
Effects of Prehabilitation on Functional Capacity in Aged Patients Undergoing Cardiothoracic Surgeries: A Systematic Review

 ,
,  , and
, and 
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategies and Selection Criteria
2.3. Data Analysis and Assessment of Article Quality
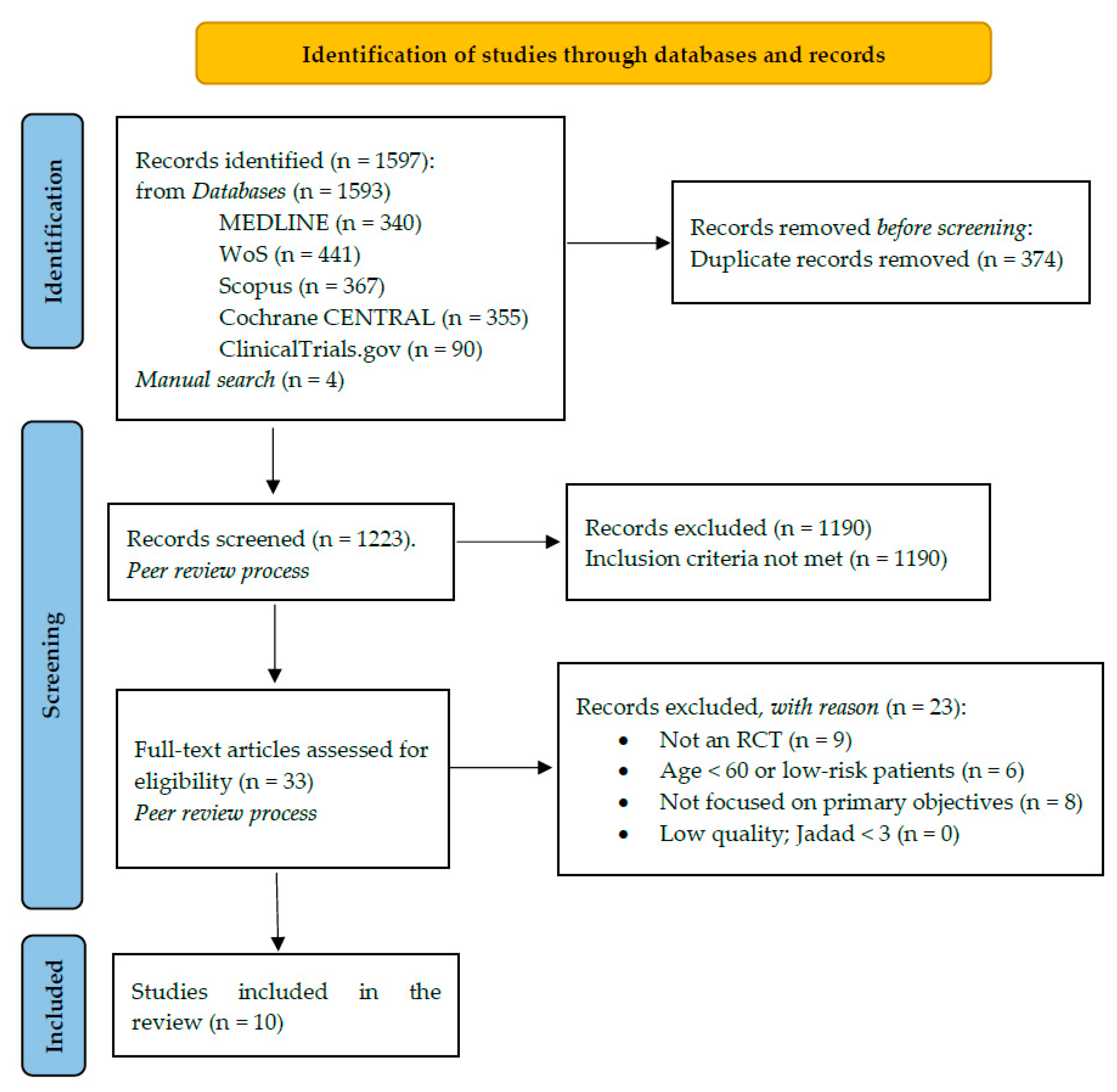
3. Results
3.1. Presentation of the Studies
3.2. Quality Assessment
3.3. Thematic Analysis
3.3.1. Therapeutic Validity
3.3.2. Functional Capacity
3.3.3. Physiological Reserve
3.3.4. Secondary Results
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernandez, F.G.; Shahian, D.M.; Kormos, R.; Jacobs, J.P.; D’Agostino, R.S.; Mayer, J.E.; Kozower, B.D.; Higgins, R.S.; Badhwar, V. The Society of Thoracic Surgeons National Database 2019 Annual Report. Ann. Thorac. Surg. 2019, 108, 1625–1632. [Google Scholar] [CrossRef] [PubMed]
- European Society of Thoracic Surgeons. ESTS Database Annual Report: Silver Book Exeter. 2020. Available online: https://www.ests.org/_userfiles/pages/files/Silver_Book2020_Part1_2_Short_300920OK.pdf (accessed on 3 March 2021).
- Abizanda Soler, P.; Álamo González, C.; Cuesta Triana, F.; Gómez Pavón, J.; González Ramírez, A.; lázaro del Nogal, M.; Matía Martín, P.; Rodríguez Mañas, L. Guía de Buena Práctica Clínica en Geriatría. In Fragilidad y Nutrición en el Anciano; Soc Española Geriatría y Gerontol, 2014; pp. 31–43. Available online: segg.es/media/descargas/GBPCG_Fragilidad_y_nutricion_en_el_anciano.pdf (accessed on 19 November 2021).
- Graham, A.; Brown, C.H. Frailty, Aging, and Cardiovascular Surgery. Anesth. Analg. 2017, 124, 1053–1060. [Google Scholar] [CrossRef] [Green Version]
- Dezube, A.R.; Cooper, L.; Jaklitsch, M.T. Prehabilitation of the Thoracic Surgery Patient. Thorac. Surg. Clin. 2020, 30, 249–258. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). Geneva. 2001. Available online: https://apps.who.int/iris/bitstream/handle/10665/42407/9241545429.pdf (accessed on 10 January 2021).
- Gill, T.M.; Gahbauer, E.A.; Han, L.; Allore, H. Trajectories of Disability in the Last Year of Life. N. Engl. J. Med. 2010, 362, 1173–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charloux, A.; Brunelli, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.-P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. Lung function evaluation before surgery in lung cancer patients: How are recent advances put into practice? A survey among members of the European Society of Thoracic Surgeons (ESTS) and of the Thoracic Oncology Section of the European Respiratory Society (ERS). Interact. Cardiovasc. Thorac. Surg. 2009, 9, 925–931. [Google Scholar] [PubMed]
- Brunelli, A.; Kim, A.W.; Berger, K.I.; Addrizzo-Harris, D.J. Physiologic Evaluation of the Patient with Lung Cancer Being Considered for Resectional Surgery: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e166S–e190S. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Borrell-Vega, J.; Gutierrez, A.G.E.; Humeidan, M.L. Multimodal Prehabilitation Programs for Older Surgical Patients. Anesthesiol. Clin. 2019, 37, 437–452. [Google Scholar] [CrossRef]
- Balagué, C.; Arroyo, A. Prehabilitation: Another step towards the optimization of surgical patients. Cir. Esp. 2020, 98, 175–177. [Google Scholar] [CrossRef]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio Thorac. Surg. 2018, 55, 91–115. [Google Scholar] [CrossRef]
- Gillis, C.; Buhler, K.; Bresee, L.; Carli, F.; Gramlich, L.; Culos-Reed, N.; Sajobi, T.; Fenton, T.R. Effects of Nutritional Prehabilitation, With and Without Exercise, on Outcomes of Patients Who Undergo Colorectal Surgery: A Systematic Review and Meta-analysis. Gastroenterology 2018, 155, 391–410.e4. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.N.; Fonda, H. The Impact of Fitness on Surgical Outcomes: The Case for Prehabilitation. Curr. Sports Med. Rep. 2016, 15, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Granger, C. Preoperative exercise training for patients with non-small cell lung cancer. Cochrane Database Syst. Rev. 2017, 2017, CD012020. [Google Scholar] [CrossRef] [PubMed]
- Hulzebos, E.H.; Smit, Y.; Helders, P.P.; van Meeteren, N.L. Preoperative physical therapy for elective cardiac surgery patients. Cochrane Database Syst. Rev. 2012, 11, 1–42. [Google Scholar] [CrossRef]
- Zheng, Y.-T.; Zhang, J.-X. Preoperative exercise and recovery after cardiac surgery: A meta-analysis. BMC Cardiovasc. Disord. 2020, 20, 2–7. [Google Scholar] [CrossRef]
- Sebio Garcia, R.; Yanez Brage, M.I.; Gimenez Moolhuyzen, E.; Granger, C.L.; Denehy, L. Functional and postoperative outcomes after preoperative exercise training in patients with lung cancer: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 486–497. [Google Scholar] [CrossRef]
- Tew, G.A.; Ayyash, R.; Durrand, J.; Danjoux, G.R. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia 2018, 73, 750–768. [Google Scholar] [CrossRef] [Green Version]
- Hoogeboom, T.J.; Oosting, E.; Vriezekolk, J.E.; Veenhof, C.; Siemonsma, P.C.; De Bie, R.A.; Ende, C.H.M.V.D.; Van Meeteren, N.L.U. Therapeutic Validity and Effectiveness of Preoperative Exercise on Functional Recovery after Joint Replacement: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e38031. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi, A.H.; el Mathari, S.; Abjigitova, D.; Maat, A.P.M.; Taverne, Y.J.J.; Bogers, A.J.C.; Mahtab, E.A. Current and Future Applications of Virtual, Augmented, and Mixed Reality in Cardiothoracic Surgery. Ann. Thorac. Surg. 2020, 18, 1–11. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Li, T.; Higgins, J.; Deeks, J.; Higgins, J.; Thomas, J.; Chnadler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane. 2021. Available online: https://training.cochrane.org/handbook (accessed on 4 May 2021).
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Hearth Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Bhatia, C.; Kayser, B. Preoperative high-intensity interval training is effective and safe in deconditioned patients with lung cancer: A randomized clinical trial. J. Rehabil. Med. 2019, 51, 712–718. [Google Scholar] [CrossRef] [Green Version]
- Lai, Y.; Su, J.; Qiu, P.; Wang, M.; Zhou, K.; Tang, Y.; Che, G. Systematic short-term pulmonary rehabilitation before lung cancer lobectomy: A randomized trial. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Morano, M.T.A.P.; Mesquita, R.; Da Silva, G.P.F.; Araújo, A.S.; Pinto, J.M.D.S.; Neto, A.G.; Viana, C.M.S.; Filho, M.O.D.M.; Pereira, E.D.B. Comparison of the effects of pulmonary rehabilitation with chest physical therapy on the levels of fibrinogen and albumin in patients with lung cancer awaiting lung resection: A randomized clinical trial. BMC Pulm. Med. 2014, 14, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vagvolgyi, A.; Rozgonyi, Z.; Kerti, M.; Agathou, G.; Vadasz, P.; Varga, J. Effectiveness of pulmonary rehabilitation and correlations in between functional parameters, extent of thoracic surgery and severity of post-operative complications: Randomized clinical trial. J. Thorac. Dis. 2018, 10, 3519–3531. [Google Scholar] [CrossRef] [PubMed]
- Sebio García, R.; Yáñez-Brage, M.I.; Giménez Moolhuyzen, E.; Salorio Riobo, M.; Lista Paz, A.; Borro Mate, J.M. Preoperative exercise training prevents functional decline after lung resection surgery: A randomized, single-blind controlled trial. Clin. Rehabil. 2017, 31, 1057–1067. [Google Scholar] [CrossRef]
- Guinan, E.M.; Forde, C.; O’Neill, L.; Gannon, J.; Doyle, S.L.; Valkenet, K.; A Trappenburg, J.C.; Van Hillegersberg, R.; Ravi, N.; Hussey, J.M.; et al. Effect of preoperative inspiratory muscle training on physical functioning following esophagectomy. Dis. Esophagus 2019, 32, 32. [Google Scholar] [CrossRef]
- Minnella, E.M.; Awasthi, R.; Loiselle, S.E.; Agnihotram, R.V.; Ferri, L.E.; Carli, F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: A Randomized Clinical Trial. JAMA Surg. 2018, 153, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- Steinmetz, C.; Bjarnason-Wehrens, B.; Baumgarten, H.; Walther, T.; Mengden, T.; Walther, C. Prehabilitation in patients awaiting elective coronary artery bypass graft surgery—Effects on functional capacity and quality of life: A randomized controlled trial. Clin. Rehabil. 2020, 34, 1256–1267. [Google Scholar] [CrossRef]
- Stammers, A.N. Optimizing the Pre-Operative Risk Profile of Older Adults Undergoing Elective Cardiac Surgery: A Randomized Controlled Trial. University of Manitoba. 2016. Available online: https://mspace.lib.umanitoba.ca/xmlui/bitstream/handle/1993/31737/stammers_andrew.pdf?sequence=1&isAllowed=y (accessed on 8 June 2021).
- Kamarajah, S.K.; Bundred, J.; Weblin, J.; Tan, B.H. Critical appraisal on the impact of preoperative rehabilitation and outcomes after major abdominal and cardiothoracic surgery: A systematic review and meta-analysis. Surgery 2020, 167, 540–549. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, F.; Abete, P.; Mazzella, F.; Furgi, G.; Nicolino, A.; Longobardi, G.; Testa, G.; Langellotto, A.; Infante, T.; Napoli, C.; et al. Six-minute walking test but not ejection fraction predicts mortality in elderly patients undergoing cardiac rehabilitation following coronary artery bypass grafting. Eur. J. Prev. Cardiol. 2012, 19, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Tahir, M.R.; Bongers, B.C.; Kallen, V.L.; Slooter, G.D.; van Meeteren, N.L. Prehabilitation before major intra-abdominal cancer surgery: A systematic review of randomised controlled trials. Eur. J. Anaesthesiol. 2019, 36, 933–945. [Google Scholar] [CrossRef]
- Jones, L.W.; Ms, C.J.P.; Eves, N.D.; Haykowsky, M.J.; Courneya, K.S.; Mackey, J.R.; Joy, A.A.; Kumar, V.; Winton, T.W.; Reiman, T. Effects of presurgical exercise training on cardiorespiratory fitness among patients undergoing thoracic surgery for malignant lung lesions. Cancer 2007, 110, 590–598. [Google Scholar] [CrossRef]
- Rosero, I.D.; Ramírez-Vélez, R.; Lucia, A.; Martínez-Velilla, N.; Santos-Lozano, A.; Valenzuela, P.L.; Morilla, I.; Izquierdo, M. Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer. Cancers 2019, 11, 944. [Google Scholar] [CrossRef] [Green Version]
- Jastrzębski, D.; Żebrowska, A.; Rutkowski, S.; Rutkowska, A.; Warzecha, J.; Ziaja, B.; Pałka, A.; Czyżewska, B.; Czyżewski, D.; Ziora, D. Pulmonary Rehabilitation with a Stabilometric Platform After Thoracic Surgery: A Preliminary Report. J. Hum. Kinet. 2018, 65, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Lemanu, D.P.; Singh, P.P.; MacCormick, A.D.; Arroll, B.; Hill, A.G. Effect of Preoperative Exercise on Cardiorespiratory Function and Recovery After Surgery: A Systematic Review. World J. Surg. 2013, 37, 711–720. [Google Scholar] [CrossRef]
- Pompili, C.; Brunelli, A.; Xiumé, F.; Refai, M.; Salati, M.; Sabbatini, A. Predictors of postoperative decline in quality of life after major lung resections. Eur. J. Cardio-Thorac. Surg. 2011, 39, 732–737. [Google Scholar] [CrossRef]
- Yau, D.K.W.; Underwood, M.J.; Joynt, G.M.; Lee, A. Effect of preparative rehabilitation on recovery after cardiac surgery: A systematic review. Ann. Phys. Rehabil. Med. 2021, 64, 101391. [Google Scholar] [CrossRef]
- Hulzebos, E.H.; Helders, P.J.; Favié, N.J.; De Bie, R.A.; de la Riviere, A.B.; Van Meeteren, N.L. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: A randomized clinical trial. J. Am. Med. Assoc. 2006, 296, 1851–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutron, I.; Guittet, L.; Estellat, C.; Moher, D.; Hróbjartsson, A.; Ravaud, P. Reporting Methods of Blinding in Randomized Trials Assessing Nonpharmacological Treatments. PLoS Med. 2007, 4, e61. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Costa, D.; Gómez-Salgado, J.; Castillejo del Río, A.; Borrallo-Riego, Á.; Guerra-Martín, M.D. Effects of Prehabilitation on Functional Capacity in Aged Patients Undergoing Cardiothoracic Surgeries: A Systematic Review. Healthcare 2021, 9, 1602. https://doi.org/10.3390/healthcare9111602
Fernández-Costa D, Gómez-Salgado J, Castillejo del Río A, Borrallo-Riego Á, Guerra-Martín MD. Effects of Prehabilitation on Functional Capacity in Aged Patients Undergoing Cardiothoracic Surgeries: A Systematic Review. Healthcare. 2021; 9(11):1602. https://doi.org/10.3390/healthcare9111602
Chicago/Turabian StyleFernández-Costa, Damián, Juan Gómez-Salgado, Andrés Castillejo del Río, Álvaro Borrallo-Riego, and María Dolores Guerra-Martín. 2021. "Effects of Prehabilitation on Functional Capacity in Aged Patients Undergoing Cardiothoracic Surgeries: A Systematic Review" Healthcare 9, no. 11: 1602. https://doi.org/10.3390/healthcare9111602