
A Protocol for a Systematic Review and Meta-Analysis of Mind–Body Modalities to Manage the Mental Health of Healthcare Workers during the COVID-19 Era


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality and Risk of Bias Assessment
2.6. Data Analysis and Synthesis
2.7. Reporting Bias
2.8. Patient and Public Involvement Statement
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javed, B.; Sarwer, A.; Soto, E.B.; Mashwani, Z.-U.-R. The coronavirus (COVID-19) pandemic’s impact on mental health. Int. J. Health Plan. Manag. 2020, 35, 993–996. [Google Scholar] [CrossRef]
- Braquehais, M.D.; Vargas-Cáceres, S.; Gómez-Durán, E.; Nieva, G.; Valero, S.; Casas, M.; Bruguera, E. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QJM 2020, 207, 613–617. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef]
- da Silva, F.C.T.; Neto, M.L.R. Psychological effects caused by the COVID-19 pandemic in health professionals: A systematic review with meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110062. [Google Scholar] [CrossRef]
- Ehrlich, H.; McKenney, M.; Elkbuli, A. Protecting our healthcare workers during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 1527–1528. [Google Scholar] [CrossRef] [PubMed]
- Wolsko, P.M.; Eisenberg, D.M.; Davis, R.B.; Phillips, R.S. Use of mind-body medical therapies. J. Gen. Intern. Med. 2004, 19, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocchiara, R.A.; Peruzzo, M.; Mannocci, A.; Ottolenghi, L.; Villari, P.; Polimeni, A.; Guerra, F.; La Torre, G. The Use of Yoga to Manage Stress and Burnout in Healthcare Workers: A Systematic Review. J. Clin. Med. 2019, 8, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriakous, S.A.; Elliott, K.A.; Lamers, C.; Owen, R. The Effectiveness of Mindfulness-Based Stress Reduction on the Psychological Functioning of Healthcare Professionals: A Systematic Review. Mindfulness 2020, 12, 1–28. [Google Scholar] [CrossRef]
- Dharmawardene, M.; Givens, J.; Wachholtz, A.; Makowski, S.; Tjia, J. A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support. Palliat. Care 2016, 6, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Cocchiara, R.A.; Dorelli, B.; Gholamalishahi, S.; Longo, W.; Musumeci, E.; Mannocci, A.; La Torre, G. Tai Chi and Workplace Wellness for Health Care Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 343. [Google Scholar] [CrossRef] [Green Version]
- Maric, V.; Mishra, J.; Ramanathan, D.S. Using Mind-Body Medicine to Reduce the Long-Term Health Impacts of COVID-Specific Chronic Stress. Front. Psychiatry 2021, 12, 585952. [Google Scholar] [CrossRef] [PubMed]
- Behan, C. The benefits of meditation and mindfulness practices during times of crisis such as COVID-19. Ir. J. Psychol. Med. 2020, 37, 256–258. [Google Scholar] [CrossRef]
- Kwon, C.-Y.; Kwak, H.-Y.; Kim, J.W. Using Mind-Body Modalities via Telemedicine during the COVID-19 Crisis: Cases in the Republic of Korea. Int. J. Environ. Res. Public Health 2020, 17, 4477. [Google Scholar] [CrossRef]
- Hall, D.L.; Millstein, R.A.; Luberto, C.M.; Perez, G.K.; Park, E.R. Responding to COVID-19 Stress: Disseminating Mind-Body Resiliency Approaches. Glob. Adv. Health Med. 2020, 9, 2164956120976554. [Google Scholar] [CrossRef]
- Rodriguez-Vega, B.; Palao, Á.; Muñoz-Sanjose, A.; Torrijos, M.; Aguirre, P.; Fernández, A.; Amador, B.; Rocamora, C.; Blanco, L.; Marti-Esquitino, J.; et al. Implementation of a Mindfulness-Based Crisis Intervention for Frontline Healthcare Workers During the COVID-19 Outbreak in a Public General Hospital in Madrid, Spain. Front. Psychiatry 2020, 11, 562578. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, S.; Tennison, J.; Cohen, L.; Urso, C.; Subramaniam, B.; Bruera, E. Yoga-Based Breathing Techniques for Health Care Workers During COVID-19 Pandemic: Interests, Feasibility, and Acceptance. J. Altern. Complementary Med. 2021, 706–709. [Google Scholar] [CrossRef]
- Trevino, K.M.; Raghunathan, N.; Latte-Naor, S.; Polubriaginof, F.C.G.; Jensen, C.; Atkinson, T.M.; Emard, N.; Seluzicki, C.M.; Ostroff, J.S.; Mao, J.J. Rapid deployment of virtual mind-body interventions during the COVID-19 outbreak: Feasibility, acceptability, and implications for future care. Support. Care Cancer 2021, 29, 543–546. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Programme, C.A.S. CASP (Randomised Controlled Trial) Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 1 October 2021).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboke, NJ, USA, 2019. [Google Scholar]
- Health, N.I.O. Study Quality Assessment Tools. US Department of Health & Human Services. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 July 2021).
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vera San Juan, N.; Aceituno, D.; Djellouli, N.; Sumray, K.; Regenold, N.; Syversen, A.; Mulcahy Symmons, S.; Dowrick, A.; Mitchinson, L.; Singleton, G.; et al. Mental health and well-being of healthcare workers during the COVID-19 pandemic in the UK: Contrasting guidelines with experiences in practice. BJPsych Open 2020, 7, e15. [Google Scholar] [CrossRef]
- Portella, C.F.S.; Ghelman, R.; Abdala, C.V.M.; Schveitzer, M.C. Evidence map on the contributions of traditional, complementary and integrative medicines for health care in times of COVID-19. Integr. Med. Res. 2020, 9, 100473. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| #1. COVID-19[MH] OR SARS-CoV-2[MH] OR COVID-19[TIAB] OR SARS-CoV-2[TIAB] OR (wuhan[TIAB] AND coronavirus[TIAB]) OR 2019-nCoV[TIAB] OR 2019nCoV[TIAB] #2. Nurses[MH] OR Nursing[MH] OR nurs*[TIAB] #3. Physicians[MH] OR physician*[TIAB] OR doctor*[TIAB] #4. Health Personnel[MH] OR “health personnel*”[TIAB] OR “healthcare worker*”[TIAB] OR “hospital staff*”[TIAB] OR “health manager*”[TIAB] #5. “Mind–body Therapies”[MH] OR Meditation[MH] OR Mindfulness[MH] OR Relaxation[MH] OR “Relaxation Therapy”[MH] OR “Autogenic Training”[MH] OR Yoga[MH] OR “Tai Ji”[MH] OR Qigong[MH] OR “Breathing Exercises”[MH] OR “Music Therapy”[MH] OR “Imagery, Psychotherapy”[MH] OR “Biofeedback, Psychology”[MH] OR mind–body[TIAB] OR meditation[TIAB] OR mindful*[TIAB] OR relaxation[TIAB] OR “autogenic training”[TIAB] OR yoga[TIAB] OR “Tai Ji”[TIAB] OR “Tai Chi”[TIAB] OR Taichi[TIAB] OR qigong[TIAB] OR “qi gong”[TIAB] OR breathing[TIAB] OR music[TIAB] OR “guided imagery”[TIAB] OR biofeedback[TIAB] OR prayer[TIAB] OR faith[TIAB] #6. #1 AND (#2 OR #3 OR #4) AND #5 |
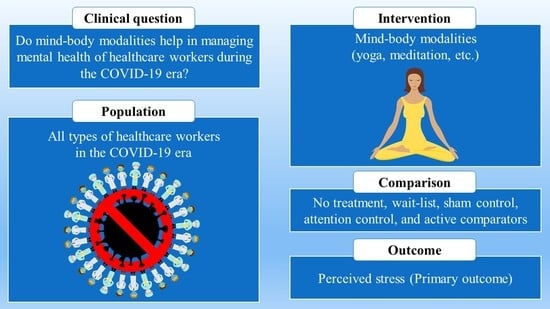
| Population | All types of HCWs, including physicians, nurses, hospital staff, and health managers |
| Intervention | Mind–body modalities, including meditation, mindfulness-based intervention, autogenic training, yoga, tai chi, qigong, breathing exercise, music therapy, guided imagery, biofeedback, prayer, and faith-based techniques |
| Comparison | No treatment, wait-list, sham control, attention control, and active comparators |
| Outcome | Primary outcome: level of perceived stressSecondary outcome: any mental health-related outcomes |
| Study type | All original clinical studies, including RCTs, CCTs, and before-after studies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.-Y.; Lee, B. A Protocol for a Systematic Review and Meta-Analysis of Mind–Body Modalities to Manage the Mental Health of Healthcare Workers during the COVID-19 Era. Healthcare 2021, 9, 1320. https://doi.org/10.3390/healthcare9101320
Kwon C-Y, Lee B. A Protocol for a Systematic Review and Meta-Analysis of Mind–Body Modalities to Manage the Mental Health of Healthcare Workers during the COVID-19 Era. Healthcare. 2021; 9(10):1320. https://doi.org/10.3390/healthcare9101320
Chicago/Turabian StyleKwon, Chan-Young, and Boram Lee. 2021. "A Protocol for a Systematic Review and Meta-Analysis of Mind–Body Modalities to Manage the Mental Health of Healthcare Workers during the COVID-19 Era" Healthcare 9, no. 10: 1320. https://doi.org/10.3390/healthcare9101320