
Immediate Effects of Sforzesco® Bracing on Respiratory Function in Adolescents with Idiopathic Scoliosis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
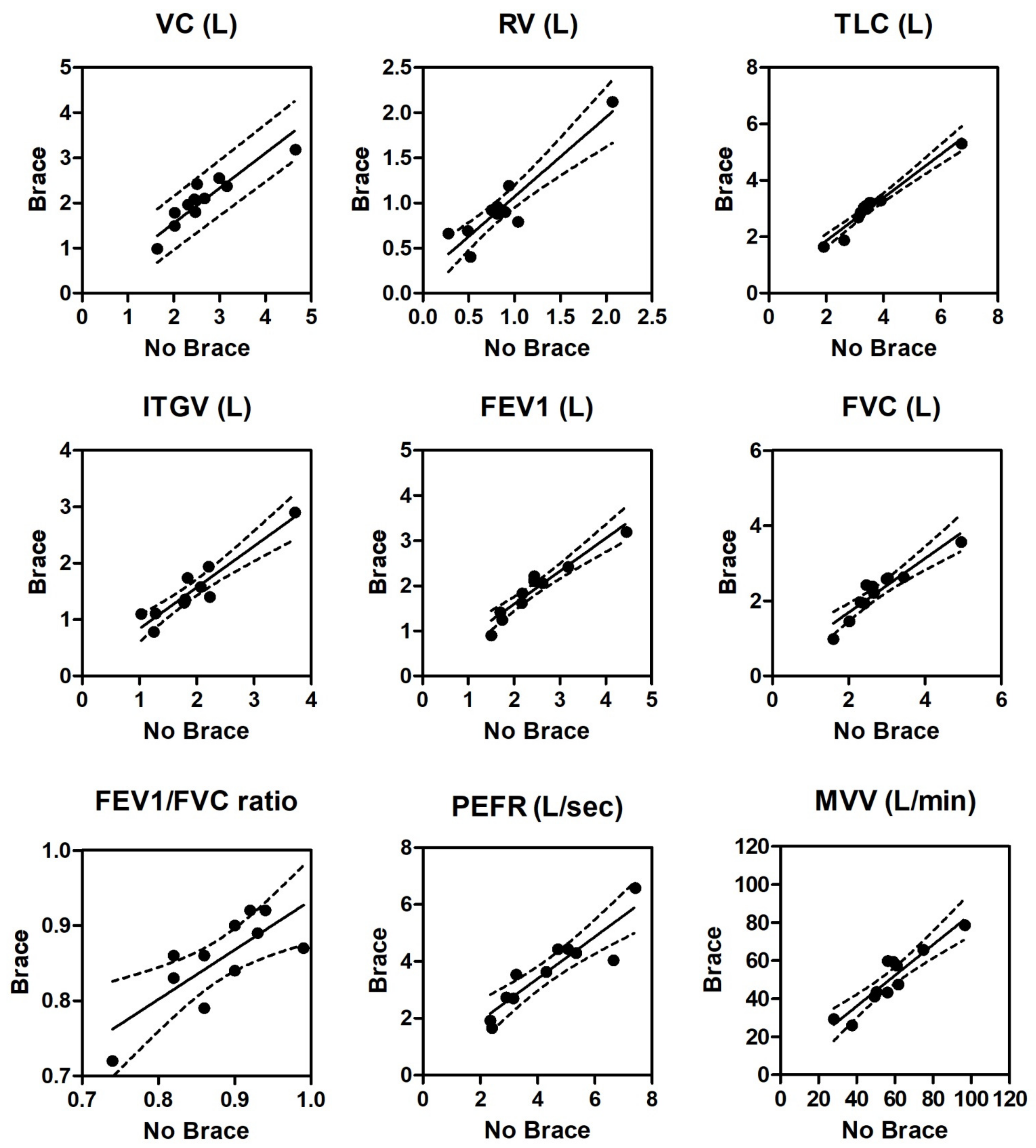
| y-Intercept (a) | Slope (b) | Slope 95% CI | Coeff. r | R2 | p Value | Deviation from 0 | Regression Equation = a + (b·x) | |
|---|---|---|---|---|---|---|---|---|
| VC | 0.3365 | 0.6577 | 0.430 to 0.885 | 0.909 | 0.826 | <0.0001 | Significant | = 0.3365 + (0.6577 x) |
| RV | 0.1875 | 0.8824 | 0.611 to 1.154 | 0.926 | 0.857 | <0.0001 | Significant | = 0.1875 + (0.8824 x) |
| TLC | 0.3214 | 0.7659 | 0.638 to 0.893 | 0.977 | 0.954 | <0.0001 | Significant | = 0.3214 + (0.7659 x) |
| TGV | 0.1072 | 0.7311 | 0.522 to 0.940 | 0.935 | 0.874 | <0.0001 | Significant | = 0.1072 + (0.7311 x) |
| FEV1 | 0.1414 | 0.7280 | 0.552 to 0.904 | 0.952 | 0.907 | <0.0001 | Significant | = 0.1414 + (0.7280 x) |
| FVC | 0.2543 | 0.7181 | 0.508 to 0.928 | 0.932 | 0.869 | <0.0001 | Significant | = 0.2543 + (0.7181 x) |
| ratio | 0.2740 | 0.6598 | 0.249 to 1.070 | 0.771 | 0.595 | =0.0054 | Significant | = 0.2740 + (0.6598 x) |
| PEFR | 0.4394 | 0.7378 | 0.479 to 0.996 | 0.907 | 0.822 | <0.0001 | Significant | = 0.4394 + (0.7378 x) |
| MVV | 3.813 | 0.8072 | 0.557 to 1.058 | 0.924 | 0.855 | <0.0001 | Significant | = 3.8130 + (0.8072 x) |
References
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Koumbourlis, A.C. Scoliosis and the respiratory system. Paediatr. Respir. Rev. 2006, 7, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.; Wright, J.G.; Dobbs, M.B. Effect of bracing adolescent idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, D.E.; Hong, H.H.; Webb, K.A. Respiratory sensation during chest wall restriction and dead space loading in exercising men. J. Appl. Physiol. 2000, 88, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.D.; Robertson, C.F.; Olinsky, A.; Dickens, D.R.V.; Phelan, P.D. Pulmonary restrictive effect of bracing in mild idiopathic scoliosis. Thorax 1987, 42, 959–961. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.D.; Robertson, C.F.; Hudson, I.; Phelan, P.D. Effect of bracing on respiratory mechanics in mild idiopathic scoliosis. Thorax 1989, 44, 548–553. [Google Scholar] [CrossRef] [Green Version]
- Katsaris, G.; Loukos, A.; Valavanis, J.; Vassiliou, M.; Behrakis, P.K. The immediate effect of a Boston brace on lung volumes and pulmonary compliance in mild adolescent idiopathic scoliosis. Eur. Spine J. 1999, 8, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Yagci, G.; Demirkiran, G.; Yakut, Y. In-brace alterations of pulmonary functions in adolescents wearing a brace for idiopathic scoliosis. Prosthet. Orthot. Int. 2019, 43, 434–439. [Google Scholar] [CrossRef]
- Negrini, S.; Marchini, G. Efficacy of the symmetric, patient-oriented, rigid, three-dimensional, active (SPoRT) concept of bracing for scoliosis: A prospective study of the Sforzesco versus Lyon brace. Eur. Medicophys. 2007, 43, 171–181; discussion 183–184. [Google Scholar]
- Negrini, S.; Atanasio, S.; Negrini, F.; Zaina, F.; Marchini, G. The Sforzesco brace can replace cast in the correction of adolescent idiopathic scoliosis: A controlled prospective cohort study. Scoliosis 2008, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3–48. [Google Scholar] [CrossRef] [Green Version]
- Quanjer, P.H.; Capderou, A.; Mazicioglu, M.M.; Aggarwal, A.N.; Banik, S.D.; Popovic, S.; Tayie, F.A.K.; Golshan, M.; Ip, M.S.M.; Zelter, M. All-age relationship between arm span and height in different ethnic groups. Eur. Respir. J. Engl. 2014, 44, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Hibbert, M.E.; Lanigan, A.; Raven, J.; Phelan, P.D. Relation of armspan to height and the prediction of lung function. Thorax 1988, 43, 657–659. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M.; Lobstein, T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Int. J. Pediatr. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Brack, T.; Jubran, A.; Tobin, M.J. Dyspnea and decreased variability of breathing in patients with restrictive lung disease. Am. J. Respir. Crit. Care Med. 2002, 165, 1260–1264. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Barois, A. Respiratory problems in severe scoliosis. Bull. Acad. Natl. Med. 1999, 183, 721–730. [Google Scholar]
- Kearon, C.; Viviani, G.R.; Kirkley, A. Fadors Determining Pulmonary Function in Adolescent Idiopathic Thoracic Scoliosis. Am. Rev. Respir. Dis 1993, 148, 288–294. [Google Scholar] [CrossRef]
- Nachemson, A.L.; Peterson, L.E. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J. Bone Jt. Surg. 1995, 77, 815–822. [Google Scholar] [CrossRef]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2067–2068. [Google Scholar] [CrossRef]
- Sahebjami, H. Dyspnea in obese healthy men. Chest 1998, 114, 1373. [Google Scholar] [CrossRef]


| Patient Initials | Age (yrs) | Gender | Height (cm) | Weight (kg) | BMI-for-Age z-Score | Time of Treatment (Month) | Cobb Angle (Grade) | Risser Score | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M.A.P. | 12 | F | 129 | 28.3 | 0.19 | 18 | 30 | 0 |
| 2 | D.A. | 15 | F | 145 | 49.1 | 1.07 | 8 | 22 | 3 |
| 3 | C.S. | 11 | F | 158 | 45.0 | 0.47 | 12 | 23 | 0 |
| 4 | G.S.M. | 13 | F | 151 | 47.4 | 0.70 | 19 | 34 | 3 |
| 5 | C.M.G. | 14 | F | 152 | 46.3 | 0.03 | 10 | 24 | 3 |
| 6 | P.A. | 12 | F | 121 | 22.3 | −0.21 | 1 | 22 | 0 |
| 7 | L.M. | 15 | M | 178 | 53.6 | −1.54 | 1 | 22 | 3 |
| 8 | L.R. | 16 | F | 162 | 47.2 | −1.21 | 24 | 30 | 4 |
| 9 | C.B. | 13 | F | 157 | 43.0 | −0.72 | 2 | 28 | 0 |
| 10 | L.A. | 12 | F | 140 | 43.5 | 2.29 | 15 | 30 | 0 |
| 11 | C.M. | 13 | F | 146 | 35.1 | −1.12 | 1 | 21 | 0 |
| Mean | 13.27 | 149 | 41.9 | −0.0045 | 10.09 | 26 | 1.45 | ||
| ±SD | 1.56 | 15.68 | 9.46 | 1.13 | 8.25 | 4.49 | 1.69 | ||
| Min | 11 | 121 | 22.3 | −1.54 | 1 | 21 | 0 | ||
| Max | 16 | 178 | 53.6 | 2.29 | 24 | 34 | 4 |
| VC (L) | RV (L) | TLC (L) | ITGV (L) | FEV1 (L) | FVC (L) | FEV1/FVC Ratio | MVV L/min | PEFR L/sec | |
|---|---|---|---|---|---|---|---|---|---|
| Predicted | 2.79 (0.26) | 0.95 (0.08) | 3.70 (0.31) | 1.84 (0.17) | 2.52 (0.23) | 2.85 (0.92) | 0.88 (0.00) | 50.12 (4.74) | 5.12 (0.39) |
| No Brace | 2.63 (0.24) | 0.86 (0.14) | 3.52 (0.36) | 1.91 (0.22) | 2.44 (0.25) | 2.77 (0.88) | 0.88 (0.02) | 57.38 (5.44) | 4.32 (0.51) |
| Brace | 2.06 (0.17) | 0.95 (0.13) | 3.02 (0.28) | 1.50 (0.17) | 1.92 (0.19) | 2.25 (0.68) | 0.85 (0.02) | 50.13 (4.75) | 3.63 (0.42) |
| 1-way ANOVA | p < 0.0001 | NS | p < 0.0001 | p < 0.0001 | p < 0.0001 | p < 0.0001 | NS | NS | p < 0.0001 |
| F-value | 29.21 | 1.21 | 18.50 | 14.75 | 22.04 | 34.56 | 1.05 | 2.29 | 15.03 |
| Pred vs. No Brace * | NS | NS | NS | NS | NS | p < 0.05 | NS | NS | p < 0.05 |
| Pred vs. Brace * | p < 0.05 | NS | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.05 | NS | NS | p < 0.05 |
| No Brace vs. Brace * | p < 0.05 | NS | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.05 | NS | NS | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Maria, F.; Vescio, A.; Caldaci, A.; Vancheri, A.; Di Maria, C.; Sapienza, M.; Testa, G.; Pavone, V. Immediate Effects of Sforzesco® Bracing on Respiratory Function in Adolescents with Idiopathic Scoliosis. Healthcare 2021, 9, 1372. https://doi.org/10.3390/healthcare9101372
Di Maria F, Vescio A, Caldaci A, Vancheri A, Di Maria C, Sapienza M, Testa G, Pavone V. Immediate Effects of Sforzesco® Bracing on Respiratory Function in Adolescents with Idiopathic Scoliosis. Healthcare. 2021; 9(10):1372. https://doi.org/10.3390/healthcare9101372
Chicago/Turabian StyleDi Maria, Fabrizio, Andrea Vescio, Alessia Caldaci, Ada Vancheri, Chiara Di Maria, Marco Sapienza, Gianluca Testa, and Vito Pavone. 2021. "Immediate Effects of Sforzesco® Bracing on Respiratory Function in Adolescents with Idiopathic Scoliosis" Healthcare 9, no. 10: 1372. https://doi.org/10.3390/healthcare9101372