
Resilience as a Mediator of the Association between Spirituality and Self-Management among Older People with Chronic Obstructive Pulmonary Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures and Variables
2.3. Statistical Analysis
3. Results
3.1. Participants’ Sociodemographic and Clinical Characteristics
3.2. Descriptive Characteristics of Target Variables and Relationships among Them
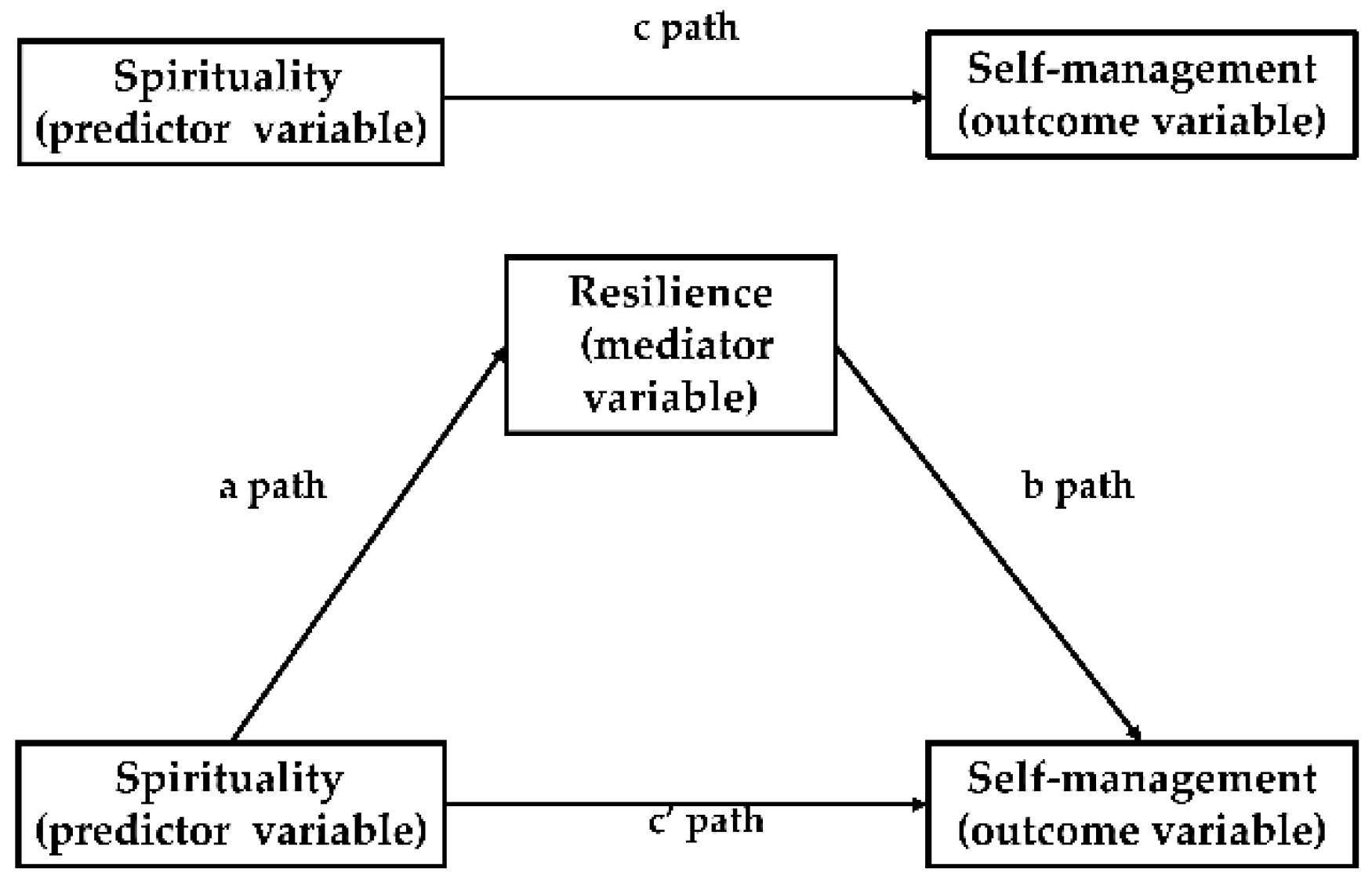
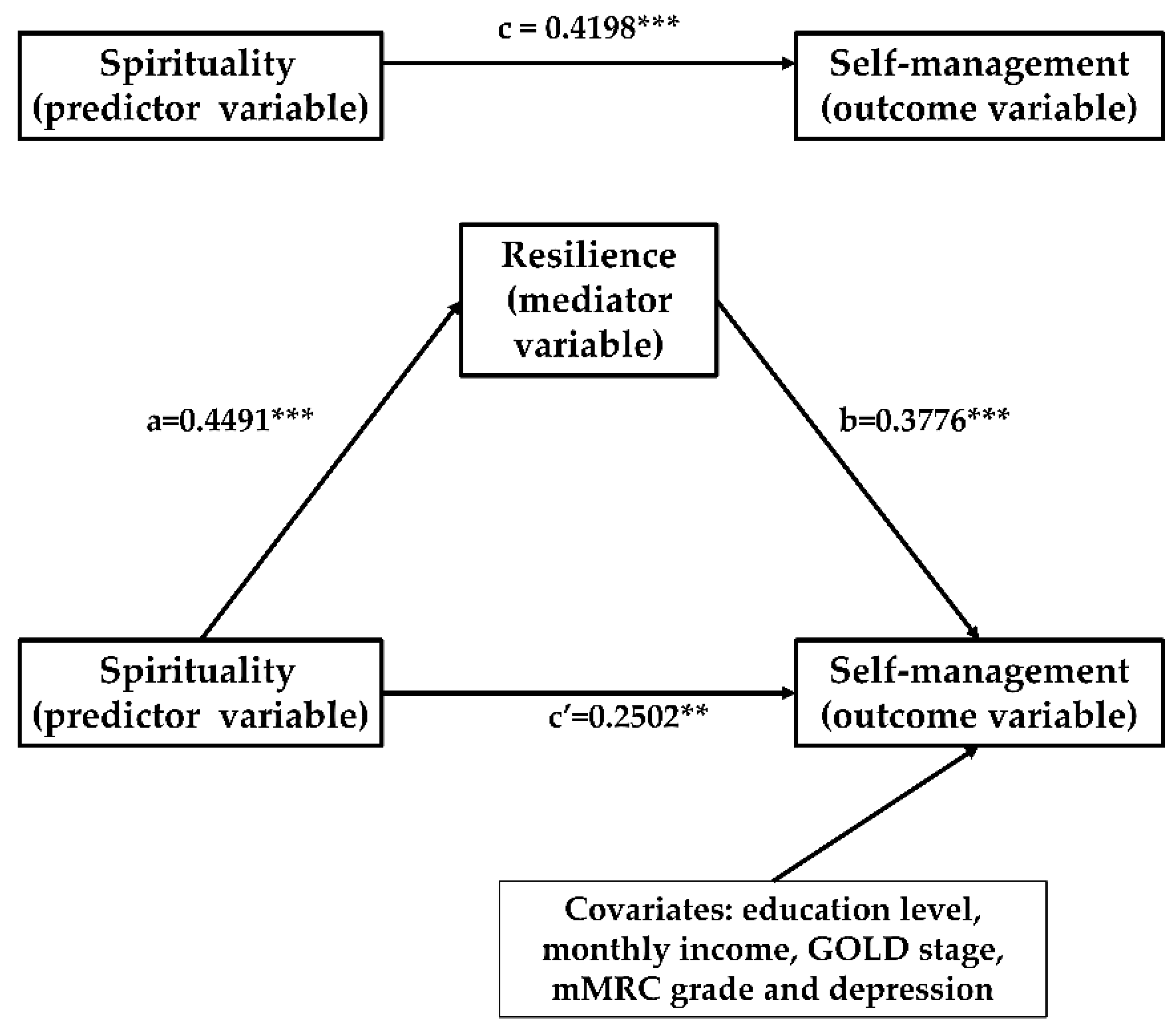
3.3. Mediating Effects of Resilience on the Relationship between Spirituality and Self-Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (2021 Report). Available online: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf (accessed on 1 October 2021).
- Celli, B.R.; Wedzicha, J.A. Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Lopez, A.D. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997, 349, 1498–1504. [Google Scholar] [CrossRef]
- Duan, R.-R.; Hao, K.; Yang, T. Air pollution and chronic obstructive pulmonary disease. Chronic Dis. Transl. Med. 2020, 6, 260–269. [Google Scholar] [CrossRef]
- Barrecheguren, M.; Bourbeau, J. Self-management strategies in chronic obstructive pulmonary disease: A first step toward personalized medicine. Curr. Opin. Pulm. Med. 2018, 24, 191–198. [Google Scholar] [CrossRef]
- Bringsvor, H.B.; Skaug, K.; Langeland, E.; Oftedal, B.F.; Assmus, J.; Gundersen, D.; Osborne, R.H.; Bentsen, S.B. Symptom burden and self-management in persons with chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenferink, A.; Brusse-Keizer, M.; van der Valk, P.D.; Frith, P.A.; Zwerink, M.; Monninkhof, E.M.; van der Palen, J.; Effing, T.W. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 2017, CD011682. [Google Scholar] [CrossRef] [PubMed]
- Disler, R.; Gallagher, R.; Davidson, P. Factors influencing self-management in chronic obstructive pulmonary disease: An integrative review. Int. J. Nurs. Stud. 2012, 49, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Bourbeau, J.; Nault, D.; Dang-Tan, T. Self-management and behaviour modification in COPD. Patient Educ. Couns. 2004, 52, 271–277. [Google Scholar] [CrossRef]
- Effing, T.; Monninkhof, E.M.; van der Valk, P.D.; van der Palen, J.; van Herwaarden, C.L.; Partidge, M.R.; Walters, E.H.; Zielhuis, G.A. Self-management education for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2007, 4, CD002990:1–CD002990:66. [Google Scholar]
- Helvaci, A.; Metin, Z.G. The effects of nurse-driven self-management programs on chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Adv. Nurs. 2020, 76, 2849–2871. [Google Scholar] [CrossRef]
- Song, X.; Hallensleben, C.; Zhang, W.; Jiang, Z.; Shen, H.; Gobbens, R.J.J.; Van Der Kleij, R.M.J.J.; Chavannes, N.H.; Versluis, A. Blended Self-Management Interventions to Reduce Disease Burden in Patients With Chronic Obstructive Pulmonary Disease and Asthma: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e24602:1–e24602:19. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Wang, H.; Du, L.; Wang, Y.; Wang, X.; Zhang, R. Disease knowledge and self-management behavior of COPD patients in China. Medicine 2019, 98, e14460. [Google Scholar] [CrossRef] [PubMed]
- Yadav, U.N.; Lloyd, J.; Hosseinzadeh, H.; Baral, K.P.; Bhatta, N.; Harris, M.F. Self-management practice, associated factors and its relationship with health literacy and patient activation among multi-morbid COPD patients from rural Nepal. BMC Public Health 2020, 20, 300. [Google Scholar] [CrossRef]
- Russell, S.; Ogunbayo, O.J.; Newham, J.J.; Heslop-Marshall, K.; Netts, P.; Hanratty, B.; Beyer, F.; Kaner, E. Qualitative systematic review of barriers and facilitators to self-management of chronic obstructive pulmonary disease: Views of patients and healthcare professionals. NPJ Prim. Care Respir. Med. 2018, 28, 2. [Google Scholar] [CrossRef] [PubMed]
- Gergianaki, I.; Kampouraki, M.; Williams, S.; Tsiligianni, I. Assessing spirituality: Is there a beneficial role in the management of COPD? NPJ Prim. Care Respir. Med. 2019, 29, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badanta-Romero, B.; de Diego-Cordero, R.; Rivilla-Garcia, E. Influence of Religious and Spiritual Elements on Adherence to Pharmacological Treatment. J. Relig. Health 2018, 57, 1905–1917. [Google Scholar] [CrossRef]
- Kretchy, I.; Owusu-Daaku, F.; Danquah, S. Spiritual and religious beliefs: Do they matter in the medication adherence behaviour of hypertensive patients? BioPsychoSocial Med. 2013, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization. Review of the Constitution of the World Health Organization: Report of the Executive Board Special Group. Available online: https://apps.who.int/gb/archive/pdf_files/EB101/pdfangl/angr2.pdf (accessed on 2 October 2021).
- Selman, L.; Harding, R.; Gysels, M.; Speck, P.; Higginson, I.J. The Measurement of Spirituality in Palliative Care and the Content of Tools Validated Cross-Culturally: A Systematic Review. J. Pain Symptom Manag. 2011, 41, 728–753. [Google Scholar] [CrossRef]
- John, F. The Four Domains Model: Connecting Spirituality, Health and Well-Being. Religions 2011, 2, 17–28. [Google Scholar]
- Vasigh, A.; Tarjoman, A.; Borji, M. Relationship between Spiritual Health and Pain Self-Efficacy in patients with Chronic Pain: A Cross-Sectional Study in West of Iran. J. Relig. Health 2019, 59, 1115–1125. [Google Scholar] [CrossRef]
- Adegbola, M. Spirituality, Self-Efficacy, and Quality of Life among Adults with Sickle Cell Disease. South. Online J. Nurs. Res. 2011, 11, 5. [Google Scholar] [PubMed]
- Unantenne, N.; Warren, N.; Canaway, R.; Manderson, L. The Strength to Cope: Spirituality and Faith in Chronic Disease. J. Relig. Health 2013, 52, 1147–1161. [Google Scholar] [CrossRef] [PubMed]
- Zadworna-Cieślak, M. Spirituality, satisfaction with life and health-related behavior of older residents of long-term care institutions—a pilot study. Explore 2020, 16, 123–129. [Google Scholar] [CrossRef]
- Alexander, A.; Robinson, L.A.; Ward, K.D.; Farrell, A.S.; Ferkin, A.C. Religious Beliefs Against Smoking Among Black and White Urban Youth. J. Relig. Health 2015, 55, 1907–1916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helvaci, A.; Izgu, N.; Ozdemir, L. Relationship between symptom burden, medication adherence and spiritual well-being in patients with chronic obstructive pulmonary disease. J. Clin. Nurs. 2020, 29, 2388–2396. [Google Scholar] [CrossRef] [PubMed]
- Mendes, N.S.; Malaguti, C.; Dos Anjos Sena, L.; Lucchetti, G.; de Jesus, L.A.S.; Vitorino, L.M.; Mesquita, R.; Lee, A.L.; Oliveira, C.C. Spirituality and religiosity are associated with physical and psychological status in patients with chronic obstructive pulmonary disease. J. Clin. Nurs. 2021, 1–10. [Google Scholar] [CrossRef]
- Osborne, R.H.; Elsworth, G.R.; Whitfield, K. The Health Education Impact Questionnaire (heiQ): An outcomes and evaluation measure for patient education and self-management interventions for people with chronic conditions. Patient Educ. Couns. 2007, 66, 192–201. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, W.; Li, J.; Cai, X.; Zhang, H.; Wang, H.; Wang, X. Development and Validation of a COPD Self-Management Scale. Respir. Care 2013, 58, 1931–1936. [Google Scholar] [CrossRef] [Green Version]
- Harvey, I.S. Self-Management of a Chronic Illness: An Exploratory Study on the Role of Spirituality among Older African American Women. J. Women Aging 2006, 18, 75–88. [Google Scholar] [CrossRef]
- Harvey, I.S.; Silverman, M. The Role of Spirituality in the Self-management of Chronic Illness among Older African and Whites. J. Cross-Cult. Gerontol. 2007, 22, 205–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polzer, R.; Miles, M.S. Spirituality and self-management of diabetes in African Americans. J. Holist. Nurs. 2005, 23, 230–250. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, J.A.; Wright, C.; Fordyce, J.; Ohueri, C.; Garciá, A.A. Self-Management of HIV and Diabetes in African American Women: A Systematic Review of Qualitative Literature. Diabetes Educ. 2018, 44, 419–434. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. The Road to Resilience. Available online: https://uncw.edu/studentaffairs/committees/pdc/documents/the%20road%20to%20resilience.pdf (accessed on 17 November 2021).
- Lu, Y.; Nyunt, M.S.Z.; Gwee, X.; Feng, L.; Feng, L.; Kua, E.H.; Kumar, R.; Ng, T.P. Life event stress and chronic obstructive pulmonary disease (COPD): Associations with mental well-being and quality of life in a population-based study. BMJ Open 2012, 2, e001674. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.; Nascimento, F.A.B.D.; Macêdo, T.P.; Morano, M.T.A.P.; Mesquita, R.; Pereira, E.D.B. Religious coping and religiosity in patients with COPD following pulmonary rehabilitation. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Sorathia, L. Palliative Care in Chronic Obstructive Pulmonary Disease. Med. Clin. N. Am. 2019, 103, 517–526. [Google Scholar] [CrossRef]
- Luckett, T.; Roberts, M.; Swami, V.; Smith, T.; Cho, J.-G.; Klimkeit, E.; Wheatley, J.R. Maintenance of non-pharmacological strategies 6 months after patients with chronic obstructive pulmonary disease (COPD) attend a breathlessness service: A qualitative study. BMJ Open 2021, 11, e050149. [Google Scholar] [CrossRef]
- Qin, J.; Bai, S.; Yan, Z.; Li, X.; Luo, C. Mediating effect of mindfulness between resilience and self-management behavior in patients with type 2 diabetes. Chin. J. Behav. Med. Brain Sci. 2021, 30, 528–532. [Google Scholar]
- Song, J.; Deng, Y.; Yang, Y.; Liu, Q. Resilience and related factors among elderly patients undergoing persistent hemodialysis. J. Nurs. Sci. 2017, 32, 19–21. [Google Scholar]
- Jones, K.F.; Simpson, G.; Briggs, L.; Dorsett, P.; Anderson, M. A study of whether individual and dyadic relations between spirituality and resilience contribute to psychological adjustment among individuals with spinal cord injuries and their family members. Clin. Rehabil. 2019, 33, 1503–1514. [Google Scholar] [CrossRef]
- Jones, K.; Simpson, G.K.; Briggs, L.; Dorsett, P. Does spirituality facilitate adjustment and resilience among individuals and families after SCI? Disabil. Rehabil. 2015, 38, 921–935. [Google Scholar] [CrossRef] [Green Version]
- Ozawa, C.; Suzuki, T.; Mizuno, Y.; Tarumi, R.; Yoshida, K.; Fujii, K.; Hirano, J.; Tani, H.; Rubinstein, E.B.; Mimura, M.; et al. Resilience and spirituality in patients with depression and their family members: A cross-sectional study. Compr. Psychiatry 2017, 77, 53–59. [Google Scholar] [CrossRef]
- Munari, A.B.; Gulart, A.A.; Dos Santos, K.; Venâncio, R.S.; Karloh, M.; Mayer, A.F. Modified Medical Research Council Dyspnea Scale in GOLD Classification Better Reflects Physical Activities of Daily Living. Respir. Care 2017, 63, 77–85. [Google Scholar] [CrossRef]
- Alden, D.; Austin, C.; Sturgeon, R. A Correlation between the Geriatric Depression Scale Long and Short Forms. J. Gerontol. 1989, 44, P124–P125. [Google Scholar] [CrossRef]
- Strada, E.A.; Homel, P.; Tennstedt, S.; Billings, J.A.; Portenoy, R.K. Spiritual well-being in patients with advanced heart and lung disease. Palliat. Support. Care. 2013, 11, 205–213. [Google Scholar] [CrossRef]
- Liu, X.; Wei, D.; Chen, Y.; Cheng, Q.; Liang, S.; Xu, X.; Zhang, M. Reliability and validity of the Chinese version of the functional assessment of chronic illness therapy-spiritual well-being in cancer patients. Chin. Gen. Pract. Nurs. 2016, 51, 1085–1090. [Google Scholar]
- Cheng, C.; Dong, D.; He, J.; Zhong, X.; Yao, S. Psychometric properties of the 10-item Connor–Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J. Affect. Disord. 2020, 261, 211–220. [Google Scholar] [CrossRef]
- Zhang, D.; Xiong, M.; Li, Y. The reliability and validity of 10-item Connor-Davidson resilience scale in the community-dwelling ol-der adults. Chin. J. Behav. Med. Brain Sci. 2018, 27, 942–946. [Google Scholar]
- Wang, L.; Nygårdh, A.; Zhao, Y.; Mårtensson, J. Self-management among patients with chronic obstructive pulmonary disease in China and its association with sociodemographic and clinical variables. Appl. Nurs. Res. 2016, 32, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Process Analysis: A Regression-Based Approach. Available online: http://dm.darden.virginia.edu/ResearchMethods/Templates.pdf (accessed on 17 November 2021).
- Rijnhart, J.J.; Twisk, J.W.; Chinapaw, M.; de Boer, M.; Heymans, M.W. Comparison of methods for the analysis of relatively simple mediation models. Contemp. Clin. Trials Commun. 2017, 7, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Funes, C.M.; Lavretsky, H.; Ercoli, L.; Cyr, N.S.; Siddarth, P. Apathy Mediates Cognitive Difficulties in Geriatric Depression. Am. J. Geriatr. Psychiatry 2018, 26, 100–106. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Warsi, G.; Dwyer, J.H. A Simulation Study of Mediated Effect Measures. Multivar. Behav. Res. 1995, 30, 41–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, A.K.; Osborne, R.H.; Larsen, M.H.; Andersen, M.H.; Holter, I.A.; Borge, C.R. Exploring health literacy needs in Chronic obstructive pulmonary disease (COPD): Associations between demographic, clinical variables, psychological well-being and health literacy. Heart Lung 2021, 50, 417–424. [Google Scholar] [CrossRef]
- Shi, S.; Hao, X.; Chen, C. Factors influencing general self-efficacy in elderly patients with chronic obstructive pulmonary disease in the community. Chin. J. Gerontol. 2015, 35, 7194–7196. [Google Scholar] [CrossRef]
- Parshall, M.; Schwartzstein, R.M.; Adams, L.; Banzett, R.B.; Manning, H.L.; Bourbeau, J.; Calverley, P.M.; Gift, A.G.; Harver, A.; Lareau, S.C.; et al. An Official American Thoracic Society Statement: Update on the Mechanisms, Assessment, and Management of Dyspnea. Am. J. Respir. Crit. Care Med. 2012, 185, 435–452. [Google Scholar] [CrossRef] [Green Version]
- Fraser, D.D.; Kee, C.C.; Minick, P. Living with chronic obstructive pulmonary disease: Insiders’ perspectives. J. Adv. Nurs. 2006, 55, 550–558. [Google Scholar] [CrossRef]
- Hanania, N.A.; O’Donnell, D.E. Activity-related dyspnea in chronic obstructive pulmonary disease: Physical and psychological consequences, unmet needs, and future directions. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1127–1138. [Google Scholar] [CrossRef] [Green Version]
- Miravitlles, M.; Worth, H.; Soler Cataluna, J.J.; Price, D.; De Benedetto, F.; Roche, N.; Godtfredsen, N.S.; van der Molen, T.; Löfdahl, C.G.; Padullés, L.; et al. Observational study to characterise 24-h COPD symptoms and their relationship with patient-reported outcomes: Results from the ASSESS study. Respir. Res. 2014, 15, 122:1–122:13. [Google Scholar] [CrossRef]
- Pham, T.V.; Beasley, C.M.; Gagliardi, J.P.; Koenig, H.G.; Stanifer, J.W. Spirituality, Coping, and Resilience Among Rural Residents Living with Chronic Kidney Disease. J. Relig. Health 2020, 59, 2951–2968. [Google Scholar] [CrossRef]
- Kwan, C.W.; Chan, C.W.; Choi, K.C. The effectiveness of a nurse-led short term life review intervention in enhancing the spiritual and psychological well-being of people receiving palliative care: A mixed method study. Int. J. Nurs. Stud. 2019, 91, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, N.; Kenealy, T.; Salmon, E.; Rea, H.; Raphael, D.; Schmidt-Busby, J. Helplessness, self blame and faith may impact on self management in COPD: A qualitative study. Prim. Care Respir. J. 2011, 20, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Seamark, D.A.; Blake, S.D.; Seamark, C.J.; Halpin, D.M. Living with severe chronic obstructive pulmonary disease (COPD): Perceptions of patients and their carers. An interpretative phenomenological analysis. Palliat. Med. 2004, 18, 619–625. [Google Scholar] [CrossRef]
- Ek, K.; Ternestedt, B.-M. Living with chronic obstructive pulmonary disease at the end of life: A phenomenological study. J. Adv. Nurs. 2008, 62, 470–478. [Google Scholar] [CrossRef]
- Azar, N.S.; Radfar, M.; Baghaei, R. Spiritual Self-care in Stroke Survivors: A Qualitative Study. J. Relig. Health 2020, 1–14. [Google Scholar] [CrossRef]
- Samuel-Hodge, C.D.; Keyserling, T.C.; Park, S.; Johnston, L.F.; Gizlice, Z.; Bangdiwala, S.I. A Randomized Trial of a Church-Based Diabetes Self-management Program for African Americans with Type 2 Diabetes. Diabetes Educ. 2009, 35, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Baig, A.A.; Benitez, A.; Locklin, C.A.; Gao, Y.; Lee, S.M.; Quinn, M.T.; Solomon, M.C.; Sánchez-Johnsen, L.; Burnet, D.L.; Chin, M.H.; et al. Picture Good Health: A Church-Based Self-Management Intervention Among Latino Adults with Diabetes. J. Gen. Intern. Med. 2015, 30, 1481–1490. [Google Scholar] [CrossRef] [Green Version]
- Simpson, G.K.; Anderson, M.I.; Jones, K.F.; Genders, M.; Gopinath, B. Do spirituality, resilience and hope mediate outcomes among family caregivers after traumatic brain injury or spinal cord injury? A structural equation modelling approach. NeuroRehabilitation 2020, 46, 3–15. [Google Scholar] [CrossRef]
- Mizuno, Y.; Hofer, A.; Suzuki, T.; Frajo-Apor, B.; Wartelsteiner, F.; Kemmler, G.; Saruta, J.; Tsukinoki, K.; Mimura, M.; Fleischhacker, W.W.; et al. Clinical and biological correlates of resilience in patients with schizophrenia and bipolar disorder: A cross-sectional study. Schizophr. Res. 2016, 175, 148–153. [Google Scholar] [CrossRef]
- Parviniannasab, A.M.; Rakhshan, M.; Momennasab, M.; Soltanian, M.; Rambod, M.; Akbarzadeh, M. Haemophiliac adolescents’ perspectives of resilience: A qualitative study based on the resilience in illness model. Clin. Child Psychol. Psychiatry 2019, 25, 346–358. [Google Scholar] [CrossRef]
- Haase, J.E.; Kintner, E.K.; Robb, S.; Stump, T.E.; Monahan, P.O.; Phillips, C.; Stegenga, K.A.; Burns, D. The Resilience in Illness Model Part 2: Confirmatory Evaluation in Adolescents and Young Adults with Cancer. Cancer Nurs. 2017, 40, 454–463. [Google Scholar] [CrossRef]
- Smith, B.W.; Ortiz, J.A.; Wiggins, K.T.; Bernard, J.F.; Dalen, J. Spirituality, Resilience, and Positive Emotions. Oxford Handbooks. Available online: https://sci-hub.se/10.1093/oxfordhb/9780199729920.013.0028 (accessed on 17 November 2021).
- Dubois, S.K.; Lehrer, H.M.; Whyne, E.Z.; Steinhardt, M.A. A Resilience Intervention for Adults with Type 2 Diabetes: Proof-of-Concept in Community Health Centers. Int. J. Behav. Med. 2020, 27, 565–575. [Google Scholar] [CrossRef] [PubMed]
- da Silva, M.S.; Kimura, M.; Stelmach, R.; de Gouveia Santos, V.L.C. Quality of life and spiritual well-being in chronic obstructive pulmonary disease patients. Rev. Esc. Enferm. USP 2009, 43, 1186–1191. [Google Scholar]
- Hasegawa, T.; Kawai, M.; Kuzuya, N.; Futamura, Y.; Horiba, A.; Ishiguro, T.; Yoshida, T.; Sawa, T.; Sugiyama, Y. Spiritual Well-Being and Correlated Factors in Subjects With Advanced COPD or Lung Cancer. Respir. Care 2017, 62, 544–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.M.; Lim, J.Y.; Kim, E.J.; Park, S. Resilience of patients with chronic diseases: A systematic review. Health Soc. Care Community 2018, 27, 797–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, D.; Zhou, M.; Sun, L.; Lin, Z.; Bian, Q.; Liu, M.; Ren, S. Resilience as a Mediator of the Association Between Perceived Stigma and Quality of Life Among People With Inflammatory Bowel Disease. Front. Psychiatry 2021, 12, 1333. [Google Scholar] [CrossRef]
- Ploughman, M.; Downer, M.B.; Pretty, R.W.; Wallack, E.M.; Amirkhanian, S.; Kirkland, M.C. Health, Lifestyle and Aging with MS Canadian Consortium. The impact of resilience on healthy aging with multiple sclerosis. Qual. Life Res. 2020, 29, 2769–2779. [Google Scholar] [CrossRef]
- Mendoza-Pinto, C.; García-Carrasco, M.; Campos-Rivera, S.; Munguía-Realpozo, P.; Etchegaray-Morales, I.; Ayón-Aguilar, J.; Alonso-García, N.E.; Méndez-Martínez, S. Medication adherence is influenced by resilience in patients with systemic lupus erythematosus. Lupus 2021, 30, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Springfield, S.; Qin, F.; Hedlin, H.; Eaton, C.B.; Rosal, M.C.; Taylor, H.; Staudinger, U.M.; Stefanick, M.L. Resilience and CVD-protective Health Behaviors in Older Women: Examining Racial and Ethnic Differences in a Cross-Sectional Analysis of the Women’s Health Initiative. Nutrients 2020, 12, 2107. [Google Scholar] [CrossRef]
- Tiemensma, J.; Gaab, E.; Voorhaar, M.; Asijee, G.; Kaptein, A.A. Illness perceptions and coping determine quality of life in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2001–2007. [Google Scholar] [CrossRef] [Green Version]
- Steinhardt, M.A.; Mamerow, M.M.; Brown, S.A.; Jolly, C.A. A resilience intervention in African American adults with type 2 diabetes: A pilot study of efficacy. Diabetes Educ. 2009, 35, 274–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, L.A.; Harrington, P.; Taylor, S.J.; Teljeur, C.; Smith, S.; Pinnock, H.; Ryan, M. Clinical-effectiveness of self-management interventions in chronic obstructive pulmonary disease: An overview of reviews. Chronic Respir. Dis. 2017, 14, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Edward, K. Chronic illness and wellbeing: Using nursing practice to foster resillence as resistance. Br. J. Nurs. 2013, 22, 741–746. [Google Scholar] [CrossRef]
- Cannon, D.L.; Sriram, K.B.; Liew, A.W.-C.; Sun, J. Resilience Factors Important in Health-Related Quality of Life of Subjects with COPD. Respir. Care 2018, 63, 1281–1292. [Google Scholar] [CrossRef]
- Choi, S.A.; Hastings, J.F. Religion, spirituality, coping, and resilience among African Americans with diabetes. J. Relig. Spirit. Soc. Work. Soc. Thought 2019, 38, 93–114. [Google Scholar] [CrossRef]
- Cosco, T.D.; Howse, K.; Brayne, C. Healthy ageing, resilience and wellbeing. Epidemiol. Psychiatr. Sci. 2017, 26, 579–583. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Categories | n (%) | COPD Self-Management | ||
|---|---|---|---|---|---|
| M ± SD | t/F | p | |||
| Gender | Male | 127 (84.1) | 152.61 ± 20.88 | 1.638 | 0.104 |
| Female | 24 (15.9) | 144.92 ± 22.23 | |||
| Age (years) | 60–69 | 35 (23.2) * | 152.54 ± 16.52 | 0.749 | 0.475 |
| 70–79 | 78 (51.7) * | 152.64 ± 21.79 | |||
| ≥80 | 38 (25.2) * | 147.74 ± 23.80 | |||
| Marital status | Spouses living | 120 (79.5) | 152.07 ± 21.38 | 0.777 | 0.438 |
| Others | 31 (20.5) | 148.74 ± 20.66 | |||
| Education level | Primary school and below | 60 (39.7) | 143.25 ± 17.48 | 8.991 | <0.001 |
| Junior-senior high school | 77 (51.0) | 155.55 ± 21.83 | |||
| College and above | 14 (9.3) | 163.36 ± 21.33 | |||
| Monthly income, Yuan | <3000 | 61 (40.4) | 146.92 ± 21.14 | 3.627 | 0.029 |
| 3000–5000 | 44 (29.1) | 150.82 ± 20.12 | |||
| >5000 | 46 (30.5) | 157.85 ± 21.14 | |||
| Smoking status | Never smoked | 37 (24.5) | 147.54 ± 20.46 | 3.049 | 0.050 |
| Current smoker | 34 (22.5) | 146.29 ± 17.61 | |||
| Ex-smoker | 80 (53.0) | 155.33 ± 22.36 | |||
| Are religious? | Yes | 15 (9.9) | 153.80 ± 14.86 | 0.464 | 0.644 |
| No | 136 (90.1) | 151.12 ± 21.82 | |||
| Number of hospitalizations in the last 1 year | 0–1 | 43 (28.5) | 153.95 ± 22.36 | 0.531 | 0.589 |
| 2–3 | 92 (60.9) | 150.73 ± 21.36 | |||
| >3 | 16 (10.6) | 148.25 ± 17.28 | |||
| GOLD stage | Stage I | 2 (1.3) | 198.00 ± 4.24 | 4.721 | 0.004 |
| Stage II | 28 (18.5) | 156.00 ± 21.76 | |||
| Stage III | 62 (41.1) | 151.68 ± 19.95 | |||
| Stage IV | 59 (39.1) | 147.31 ± 20.55 | |||
| mMRC | <2 | 21 (13.9) | 168.57 ± 22.53 | 4.221 | <0.001 |
| ≥2 | 130 (86.1) | 148.61 ± 19.71 | |||
| Depression | nomal | 121 (80.1) * | 153.21 ± 21.49 | 3.741 | 0.0260 |
| mild | 26 (17.2) * | 146.54 ± 17.91 | |||
| moderate tosevere | 4 (2.6) * | 127.75 ± 16.30 | |||
| Variables | Range | M ± SD | Standardized Score (M ± SD) |
|---|---|---|---|
| Spirituality | 8–46 | 26.77 ± 7.47 | 2.23 ± 0.62 |
| Resilience | 9–39 | 23.96 ± 6.21 | 2.40 ± 0.62 |
| Symptom management dimension | 13–32 | 22.91 ± 3.71 | 2.86 ± 0.46 |
| daily life management dimension | 31–61 | 45.18 ± 6.58 | 3.23 ± 0.47 |
| emotion management dimension | 21–57 | 37.60 ± 6.42 | 3.13 ± 0.54 |
| information management dimension | 8–31 | 18.75 ± 4.76 | 2.34 ± 0.60 |
| self-efficacy dimension | 13–44 | 26.93 ± 5.94 | 2.99 ± 0.66 |
| Self-management | 90–210 | 151.38 ± 21.21 | 2.97 ± 0.42 |
| Variables | Correlation Matrix | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 3-1 | 3-2 | 3-3 | 3-4 | 3-5 | |
| 1. Spirituality | 1 | |||||||
| 2. Resilience | 0.437 ** | 1 | ||||||
| 3. Self-management | 0.419 *** | 0.497 *** | 1 | |||||
| 3-1. Symptom management dimension | 0.205 * | 0.236 ** | 0.582 *** | 1 | ||||
| 3-2. Daily life management dimension | 0.324 *** | 0.218 ** | 0.762 *** | 0.307 ** | 1 | |||
| 3-3. Emotion management dimension | 0.439 *** | 0.595 *** | 0.786 *** | 0.242 ** | 0.467 *** | 1 | ||
| 3-4. Information management dimension | 0.158 | 0.297 *** | 0.662 *** | 0.435 *** | 0.303 *** | 0.377 ** | 1 | |
| 3-5. Self-efficacy dimension | 0.360 *** | 0.444 *** | 0.853 *** | 0.396 *** | 0.587 *** | 0.666 *** | 0.424 *** | 1 |
| Self-Management | |||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| Block 1: Sociodemographic and clinical characteristics | |||
| Education level | 0.283 *** | 0.152 * | 0.111 |
| Monthly income | 0.140 | 0.056 | 0.036 |
| GOLD stage | −0.035 | −0.006 | −0.063 |
| mMRC grade | −0.270 ** | −0.180 * | −0.087 |
| Depression | −0.220 ** | −0.168 * | −0.124 |
| Block 2: Spirituality | / | 0.420 *** | 0.250 ** |
| Block 3: Resilience | / | / | 0.378 *** |
| R2 | 0.264 | 0.393 | 0.483 |
| Adjusted R2 | 0.239 | 0.368 | 0.457 |
| ∆ R2 | 0.264 | 0.129 | 0.089 |
| Spirituality → Self-management (Model 1) | |||||
|---|---|---|---|---|---|
| B | SE | β | t | p | |
| Education level | 5.0886 | 2.527 | 0.1517 | 2.0137 | 0.0459 |
| Monthly income | 1.422 | 1.8349 | 0.0562 | 0.775 | 0.4396 |
| GOLD stage | −0.157 | 2.1853 | −0.0057 | −0.0719 | 0.9428 |
| mMRC grade | −11.0263 | 4.7641 | −0.1805 | −2.3144 | 0.0221 |
| Depression | −7.4397 | 3.1037 | −0.1678 | −2.397 | 0.0178 |
| Spirituality | 1.1917 | 0.215 | 0.4198 | 5.5418 | <0.0001 |
| Spirituality →Resilience (Model 2) | |||||
| B | SE | β | t | p | |
| Education level | 1.0639 | 0.752 | 0.1084 | 1.4148 | 0.1593 |
| Monthly income | 0.3948 | 0.546 | 0.0533 | 0.7231 | 0.4708 |
| GOLD stage | 1.2054 | 0.6503 | 0.1506 | 1.8536 | 0.0658 |
| mMRC grade | −4.4063 | 1.4177 | −0.2464 | −3.1081 | 0.0023 |
| Depression | −1.5198 | 0.9236 | −0.1172 | −1.6456 | 0.1020 |
| Spirituality | 0.3731 | 0.064 | 0.4491 | 5.8308 | <0.0001 |
| Spirituality, Resilience →Self-management (Model 3) | |||||
| B | SE | β | t | p | |
| Education level | 3.7162 | 2.3578 | 0.1108 | 1.5761 | 0.1172 |
| Monthly income | 0.9127 | 1.7033 | 0.0361 | 0.5359 | 0.5929 |
| GOLD stage | −1.7121 | 2.049 | −0.0626 | −0.8356 | 0.4048 |
| mMRC grade | −5.3419 | 4.5601 | −0.0874 | −1.1714 | 0.2434 |
| Depression | −5.479 | 2.9028 | −0.1236 | −1.8875 | 0.0611 |
| Spirituality | 0.7104 | 0.2215 | 0.2502 | 3.2067 | 0.0017 |
| Resilience | 1.29 | 0.2595 | 0.3776 | 4.9715 | <0.0001 |
| Spirituality → Self-Management | |||||
|---|---|---|---|---|---|
| Effect | B | SE | Bootstrap 95% CI | p | Effect Ratio |
| Total effect | 1.1917 | 0.2342 | [0.7460–1.6538] | <0.001 | / |
| Direct effect | 0.7104 | 0.2361 | [0.2419–1.1722] | 0.0017 | 59.61% |
| Indirect effect | 0.4813 | 0.1382 | [0.2243–0.7671] | / | 40.39% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Jiang, Y.; Chen, M.; Baiyila, N.; Nan, J. Resilience as a Mediator of the Association between Spirituality and Self-Management among Older People with Chronic Obstructive Pulmonary Disease. Healthcare 2021, 9, 1631. https://doi.org/10.3390/healthcare9121631
Chen Z, Jiang Y, Chen M, Baiyila N, Nan J. Resilience as a Mediator of the Association between Spirituality and Self-Management among Older People with Chronic Obstructive Pulmonary Disease. Healthcare. 2021; 9(12):1631. https://doi.org/10.3390/healthcare9121631
Chicago/Turabian StyleChen, Zhongyi, Yuyu Jiang, Mengjie Chen, Nuerdawulieti Baiyila, and Jiang Nan. 2021. "Resilience as a Mediator of the Association between Spirituality and Self-Management among Older People with Chronic Obstructive Pulmonary Disease" Healthcare 9, no. 12: 1631. https://doi.org/10.3390/healthcare9121631