
The Provision and Utilization of Traditional Korean Medicine in South Korea: Implications on Integration of Traditional Medicine in a Developed Country


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Human Resources and Facilities in TKM
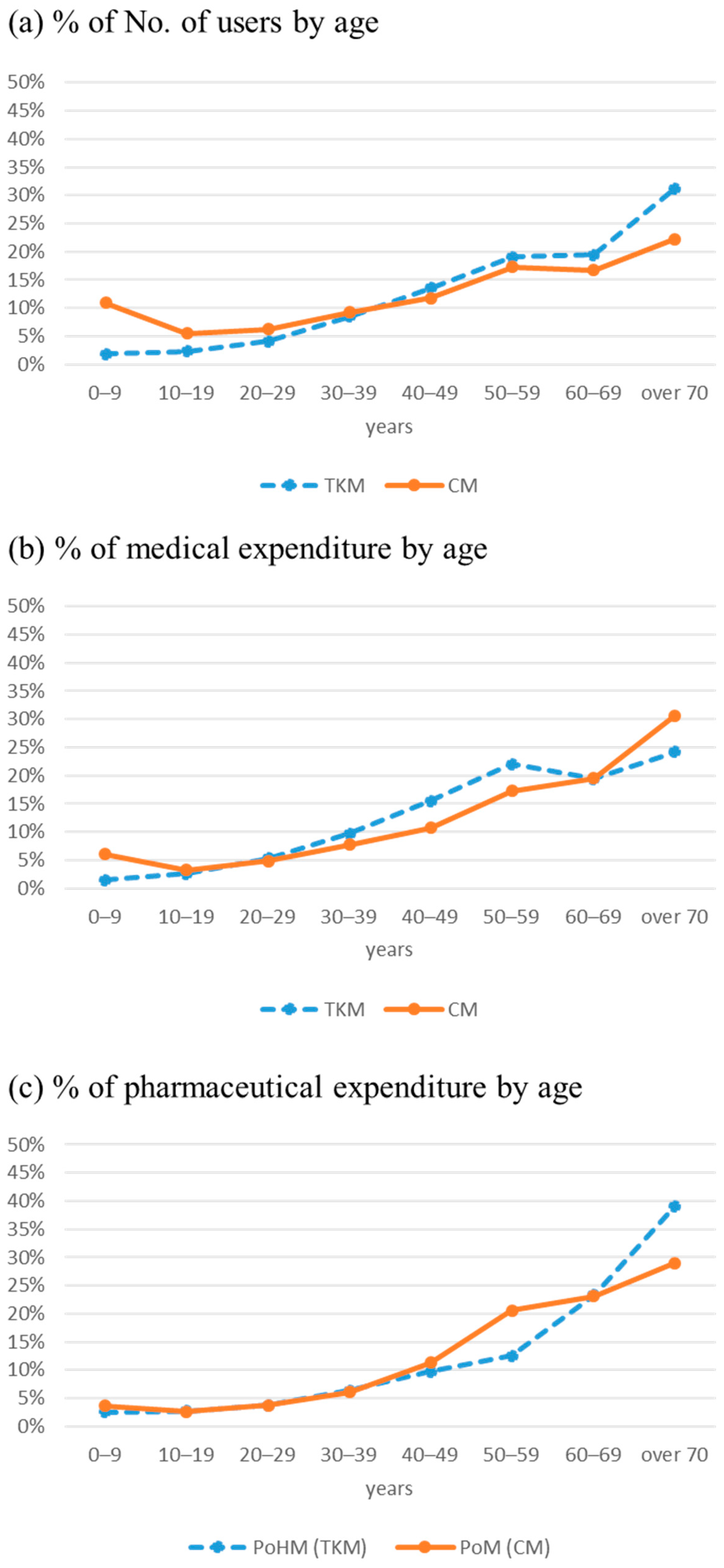
3.2. Medical and Pharmaceutical Expenditure in TKM
3.3. Utilization of TKM by the Type of Diseases 29
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Regional Office for the Western Pacific. In-House Consultation on the 2016–2017 Agenda for Traditional Medicine Integration in the Western Pacific Region. Published June 2016. Available online: https://iris.wpro.who.int/bitstream/handle/10665.1/13407/RS-2015-GE-68-PHL-eng.pdf (accessed on 10 December 2019).
- World Health Organization Regional Office for the Western Pacific. Meeting on the Contribution of Traditional Medicine in Strengthening Primary Health Care. Published December 2017. Available online: https://iris.wpro.who.int/bitstream/handle/10665.1/13969/RS-2017-GE-58-PHL-eng.pdf (accessed on 10 December 2019).
- World Health Organization Regional Office for the Western Pacific. Meeting on Strengthening Quality Assurance of Traditional Medicines. Published July 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/259121/RS-2017-GE-06-KOR-eng.pdf (accessed on 10 December 2019).
- World Health Organization Regional Office for the Western Pacific. Technical Consultation on Medium–Term Agenda on Traditional Medicine for Universal Health Coverage in the Western Pacific Region. Published June 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/275590/RS-2018-GE-35-PHL-eng.pdf?sequence=1&isAllowed=y (accessed on 15 January 2020).
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine. 2019. Available online: https://www.who.int/traditional-complementary-integrative-medicine/WhoGlobalReportOnTraditionalAndComplementaryMedicine2019.pdf (accessed on 8 October 2019).
- World Health Organization Regional Office for the Western Pacific. The Regional Strategy for Traditional Medicine in the Western Pacific (2011–2020). 2012. Available online: https://www.who.int/publications/i/item/9789290615590 (accessed on 5 October 2019).
- Lim, B. Korean medicine coverage in the National Health Insurance in Korea: Present situation and critical issues. Integr. Med. Res. 2013, 2, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J. Research Network in Traditional Korean Medicine; Korea Institute of Oriental Medicine: Daejeon, Korea, 2019. [Google Scholar]
- Park, J.E.; Kim, Y.J.; Suh, H.S. Patterns and Factors Associated with the Utilization of Oriental and Western Medical Care in Musculoskeletal Disease Outpatients. J. Health Tech. Assess 2021, 9, 41–48. [Google Scholar]
- OECD/WHO. Health at a Glance: Asia/Pacific 2020: Measuring Progress Towards Universal Health Coverage; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Korea Institute of Oriental Medicine, National Institute for Korean Medicine Development, School of Korean Medicine Pusan National University, Association of Korean Medicine. 2017 Yearbook of Traditional Korean Medicine. 2019. Available online: https://www.kiom.re.kr/brdartcl/boardarticleView.do?menu_nix=WUNNW2Aq&brd_id=BDIDX_o9YEVvNb40b134N1Rt17aq&cont_idx=9 (accessed on 18 October 2020).
- National Health Insurance Service, Health Insurance Review & Assessment Service. 2017 National Health Insurance Statistical Yearbook. 2018. Available online: http://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020045020000 (accessed on 18 October 2020).
- Korean Ministry of Health and Welfare. 2017 Annual Statistics on Health and Welfare. 2018. Available online: http://www.mohw.go.kr/react/jb/sjb030301ls.jsp?PAR_MENU_ID=03&MENU_ID=032901&SEARCHKEY=TITLE&SEARCHVALUE=%EB%B3%B4%EA%B1%B4%EB%B3%B5%EC%A7%80%ED%86%B5%EA%B3%84%EC%97%B0%EB%B3%B4&page=1 (accessed on 18 October 2020).
- Health Insurance Review & Assessment Service. 2017 Annual Statistics on Medical Expenses. 2018. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020045030000&brdScnBltNo=4&brdBltNo=2387&pageIndex=3 (accessed on 18 October 2020).
- Health Insurance Review & Assessment Service. 2017 Status of Claims for Prescribed Medicines. 2019. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020045010000&brdScnBltNo=4&brdBltNo=2348&pageIndex=1 (accessed on 18 October 2020).
- Shin, J.W.; Lee, S.Y.; Shin, H.Y.; Yoon, K.J.; Lee, S.H.; Shon, C.G.; Hwang, S.K.; Kim, S.W.; Park, G.; Shin, J.Y.; et al. 2016 Survey on Patients. Korea Institute for Health and Social Affairs. Published 2017. Available online: http://www.prism.go.kr/homepage/researchCommon/downloadResearchAttachFile.do?work_key=001&file_type=CPR&seq_no=001&pdf_conv_yn=Y&research_id=1351000-201600192 (accessed on 5 September 2020).
- Korean Ministry of Health and Welfare. Lists of Herbal Medicines Covered by National Health Insurance (2019-172). Published July 2019. Available online: http://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100&brdScnBltNo=4&brdBltNo=7446&pageIndex=1#none (accessed on 11 November 2020).
- Health-Care Expenditure on Arthritis and Other Musculoskeletal Conditions 2008–09. Arthritis Series no. 20. Cat. no. PHE 177. Australian Institute of Health and Welfare. Published August 2014. Available online: https://www.aihw.gov.au/getmedia/fef9cada-9674-4273-8191-5d7793a4360d/17760a.pdf.aspx?inline=true (accessed on 11 November 2020).
- Corp, N.; Jordan, J.L.; Croft, P.R. Justifications for using complementary and alternative medicine reported by persons with musculoskeletal conditions: A narrative literature synthesis. PLoS ONE 2018, 13, e0200879. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Li, K. The Association Between Musculoskeletal Symptoms and Traditional Chinese Medicine Use Among Chinese Older Adults in the Greater Chicago Area. Gerontol. Geriatr. Med. 2018, 4, 2333721418778179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavadar, G.; Eroglu Demir, S.; Aytekin, E.; Akbal, Y. Use of traditional and complementary medicine for musculoskeletal diseases. Turk J. Med. Sci. 2019, 49, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Korean Ministry of Health and Welfare, National Development Institute of Korean Medicine. 2020 Survey Report on Utilization of Traditional Korean Medicine. Published June 2021. Available online: https://www.koms.or.kr/board/researchReport/view.do?post_no=161&menu_no=21 (accessed on 30 September 2021).
- Tavares, A.I. Substitutes or complements? Diagnosis and treatment with non-conventional and conventional medicine. Int. J. Health Policy Manag. 2015, 4, 235–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grand View Research. Dietary Supplements Market Size, Share & Trends Analysis Report by Ingredient (Vitamins, Minerals), By Form, By Application, By End User, By Distribution Channel, By Region, and Segment Forecasts, 2020–2027. 2020. [Google Scholar]
- Grand View Research. Massage Equipment Market Size, Share & Trends Analysis Report By Product (Chairs & Sofas, Handheld), By Application (Commercial, Home), By Region, And Segment Forecasts, 2019–2025. 2019. [Google Scholar]
- Korean Ministry of Education, Korean Educational Development Institute. 2019 Statistical Yearbook of Education. 2020. Available online: https://kess.kedi.re.kr/publ/view?survSeq=2020&publSeq=2&menuSeq=3895&itemCode=02&language=en# (accessed on 1 October 2021).
- Korean Ministry of Health and Welfare, National Medical Center. 2019 Statistics of Public health care. Available online: https://www.nmc.or.kr/nmc/singl/convert/convertToHtml.do?viewType=CONTBODY&atchFileId=852b10a3702545de89cfcdc82bc74db1&fileSn=1 (accessed on 30 September 2021).
- Korea Health Promotion Institute. Introduction to Integrated Community Health Promotion Program in Traditional Korean Medicine; Korea Health Promotion Institute: Seoul, Korea, 2020.
- Korean Ministry of Health and Welfare; National Development Institute of Korean Medicine. Research on Health and Welfare Service Model and System Development in Traditional Korean Medicine Regarding Local Community. 2019. [Google Scholar]
- Korean Ministry of Health and Welfare. Health Insurance Review & Assessment Service. Guidelines for Pilot Projects on Home Visit Traditional Korean Medicine Service. 2021. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100&brdScnBltNo=4&brdBltNo=8978&pageIndex=1#none (accessed on 28 September 2021).
- National Clearinghouse for Korean Medicine. Database of Clinical Practice Guidelines of Traditional Korean Medicine. Available online: http://www.nckm.or.kr/main/module/practiceGuide/index.do?menu_idx=14 (accessed on 1 November 2020).
- Kim, D.; Lim, B.; Han, D.; Park, J.; Jung, H. Survey on practice behavior and model acceptance of traditional Korean medicine(TKM) doctors in order to develop health insurance payment model related with TKM clinical practice guidelines(CPGs). J. Soc. Prev. Korean Med. 2017, 21, 1–10. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. 2019 National Healthcare Quality and Disparities Report. Agency for Healthcare Research and Quality: Rockville, MD, USA, 2021. Available online: https://www.ahrq.gov/research/findings/nhqrdr/nhqdr19/index.html (accessed on 1 March 2021).


{kind=link}
| TKM Personnel | TKM Facilities | |||||
|---|---|---|---|---|---|---|
| TKM Doctors | Doctors Who Have Both Licenses (a) | HM Pharmacists (b) | TKM Hospitals | TKM Clinics | HM Pharmacies | |
| YR 2008 (n (%)) (c) | 14,818 (13.4) | 189 (1.3) | 1222 (3.7) | 146 (5.8) | 11,334 (22.0) | 510 (2.4) |
| YR 2017 (n (%)) (c) | 24,627 (16.4) | 316 (1.3) | 2404 (6.1) | 312 (8.7) | 14,155 (22.6) | 595 (2.7) |
| Annual average growth rate(%) (d) (2008–2017) | 5.8 | 5.9 | 7.8 | 8.8 | 2.5 | 1.7 |
| NHI | Medical Aid | Workers’ Compensation | Automobile Insurance | ||
|---|---|---|---|---|---|
| Total | |||||
| Nursing Hospitals (a) | |||||
| Medical expenditure in TKM (USD, Million) (2017) | 2237 | 96.2 | 146.5 | 3.1 | 495.7 |
| % of TKM expenditure among total medical expenditure in each type of insurance (2017) | 3.6 | 2.1 | 2.3 | 0.6 | 31.8 |
| Annual average growth rate of TKM medical expenditure (%) (b) (2008–2017) | 7.2 | 18.8 (2010–2017) | 8.2 | 8.4 | 27.8 (2014–2017) |
| Annual average growth rate of CM medical expenditure (%) (b) (2008–2017) | 8.0 | 17.6 (2010–2017) | 5.3 | −0.5 | 1.5 (2014–2017) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Yi, E.; Yi, J. The Provision and Utilization of Traditional Korean Medicine in South Korea: Implications on Integration of Traditional Medicine in a Developed Country. Healthcare 2021, 9, 1379. https://doi.org/10.3390/healthcare9101379
Park J, Yi E, Yi J. The Provision and Utilization of Traditional Korean Medicine in South Korea: Implications on Integration of Traditional Medicine in a Developed Country. Healthcare. 2021; 9(10):1379. https://doi.org/10.3390/healthcare9101379
Chicago/Turabian StylePark, Jieun, Eunhee Yi, and Junhyeok Yi. 2021. "The Provision and Utilization of Traditional Korean Medicine in South Korea: Implications on Integration of Traditional Medicine in a Developed Country" Healthcare 9, no. 10: 1379. https://doi.org/10.3390/healthcare9101379