
Clinical Outcomes of Genotype-Matched Therapy for Recurrent Gynecological Cancers: A Single Institutional Experience

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient’s Clinical Information and Genome Sequence
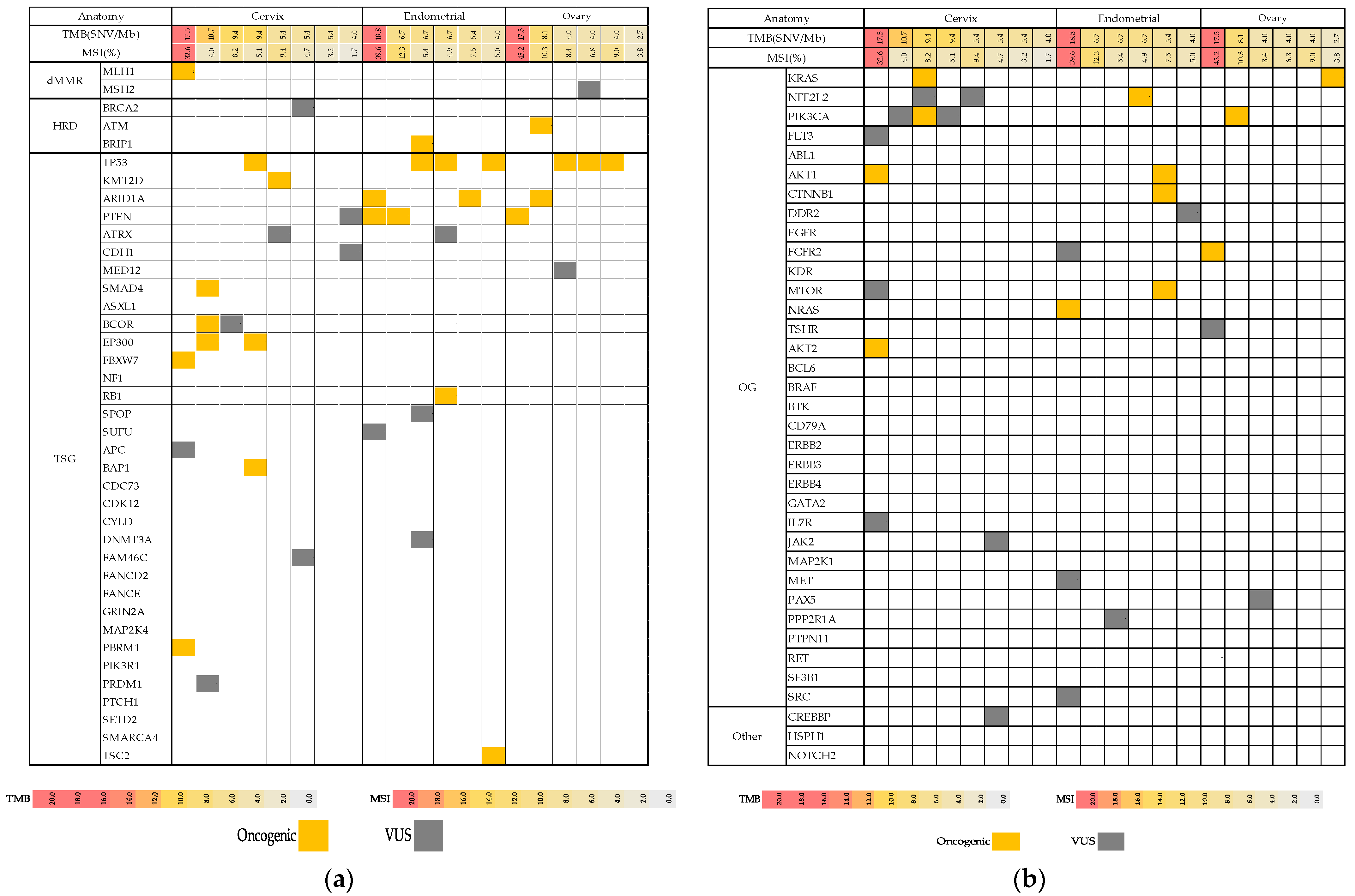
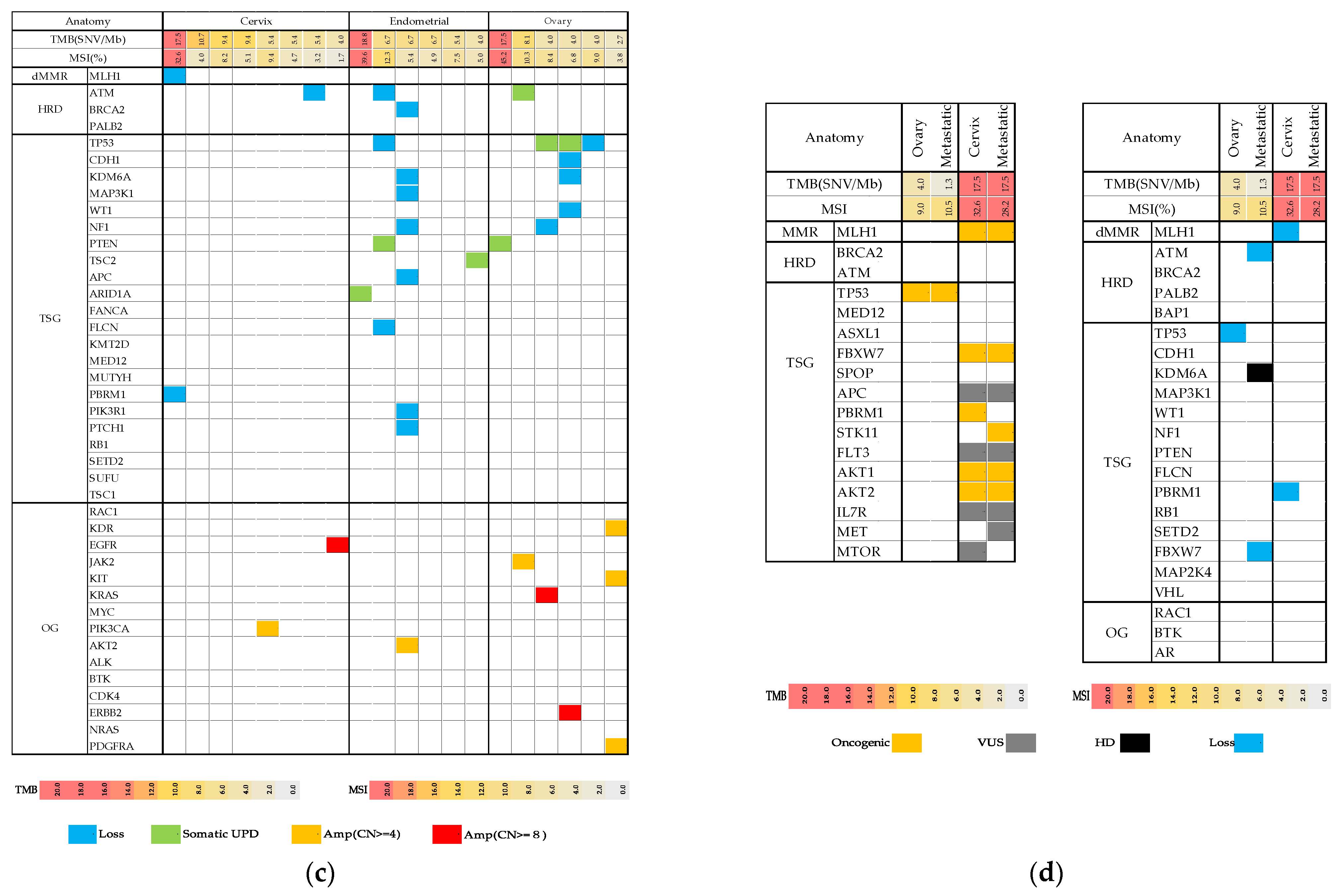
2.2. Mutation Map
2.3. Genotype-Matched Therapy
2.4. Three Cases of Successful Genotyped-Matched Therapy
2.4.1. Case 1
2.4.2. Case 2
2.4.3. Case 3
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Genomic Analysis
4.3. Definition of Actionable and Druggable Variants
CGB
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Registry and Statistics. Cancer Information Service, National Cancer Center Japan Cancer Statistics in Japan. Available online: https://ganjoho.jp/en/professional/statistics/table_download.html (accessed on 16 February 2021).
- Oronsky, B.; Ray, C.M.; Spira, A.I.; Trepel, J.B.; Carter, C.A.; Cottrill, H.M. A brief review of the management of platinum-resistant-platinum-refractory ovarian cancer. Med. Oncol. 2017, 34, 103. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Redig, A.J.; Jänne, P.A. Basket trials and the evolution of clinical trial design in an era of genomic medicine. J. Clin. Oncol. 2015, 33, 975–977. [Google Scholar] [CrossRef] [Green Version]
- Willyard, C. ‘Basket studies’ will hold intricate data for cancer drug approvals. Nat. Med. 2013, 19, 655. [Google Scholar] [CrossRef]
- Colon-Otero, G.; John Weroha, S.; Foster, N.R.; Haluska, P.; Hau, X.; Wahner-Hendrickson, A.; Jatoi, A.; Block, M.; Dihn, T. Phase 2 trial of everolimus and letrozole in relapsed estrogen receptor-positive high-grade ovarian cancers. Gynecol. Oncol. 2017, 146, 64–68. [Google Scholar] [CrossRef]
- Nakamura, K.; Aimono, E.; Tanishima, S.; Imai, M.; Nagatsuma, A.K.; Hayashi, H.; Yoshimura, Y.; Nakayama, K.; Kyo, S.; Nishihara, H. Olaparib Monotherapy for BRIP1-Mutated High-Grade Serous Endometrial Cancer. JCO Precis. Oncol. 2020, 4, PO.19.00368. [Google Scholar] [CrossRef]
- Toomey, S.; Carr, A.; Mezynski, M.J.; Elamin, Y.; Rafee, S.; Cremona, M.; Morgan, C.; Madden, S.; Abdul-Jalil, K.I.; Gately, K.; et al. Identification and clinical impact of potentially actionable somatic oncogenic mutations in solid tumor samples. J. Transl. Med. 2020, 18, 99. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Freixinos, V.; Ruiz-Pace, F.; Fariñas-Madrid, L.; Garrido-Castro, A.C.; Villacampa, G.; Nuciforo, P.; Vivancos, A.; Dienstmann, R.; Oaknin, A. Genomic heterogeneity and efficacy of PI3K pathway inhibitors in patients with gynaecological cancer. ESMO Open. 2019, 4, e000444. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.S.; Huang, H.D.; Yeh, K.T.; Chang, J.G. Genetic alterations in endometrial cancer by targeted next-generation sequencing. Exp. Mol. Pathol. 2016, 100, 8–12. [Google Scholar] [CrossRef]
- Slomovitz, B.M.; Lu, K.H.; Johnston, T.; Coleman, R.L.; Munsell, M.; Broaddus, R.R.; Walker, C.; Ramondetta, L.M.; Burke, T.W.; Gershenson, D.M.; et al. A phase 2 study of the oral mammalian target of rapamycin inhibitor, everolimus, in patients with recurrent endometrial carcinoma. Cancer 2010, 116, 5415–5419. [Google Scholar] [CrossRef] [Green Version]
- Makker, V.; Recio, F.O.; Ma, L.; Matulonis, U.; O’Hara Lauchle, J.; Parmar, H.; Gilbert, H.; Wang, Y.; Koeppen, H.; Spoerke, J.M.; et al. Phase II trial of GDC-0980 (dual PI3K/mTOR inhibitor) in patients with advanced endometrial carcinoma: Final study results. J. Clin. Oncol. 2014, 32, 5513. [Google Scholar] [CrossRef]
- Tourneau, C.L.; Delord, J.P.; Gonçalves, A.; Gavoille, C.; Dubot, C.; Isambert, N.; Campone, M.; Trédan, O.; Massiani, M.A.; Mauborgne, C.; et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): A multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015, 16, 1324–1334. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Massard, C.; Michiels, S.; Ferté, C.; Le Deley, M.C.; Lacroix, L.; Hollebecque, A.; Verlingue, L.; Ileana, E.; Rosellini, S.; Ammari, S.; et al. High-Throughput Genomics and Clinical Outcome in Hard-to-Treat Advanced Cancers: Results of the MOSCATO 01 Trial. Cancer Discov. 2017, 7, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Sunami, K.; Ichikawa, H.; Kubo, T.; Kato, M.; Fujiwara, Y.; Shimomura, A.; Koyama, T.; Kakishima, H.; Kitami, M.; Matsushita, H.; et al. Feasibility and utility of a panel testing for 114 cancer-associated genes in a clinical setting: A hospital-based study. Cancer Sci. 2019, 110, 1480–1490. [Google Scholar] [CrossRef] [Green Version]
- Tsimberidou, A.M.; Iskander, N.G.; Hong, D.S.; Wheler, J.J.; Falchook, G.S.; Fu, S.; Piha-Paul, S.; Naing, A.; Janku, F.; Luthra, R.; et al. Personalized medicine in a phase I clinical trials program: The MD Anderson Cancer Center initiative. Clin. Cancer Res. 2012, 18, 6373–6383. [Google Scholar] [CrossRef] [Green Version]
- Wheler, J.J.; Janku, F.; Naing, A.; Li, Y.; Stephen, B.; Zinner, R.; Subbiah, V.; Fu, S.; Karp, D.; Falchook, G.S.; et al. Cancer Therapy Directed by Comprehensive Genomic Profiling: A Single Center Study. Cancer Res. 2016, 76, 3690–3701. [Google Scholar] [CrossRef] [Green Version]
- Seol, Y.M.; Kwon, C.H.; Lee, S.J.; Lee, S.J.; Choi, Y.; Choi, Y.J.; Kim, H.; Park, D.Y. A Pilot Prospective Study of Refractory Solid Tumor Patients for NGS-Based Targeted Anticancer Therapy. Transl. Oncol. 2019, 12, 301–307. [Google Scholar] [CrossRef]
- Bitzer, M.; Ostermann, L.; Horger, M.; Biskup, S.; Schulze, M.; Ruhm, K.; Hilke, F.; öner, ö.; Nikilaou, K.; Schroeder, C.; et al. Next-Generation Sequencing of Advanced GI Tumors Reveals Individual Treatment Options. JCO Precis. Oncol. 2020, 4, 258–271. [Google Scholar] [CrossRef]
- Sultova, E.; Westphalen, C.B.; Jung, A.; Kumbrink, J.; Kirchner, T.; Mayr, D.; Rudelius, M.; Ormanns, S.; Heinemann, V.; Metzeler, K.H.; et al. Implementation of Precision Oncology for Patients with Metastatic Breast Cancer in an Interdisciplinary. Diagnostics 2021, 11, 733. [Google Scholar] [CrossRef]
- André, F.; Bachelot, T.; Commo, F.; Campone, M.; Arnedos, M.; Dieras, V.; Lacroix-Triki, M.; Lacroix, L.; Cohen, P.; Gentien, D.; et al. Comparative genomic hybridisation array and DNA sequencing to direct treatment of metastatic breast cancer: A multicentre, prospective trial (SAFIR01/UNICANCER). Lancet Oncol. 2014, 15, 267–274. [Google Scholar] [CrossRef]
- Janku, F.; Tsimberidou, A.M.; Garrido-Laguna, I.; Wang, X.; Luthra, R.; Hong, D.S.; Naing, A.; Falchook, G.S.; Moroney, J.W.; Piha-Paul, S.A.; et al. PIK3CA mutations in patients with advanced cancers treated with PI3K/AKT/mTOR axis inhibitors. Mol. Cancer Ther. 2011, 10, 558–565. [Google Scholar] [CrossRef] [Green Version]
- Catasus, L.; D’Angelo, E.; Pons, C.; Espinosa, I.; Prat, J. Expression profiling of 22 genes involved in the PI3K-AKT pathway identifies two subgroups of high-grade endometrial carcinomas with different molecular alterations. Mod. Pathol. 2010, 23, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Slomovitz, B.M.; Jiang, Y.; Yates, M.S.; Soliman, P.T.; Johnston, T.; Nowakowski, M.; Levenback, C.; Zhang, Q.; Ring, K.; Munsell, M.F.; et al. Phase II study of everolimus and letrozole in patients with recurrent endometrial carcinoma. J. Clin. Oncol. 2015, 33, 930–936. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, H.; Tanishima, S.; Fujii, K.; Mori, R.; Okada, C.; Yanagita, E.; Shibata, Y.; Matsuoka, R.; Amano, T.; Yamada, T.; et al. Clinical impact of a cancer genomic profiling test using an in-house comprehensive targeted sequencing system. Cancer Sci. 2020, 111, 3926–3937. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | |
|---|---|
| Median (range) | 58.5 (39–75) |
| Tumor type, n (%) | |
| cervical cancer | 8 (40%) |
| endometrial cancer | 6 (30%) |
| ovarian cancer | 6 (30%) |
| Genomic alterations, n (%) | |
| TP53 | 7 (35%) |
| PTEN | 4 (20%) |
| PIK3CA | 4 (20%) |
| Actionable alteration, n (%) | 19 (95%) |
| Druggable alteration, n (%) | 19 (95%) |
| Prior chemotherapy (n) | |
| Median (range) | 2 (0–4) |
| Genotype matched therapy | |
| Matched therapy, n (%) | 7 (35%) |
| Response rate, n (%) | 3/7 (43%) |
| No | Age | Stage | Tumor Type | Histological Type | Targets | Targeted Therapy | Best Response |
|---|---|---|---|---|---|---|---|
| 1 | 62 | IIB | CC | SCC | Hypermutated and MSI-high MLH1 (Loss) | pembrolizumab | PD |
| 2 | 65 | IB | EC | EM(G3) | PTEN (mut) | everolimus | SD |
| 3 | 68 | IVB | EC | EM(G3) | TSC2 (somatic UPD) | everolimus letrozole | PR |
| 4 | 59 | IVB | EC | EM(G3) | AKT1, MTOR, CTNNB1(mut) | everolimus letrozole | PD |
| 5 | 59 | IVB | EC | EM(G3) | Hypermutated and MSI-high | pembrolizumab | - |
| 6 | 70 | IVB | EC | HGSC | HRD, BRIP1(mut) | olaparib | CR |
| 7 | 41 | IVB | OC | HGSC | NF1 (Loss) | Everolimus letrozole | PD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawada, K.; Nakayama, K.; Nakamura, K.; Yoshimura, Y.; Razia, S.; Ishikawa, M.; Yamashita, H.; Ishibashi, T.; Sato, S.; Kyo, S. Clinical Outcomes of Genotype-Matched Therapy for Recurrent Gynecological Cancers: A Single Institutional Experience. Healthcare 2021, 9, 1395. https://doi.org/10.3390/healthcare9101395
Sawada K, Nakayama K, Nakamura K, Yoshimura Y, Razia S, Ishikawa M, Yamashita H, Ishibashi T, Sato S, Kyo S. Clinical Outcomes of Genotype-Matched Therapy for Recurrent Gynecological Cancers: A Single Institutional Experience. Healthcare. 2021; 9(10):1395. https://doi.org/10.3390/healthcare9101395
Chicago/Turabian StyleSawada, Kiyoka, Kentaro Nakayama, Kohei Nakamura, Yuki Yoshimura, Sultana Razia, Masako Ishikawa, Hitomi Yamashita, Tomoka Ishibashi, Seiya Sato, and Satoru Kyo. 2021. "Clinical Outcomes of Genotype-Matched Therapy for Recurrent Gynecological Cancers: A Single Institutional Experience" Healthcare 9, no. 10: 1395. https://doi.org/10.3390/healthcare9101395