
Machine Learning for Predicting the Risk for Childhood Asthma Using Prenatal, Perinatal, Postnatal and Environmental Factors

Abstract
:1. Introduction
2. Materials and Methods
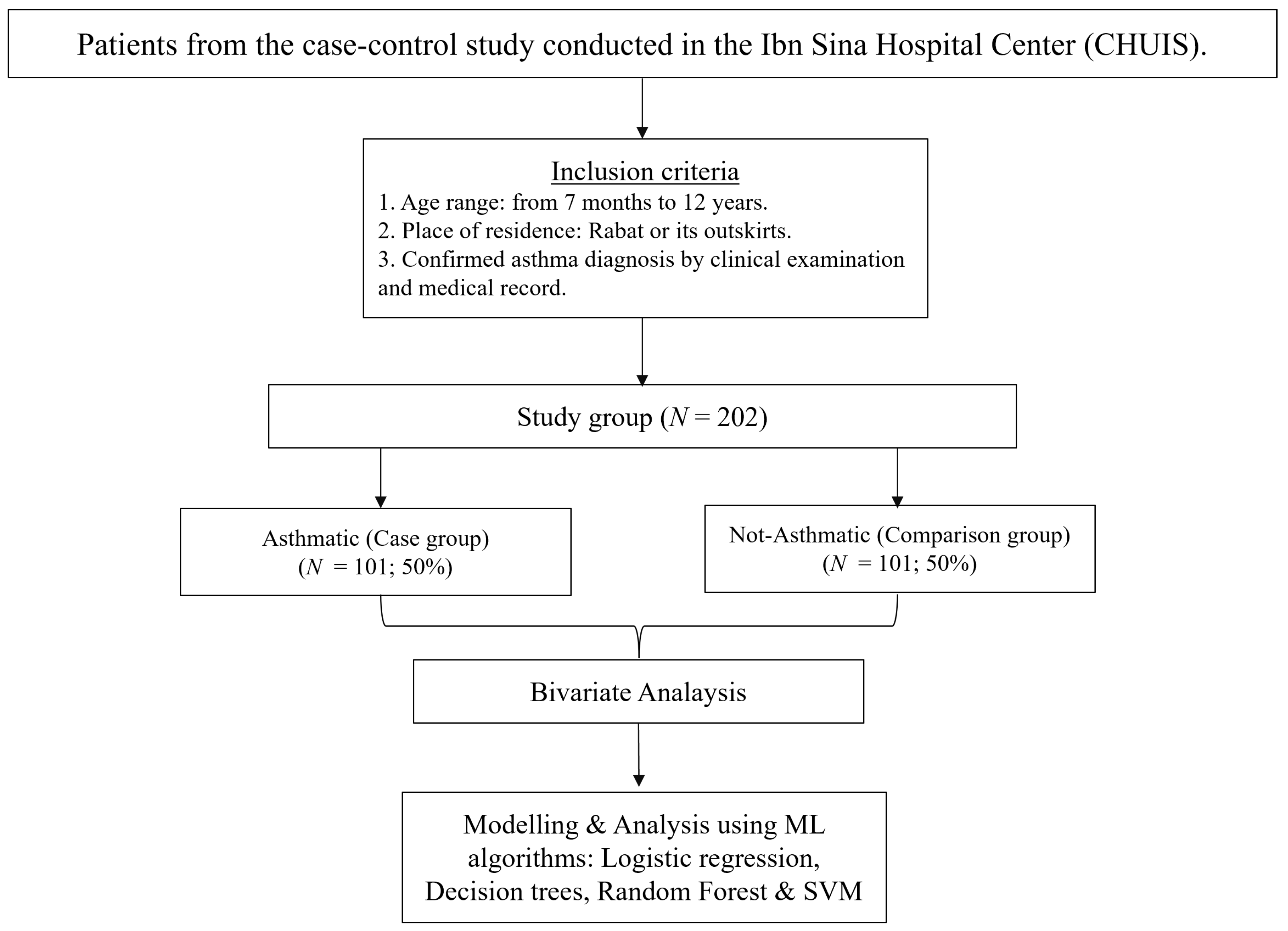
2.1. Data Collection
2.2. Inclusion Criteria
- Age range: this ranges from 7 months to 12 years.
- Place of residence: only patients living in the city of Rabat or its outskirts were included in the study.
- Confirmed asthma diagnosis: the diagnosis was based on a clinical examination by a pediatrician who assessed tangible symptoms such as wheezing, chest tightness, difficulty in breathing induced by physical exercise and dry coughs, especially at night.
2.3. Data Analysis
3. Results
3.1. Logistic Regression
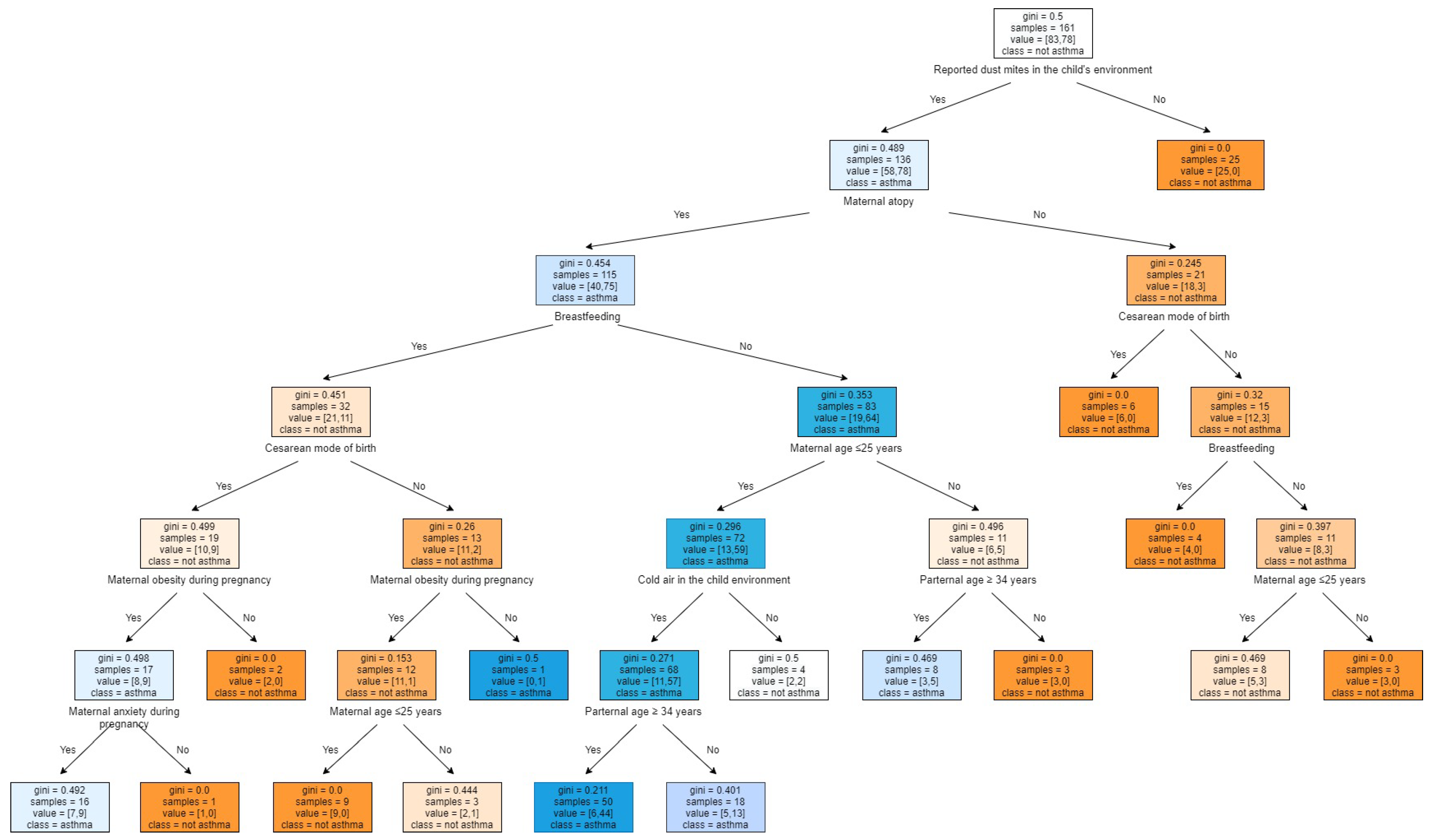
3.2. Decision Tree Model
- The predicted class (‘Asthma’ or ‘Not asthma’).
- The predicted probability of asthma diagnosis.
- The percentage of observations in the node.
3.3. Random Forest Model
3.4. Support Vector Machine
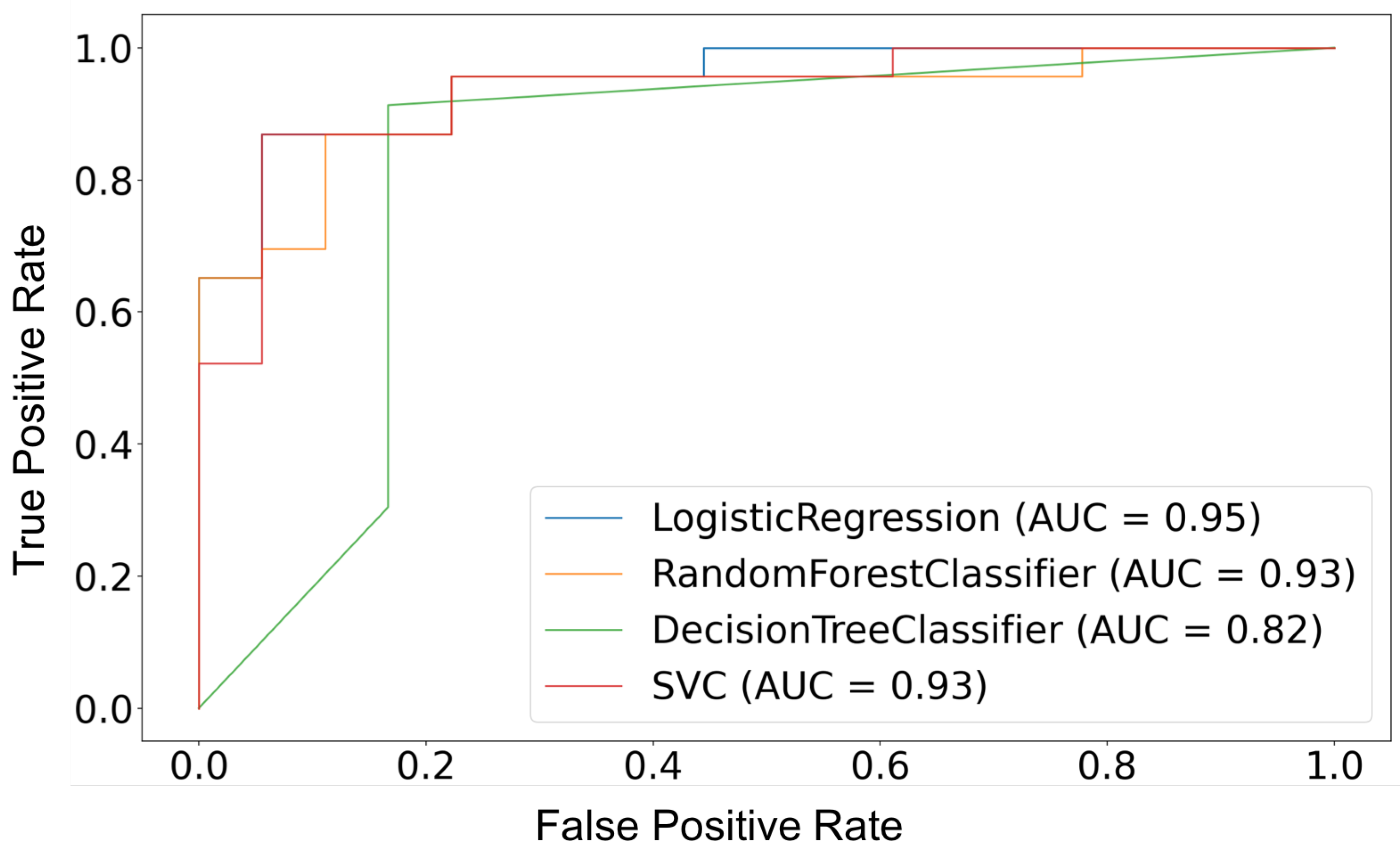
3.5. Comparison of Performance of Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Asthma Fact Sheet. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/asthma (accessed on 3 May 2021).
- Wadden, D.; Farrell, J.; Smith, M.J.; Twells, L.K.; Gao, Z. Maternal history of asthma modifies the risk of childhood persistent asthma associated with maternal age at birth: Results from a large prospective cohort in Canada. J. Asthma 2021, 58, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, C.; Sheikh, A.; Nwaru, B.I. Prenatal maternal psychosocial stress and risk of asthma and allergy in their offspring: Protocol for a systematic review and meta-analysis. NPJ Prim. Care Respir. Med. 2016, 26, 16021. [Google Scholar] [CrossRef]
- Yang, H.J. Impact of perinatal environmental tobacco smoke on the development of childhood allergic diseases. Korean J. Pediatr. 2016, 59, 319. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I. Recent perspectives on global epidemiology of asthma in childhood. Allergol. Immunopathol. 2010, 38, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Martino, D.; Prescott, S. Epigenetics and prenatal influences on asthma and allergic airways disease. Chest 2011, 139, 640–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nafti, S.; Taright, S.; El Ftouh, M.; Yassine, N.; Benkheder, A.; Bouacha, H.; Fakhfakh, H.; Ali-Khoudja, M.; Texier, N.; El Hasnaoui, A. Prevalence of asthma in North Africa: The Asthma Insights and Reality in the Maghreb (AIRMAG) study. Respir. Med. 2009, 103, S2–S11. [Google Scholar] [CrossRef] [Green Version]
- Subbarao, P.; Becker, A.; Brook, J.R.; Daley, D.; Mandhane, P.J.; Miller, E.G.; Turvey, E.S.; Sears, M.R. Epidemiology of asthma: Risk factors for development. Expert Rev. Clin. Immunol. 2009, 5, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Kashanian, M.; Mohtashami, S.S.; Bemanian, M.H.; Moosavi, S.A.J.; Moradi Lakeh, M. Evaluation of the associations between childhood asthma and prenatal and perinatal factors. Int. J. Gynecol. Obstet. 2017, 137, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Oliveti, J.F.; Kercsmar, C.M.; Redline, S. Pre-and perinatal risk factors for asthma in inner city African-American children. Am. J. Epidemiol. 1996, 143, 570–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midodzi, W.K.; Rowe, B.H.; Majaesic, C.M.; Saunders, L.D.; Senthilselvan, A. Early life factors associated with incidence of physician-diagnosed asthma in preschool children: Results from the Canadian Early Childhood Development cohort study. J. Asthma 2010, 47, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.; Roberts, S.E.; Wotton, C.J.; Goldacre, M.J. Influence of maternal and perinatal factors on subsequent hospitalisation for asthma in children: Evidence from the Oxford record linkage study. BMC Pulm. Med. 2010, 10, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douwes, J.; Cheng, S.; Travier, N.; Cohet, C.; Niesink, A.; McKenzie, J.; Cunningham, C.; Le Gros, G.; von Mutius, E.; Pearce, N. Farm exposure in utero may protect against asthma, hay fever and eczema. Eur. Respir. J. 2008, 32, 603–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arif, A.A.; Veri, S.D. The association of prenatal risk factors with childhood asthma. J. Asthma 2019, 56, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Gryech, I.; Ghogho, M.; Elhammouti, H.; Sbihi, N.; Kobbane, A. Machine learning for air quality prediction using meteorological and traffic related features. J. Ambient. Intell. Smart Environ. Prepr. 2020, 12, 379–391. [Google Scholar] [CrossRef]
- Vidnerová, P.; Neruda, R. Sensor Data Air Pollution Prediction by Kernel Models. In Proceedings of the 2016 16th IEEE/ACM International Symposium on Cluster, Cloud and Grid Computing (CCGrid), Cartagena, Colombia, 16–19 May 2016; pp. 666–673. [Google Scholar] [CrossRef]
- Smola, A.J.; Schölkopf, B. A tutorial on support vector regression. Stat. Comput. 2004, 14, 199–222. [Google Scholar] [CrossRef] [Green Version]
- Illi, S.; Weber, J.; Zutavern, A.; Genuneit, J.; Schierl, R.; Strunz-Lehner, C.; von Mutius, E. Perinatal influences on the development of asthma and atopy in childhood. Ann. Allergy Asthma Immunol. 2014, 112, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.J.; Nafstad, P.; Magnus, P. Environmental tobacco smoke, parental atopy, and childhood asthma. Environ. Health Perspect. 2001, 109, 579–582. [Google Scholar] [CrossRef]
- Laerum, B.N.; Svanes, C.; Wentzel-Larsen, T.; Gulsvik, A.; Torén, K.; Norrman, E.; Gíslason, T.; Janson, C.; Omenaas, E. Young maternal age at delivery is associated with asthma in adult offspring. Respir. Med. 2007, 101, 1431–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherriff, A.; Peters, T.J.; Henderson, J.; Strachan, D. Risk factor associations with wheezing patterns in children followed longitudinally from birth to 3(1/2) years. Int. J. Epidemiol. 2001, 30, 1473–1484. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, A.M.L.; Ehrenstein, V.; Riis, A.H.; Toft, G.; Mikkelsen, E.M.; Olsen, J. The potential impact of paternal age on risk of asthma in childhood: A study within the Danish National Birth Cohort. Respir. Med. 2018, 137, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almqvist, C.; Olsson, H.; Ullemar, V.; D’Onofrio, B.M.; Frans, E.; Lundholm, C. Association between parental age and asthma in a population-based register study. J. Allergy Clin. Immunol. 2015, 136, 1103–1105.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gryech, I.; Ben-Aboud, Y.; Guermah, B.; Sbihi, N.; Ghogho, M.; Kobbane, A. MoreAir: A Low-Cost Urban Air Pollution Monitoring System. Sensors 2020, 20, 998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Rodriguez, J.A.; Forno, E.; Rodriguez-Martinez, C.E.; Celedón, J.C. Risk and protective factors for childhood asthma: What is the evidence? J. Allergy Clin. Immunol. Pract. 2016, 4, 1111–1122. [Google Scholar] [CrossRef] [Green Version]
- Segura, N.; Fraj, J.; Cubero, J.; Sobrevía, M.; Lezaun, A.; Ferrer, L.; Sebastián, A.; Colás, C. Mould and grass pollen allergy as risk factors for childhood asthma in Zaragoza, Spain. Allergol. Immunopathol. 2016, 44, 455–460. [Google Scholar] [CrossRef]
- Celedón, J.C.; Milton, D.K.; Ramsey, C.D.; Litonjua, A.A.; Ryan, L.; Platts-Mills, T.A.; Gold, D.R. Exposure to dust mite allergen and endotoxin in early life and asthma and atopy in childhood. J. Allergy Clin. Immunol. 2007, 120, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Murrison, L.B.; Brandt, E.B.; Myers, J.B.; Hershey, G.K.K. Environmental exposures and mechanisms in allergy and asthma development. J. Clin. Investig. 2019, 129, 1504–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulder, B.; Pouwels, K.B.; Schuiling-Veninga, C.C.M.; Bos, H.J.; De Vries, T.W.; Jick, S.S.; Hak, E. Antibiotic use during pregnancy and asthma in preschool children: The influence of confounding. Clin. Exp. Allergy 2016, 46, 1214–1226. [Google Scholar] [CrossRef] [PubMed]
- McKeever, T.M.; Lewis, S.A.; Smith, C.; Hubbard, R. The importance of prenatal exposures on the development of allergic disease: A birth cohort study using the West Midlands General Practice Database. Am. J. Respir. Crit. Care Med. 2002, 166, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.H.; Kuo, H.F.; Huang, C.H.; Yang, S.N.; Lee, M.S.; Hung, C.H. Early life exposure to antibiotics and the risk of childhood allergic diseases: An update from the perspective of the hygiene hypothesis. J. Microbiol. Immunol. Infect. 2013, 46, 320–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bager, P.; Wohlfahrt, J.; Westergaard, T. Caesarean delivery and risk of atopy and allergic disesase: Meta-analyses. Clin. Exp. Allergy 2008, 38, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Thavagnanam, S.; Fleming, J.; Bromley, A.; Shields, M.D.; Cardwell, C.R. A meta-analysis of the association between Caesarean section and childhood asthma. Clin. Exp. Allergy 2008, 38, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Sitarik, A.R.; Kasmikha, N.S.; Kim, H.; Wegienka, G.; Havstad, S.; Ownby, D.; Zoratti, E.; Johnson, C.C. Breast-feeding and delivery mode modify the association between maternal atopy and childhood allergic outcomes. J. Allergy Clin. Immunol. 2018, 142, 2002–2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pluymen, L.P.; Smit, H.A.; Wijga, A.H.; Gehring, U.; De Jongste, J.C.; Van Rossem, L. Cesarean delivery, overweight throughout childhood, and blood pressure in adolescence. J. Pediatr. 2016, 179, 111–117. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 202) | Children with Asthma (N = 101, 50%) | Children without Asthma (N = 101, 50%) | Chi-Square Test (p-Value) |
|---|---|---|---|
| Factors related to family history | |||
| Maternal atopy | 28 (84.85%) | 5 (15.15%) | 1.263 |
| Paternal atopy | 17 (65.38%) | 9 (34.62%) | 0.09361 |
| History of an atopic disease in brothers or sisters | 9 (56.25%) | 7 (43.75%) | 0.6032 |
| Personal atopic dermatitis | 13 (61.90%) | 8 (0.3809524) | 0.2502 |
| Factors related to the child environment | |||
| Reported dust mites in the child environment | 31 (96.87%) | 1 (3.13%) | 8.089 |
| Reported pets (cats) in the child environment | 7 (77.78%) | 2 (22.22%) | 0.08897 |
| Reported pollen in the child environment | 13 (0.7222222) | 5 (27.78%) | 0.04875 |
| Reported mold in the child environment | 12 (85.71%) | 2 (14.20%) | 0.005719 |
| Reported cold airflow in the child environment | 15 (83.34%) | 3 (16.67%) | 0.003115 |
| Reported respiratory infections in family members (cold) | 23 (76.67%) | 7 ( 23.34%) | 0.001589 |
| Reported respiratory infections in family members (flu) | 15 (62.50%) | 9 (37.5%) | 0.1931 |
| Reported respiratory infections in family members (sinusitis) | 5 (83.34%) | 1 (16.67%) | 0.09819 |
| Prenatal, Perinatal and postnatal factors | |||
| Maternal age ≤ 25 years | 33 (76.75%) | 10 (23.26%) | 8.027 |
| Maternal age ≥ 35 years | 5 (62.5%) | 3 (37.50%) | 0.4717 |
| Paternal age ≤ 24 years | (62.50%) | (37.50%) | 0.4717 |
| Paternal age ≥ 34 years | 22 (%) | 7 (%) | 0.002679 |
| Maternal obesity during pregnancy | 15 (75%) | 5 (25%) | 0.01878 |
| Maternal anxiety during pregnancy | 16 (69.57%) | 7 (30.43%) | 0.04674 |
| Exposure to secondhand smoking during pregnancy | 25 (56.82%) | 19 (43.18%) | 0.3076 |
| Consumption of antibiotics/paracetamol during pregnancy | 9 (90%) | 1 (10%) | 0.009641 |
| Underweight child | 9 (75%) | 3 (25%) | 0.07483 |
| Overweight child | 15 (68.18%) | 7 (31.81%) | 0.07149 |
| Prematurity | 5 (62.50%) | 3 (37.50%) | 0.4717 |
| Cesarian mode of birth | 59 (60.83%) | 38 (39.17%) | 0.003177 |
| Breastfeeding | 55 (38.73%) | 87 (61.27%) | 8.876 |
| dietary diversity for children aged between 4 and 6 months | 21 (37.50%) | 35 ( 62.50%) | 0.02816 |
| dietary diversity for children aged more than 6 months | 80 (54.79%) | 66 (45.20%) | 0.02816 |
| Factors related to early childhood | |||
| Overweight during the first 2 years | 11 (78.57%) | 3 (21.43%) | 0.02705 |
| Consumption of antibiotics during first 2 years | 32 (74.42%) | 11 ( 25.58%) | 0.0003174 |
| Exposure to pollution in the first two years | 14 (60.87%) | 9 (39.13%) | 0.2693 |
| Variable | OR | 2.5% | 97.5% |
|---|---|---|---|
| Maternal atopy | 19.04 | 3.83 | 126.39 |
| Reported dust mites in the child’s environment | 101.23 | 13.39 | 2271.27 |
| Maternal age ≤ 25 years | 7.19 | 1.81 | 33.17 |
| Maternal age ≥ 35 years | 53.13 | 4.24 | 850.82 |
| Cold air in the child environment | 21.62 | 2.18 | 335.19 |
| Respiratory infections in family members (cold) | 5.98 | 1.32 | 31.15 |
| Respiratory infections in family members (flu) | 11.61 | 2.31 | 76.33 |
| Paternal age ≥ 34 years | 13.50 | 2.66 | 84.79 |
| Cesarean mode of birth | 6.77 | 2.12 | 25.75 |
| Breastfeeding in the first two years | 0.03 | 0.01 | 0.12 |
| Dietary diversity for children aged between 4 and 6 months | 0.35 | 0.09 | 1.24 |
| Variable | Mean Decrease Gini |
|---|---|
| Breastfeeding | 9.49 |
| Reported dust mites in the child’s environment | 9.37 |
| Maternal atopy | 4.93 |
| Cesarean mode of birth | 4.18 |
| Maternal age of ≤25 years | 3.99 |
| Antibiotic use during the first 2 years | 3.59 |
| Respiratory infections in family members (cold) | 3.41 |
| Paternal age of ≤25 years | 2.85 |
| Maternal obesity during pregnancy | 2.05 |
| Respiratory infections in family members (flu) | 1.89 |
| Consumption of antibiotics/paracetamol during pregnancy | 1.77 |
| Dietary diversity for children aged between 4 months and 6 months old | 1.72 |
| Dietary diversity for children aged more than 6 months | 1.62 |
| Cold airflow in the child environment | 1.57 |
| Strong odors in the child’s environment | 1.39 |
| Overweight in the first 2 years | 1.27 |
| Pollen in the child environment | 1.14 |
| Mold in the child environment | 0.99 |
| Maternal age of ≥35 years | 0.82 |
| Performance Metrics | Logistic Regression | Decision Tree | Random Forest | SVM |
|---|---|---|---|---|
| F1 score (y = Asthmatic) | 0.89 | 0.87 | 0.86 | 0.81 |
| F1 score (y = Not Asthmatic) | 0.83 | 0.82 | 0.89 | 0.80 |
| Accuracy (%) | 85.36 | 85.3 | 87.8 | 80 |
| Average accuracy for 10-fold cross validation (%) | 82.57 | 75.19 | 84.9 | 82.5 |
| Sensitivity, Sn (%) | 83 | 91 | 87 | 67 |
| Specificity, Sp (%) | 88 | 78 | 88 | 94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeddi, Z.; Gryech, I.; Ghogho, M.; EL Hammoumi, M.; Mahraoui, C. Machine Learning for Predicting the Risk for Childhood Asthma Using Prenatal, Perinatal, Postnatal and Environmental Factors. Healthcare 2021, 9, 1464. https://doi.org/10.3390/healthcare9111464
Jeddi Z, Gryech I, Ghogho M, EL Hammoumi M, Mahraoui C. Machine Learning for Predicting the Risk for Childhood Asthma Using Prenatal, Perinatal, Postnatal and Environmental Factors. Healthcare. 2021; 9(11):1464. https://doi.org/10.3390/healthcare9111464
Chicago/Turabian StyleJeddi, Zineb, Ihsane Gryech, Mounir Ghogho, Maryame EL Hammoumi, and Chafiq Mahraoui. 2021. "Machine Learning for Predicting the Risk for Childhood Asthma Using Prenatal, Perinatal, Postnatal and Environmental Factors" Healthcare 9, no. 11: 1464. https://doi.org/10.3390/healthcare9111464