 | 1.116 | 0.900 | 1.385 | 0.317 |
| 2018 | 1.000 | |||
| Sleep Patterns Overtime | Self-Rated Depressive Symptom | |||
|---|---|---|---|---|
| OR | 95% CI | p-Value | ||
| Sleep patterns overtime | ||||
| 1 | 2.073 | 1.460 | 2.944 | <0.001 |
| 2 | 1.000 | |||
| 3 | 1.503 | 1.124 | 2.011 | 0.006 |
| 4 | 1.170 | 0.966 | 1.417 | 0.108 |
| Gender | ||||
| Male | 0.913 | 0.709 | 1.178 | 0.485 |
| Female | 1.000 | |||
| Age | ||||
| 15–29 | 0.754 | 0.468 | 1.215 | 0.246 |
| 30–39 | 1.174 | 0.846 | 1.630 | 0.337 |
| 40–49 | 1.161 | 0.883 | 1.527 | 0.286 |
| 50–59 | 1.108 | 0.846 | 1.452 | 0.455 |
| ≥60 | 1.000 | |||
| Residential region | ||||
| Metropolitan | 0.898 | 0.702 | 1.149 | 0.394 |
| Urban | 0.777 | 0.636 | 0.949 | 0.014 |
| Rural | 1.000 | |||
| Marital status | ||||
| Married | 0.456 | 0.366 | 0.567 | <0.001 |
| Single | 0.757 | 0.582 | 0.984 | 0.038 |
| Divorce, separated | 1.000 | |||
| Smoking status | ||||
| Current smoker | 1.481 | 1.131 | 1.941 | 0.004 |
| Former smoker | 1.181 | 0.884 | 1.576 | 0.261 |
| Nothing | 1.000 | |||
| Alcohol consumption | ||||
| Drinker | 0.876 | 0.690 | 1.113 | 0.279 |
| Former drinker | 0.926 | 0.715 | 1.199 | 0.559 |
| Nothing | 1.000 | |||
| Disability grade | ||||
| 1–3 | 1.482 | 1.221 | 1.798 | <0.001 |
| 4–6 | 1.000 | |||
| Chronic disease | ||||
| Yes | 1.430 | 1.181 | 1.732 | 0.000 |
| No | 1.000 | |||
| Employment status | ||||
| Worker in use | 0.400 | 0.320 | 0.500 | <0.001 |
| Temporary worker | 0.469 | 0.353 | 0.624 | <0.001 |
| Daily worker | 0.170 | 0.053 | 0.550 | 0.003 |
| Self-employed | 0.818 | 0.505 | 1.324 | 0.413 |
| Unpaid family volunteer | 1.000 | |||
| Self-rated health | ||||
| Bad | 2.388 | 1.944 | 2.933 | <0.001 |
| Good | 1.000 | |||
| Perceived stress | ||||
| Yes | 3.067 | 2.504 | 3.756 | <0.001 |
| No | 1.000 | |||
| Year | ||||
| 2016 | 1.371 | 1.114 | 1.687 | 0.003 |
| 2017 | 1.130 | 0.913 | 1.400 | 0.261 |
| 2018 | 1.000 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, S.J.; Jeong, Y.M.; Kim, J.-H. Relationship between Sleep Duration Trajectories and Self-Rated Depressive Symptoms in South Koreans with Physical Disabilities. Healthcare 2021, 9, 361. https://doi.org/10.3390/healthcare9030361
Yi SJ, Jeong YM, Kim J-H. Relationship between Sleep Duration Trajectories and Self-Rated Depressive Symptoms in South Koreans with Physical Disabilities. Healthcare. 2021; 9(3):361. https://doi.org/10.3390/healthcare9030361
Chicago/Turabian StyleYi, Su Jeong, Yoo Mi Jeong, and Jae-Hyun Kim. 2021. "Relationship between Sleep Duration Trajectories and Self-Rated Depressive Symptoms in South Koreans with Physical Disabilities" Healthcare 9, no. 3: 361. https://doi.org/10.3390/healthcare9030361