Patient-Related Factors of Medialization Laryngoplasty with Autologous Thyroid Cartilage


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Subjects
2.2. Voice Parameters Analysis
2.3. Subjective Assessment
2.4. Statistical Analysis
3. Results
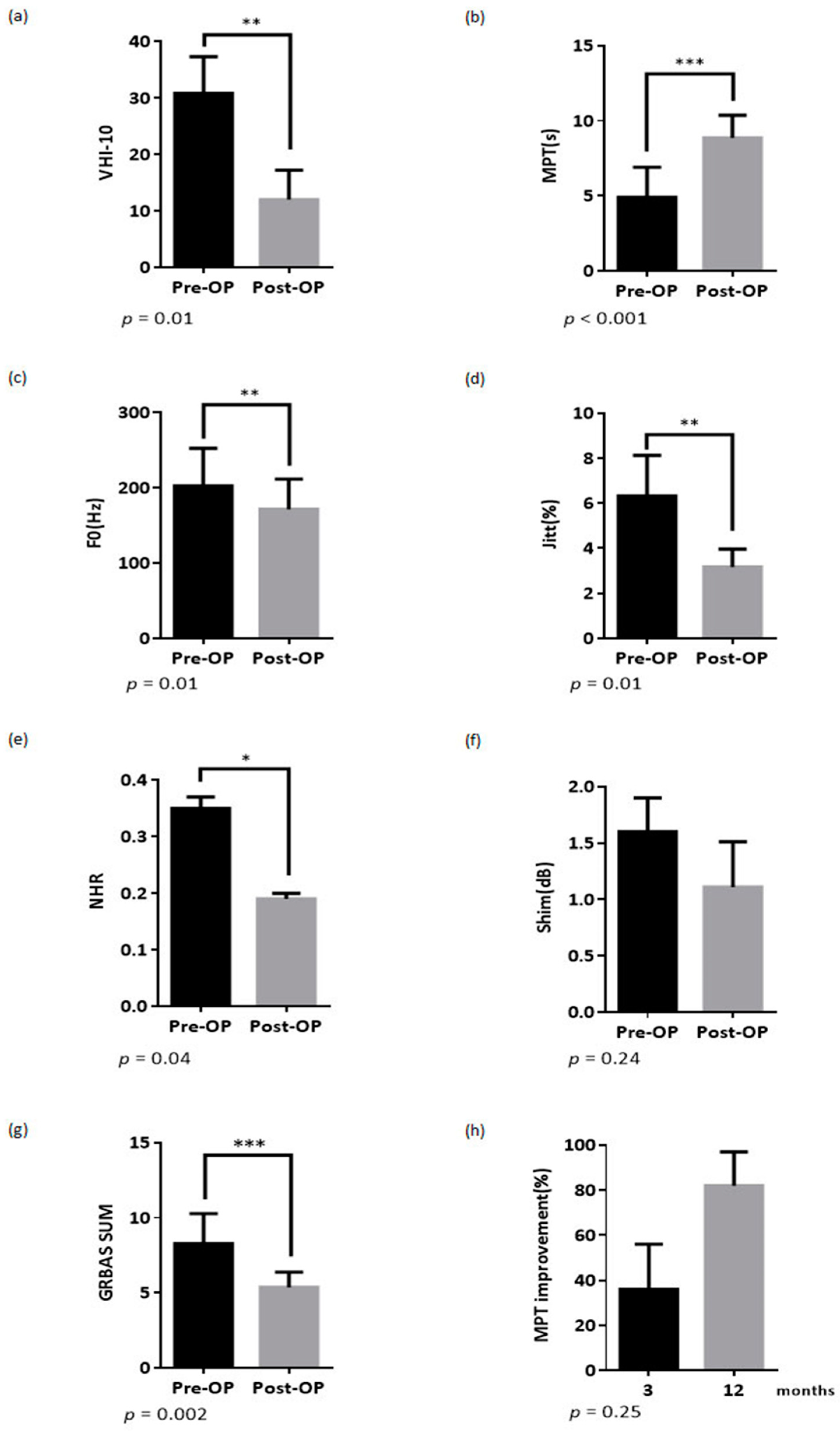
3.1. Voice Outcomes
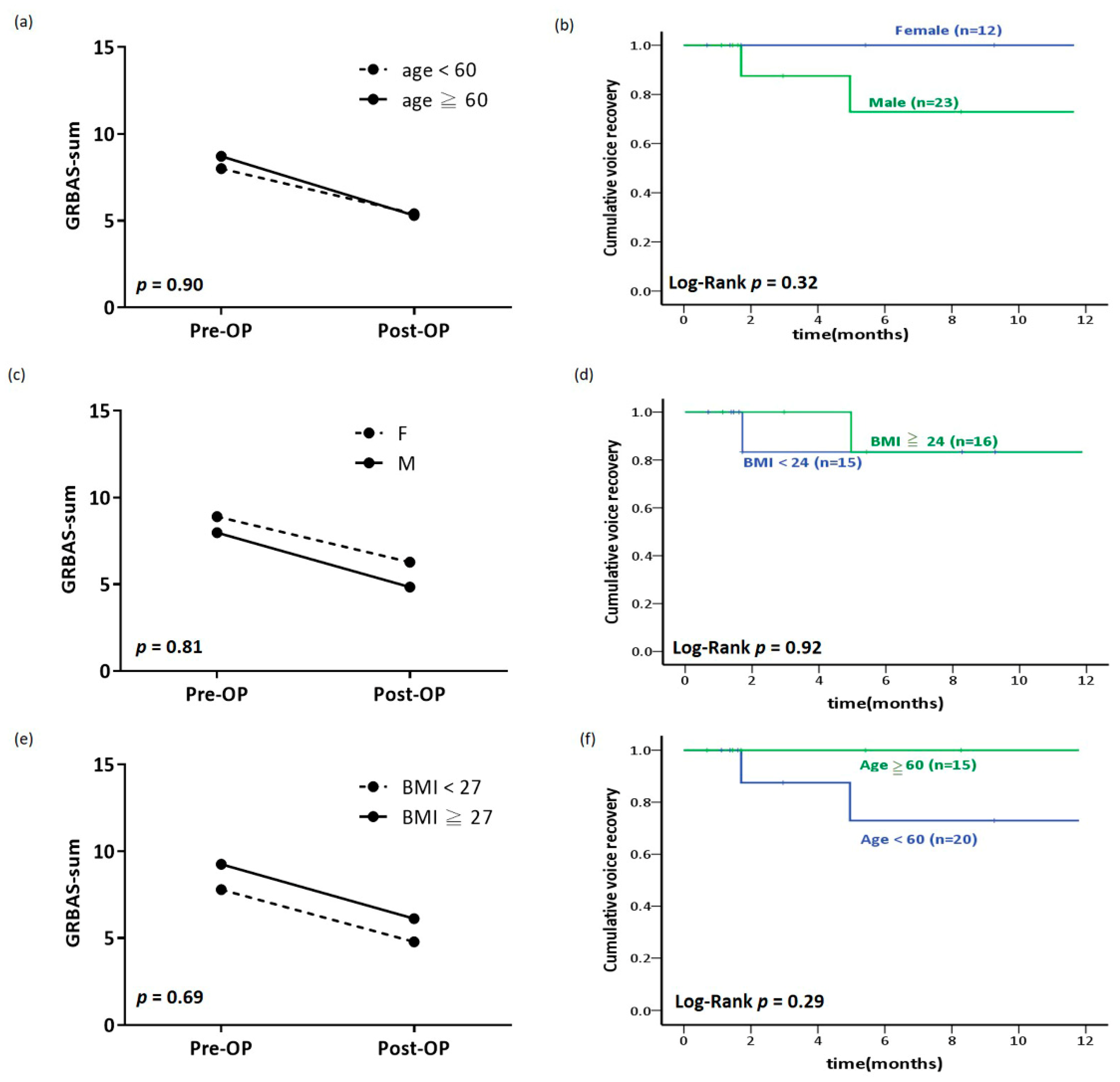
3.2. Comparison of the Outcome of MLATC between Patients’ Aged ≥ 60 and Those Aged < 60
3.3. Comparison of the Outcome of MLATC between Women and Men Patients
3.4. Comparison of the Outcome of MLATC between Patients with High and Low BMI
3.5. Repeated-Measures ANOVA for Analysis of Different Effect on Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Giraldez-Rodriguez, L.A.; Johns, M., 3rd. Glottal insufficiency with aspiration risk in dysphagia. Otolaryngol. Clin. N. Am. 2013, 46, 1113–1121. [Google Scholar] [CrossRef]
- Hsu, C.M.; Hsu, C.H.; Yang, M.Y.; Lin, H.C.; Lai, C.C.; Hsu, C.Y.; Tsou, Y.A. Glottal insufficiency with thyroid cartilage implantation: Our experience in eight patients. Clin. Otolaryngol. 2012, 37, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. Compensation Strategies in Voice Production with Glottal Insufficiency. J. Voice 2019, 33, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, K.; Hoffman, K.; D’Angelo, D.; Sulica, L. Sulcus vocalis: Results of excision without reconstruction. Laryngoscope 2019, 130, 2208–2212. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.S.; Dailey, S.H. Sulcus Vocalis. Otolaryngol. Clin. N. Am. 2019, 52, 735–743. [Google Scholar] [CrossRef]
- Tsai, M.S.; Yang, Y.H.; Liu, C.Y.; Lin, M.H.; Chang, G.H.; Tsai, Y.T.; Hsu, C.M. Unilateral Vocal Fold Paralysis and Risk of Pneumonia: A Nationwide Population-Based Cohort Study. Otolaryngol. Head Neck Surg. 2018, 158, 896–903. [Google Scholar] [CrossRef]
- Marie, J.P.; Hansen, K.; Brami, P.; Marronnier, A.; Bon-Mardion, N. Nonselective Reinnervation as a Primary or Salvage Treatment of Unilateral Vocal Fold Palsy. Laryngoscope 2019, 130, 1756–1763. [Google Scholar] [CrossRef]
- Oluwole, M.; Mills, R.P.; Davis, B.C.; Blair, R.L. The management of unilateral vocal cord palsy by augmentation using autologous fat. Clin. Otolaryngol. Allied Sci. 1996, 21, 357–359. [Google Scholar] [CrossRef]
- Ricci Maccarini, A.; Stacchini, M.; Mozzanica, F.; Schindler, A.; Basile, E.; De Rossi, G.; Woo, P.; Remacle, M.; Magnani, M. Efficacy of trans-nasal fiberendoscopic injection laryngoplasty with centrifuged autologous fat in the treatment of glottic insufficiency due to unilateral vocal fold paralysis. Acta Otorhinolaryngol. Ital. 2018, 38, 204–213. [Google Scholar]
- Sielska-Badurek, E.M.; Sobol, M.; Jedra, K.; Rzepakowska, A.; Osuch-Wojcikiewicz, E.; Niemczyk, K. Injection laryngoplasty as miniinvasive office-based surgery in patients with unilateral vocal fold paralysis—voice quality outcomes. Wideochir. Inne Tech. Maloinwazyjne 2017, 12, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Wu, L.; Gray, R.; Chhetri, D.K. Three-dimensional vocal fold structural change due to implant insertion in medialization laryngoplasty. PLoS ONE 2020, 15, e0228464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.S.; Yang, M.Y.; Chang, G.H.; Tsai, Y.T.; Lin, M.H.; Hsu, C.M. Autologous thyroid cartilage graft implantation in medialization laryngoplasty: A modified approach for treating unilateral vocal fold paralysis. Sci. Rep. 2017, 7, 4790. [Google Scholar] [CrossRef] [Green Version]
- Slavit, D.H. Phonosurgery in the elderly: A review. Ear Nose Throat J. 1999, 78, 505–509, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horii, Y. Jitter and shimmer differences among sustained vowel phonations. J. Speech Hear. Res. 1982, 25, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Klingholz, F.; Martin, F. Quantitative spectral evaluation of shimmer and jitter. J. Speech Hear. Res. 1985, 28, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Pereira Jotz, G.; Cervantes, O.; Abrahao, M.; Parente Settanni, F.A.; Carrara de Angelis, E. Noise-to-harmonics ratio as an acoustic measure of voice disorders in boys. J. Voice 2002, 16, 28–31. [Google Scholar] [CrossRef]
- Lundy, D.S.; Casiano, R.R.; Xue, J.W. Can maximum phonation time predict voice outcome after thyroplasty type I? Laryngoscope 2004, 114, 1447–1454. [Google Scholar] [CrossRef]
- Hunma, S.; Ramuth, H.; Miles-Chan, J.L.; Schutz, Y.; Montani, J.P.; Joonas, N.; Dulloo, A.G. Body composition-derived BMI cut-offs for overweight and obesity in Indians and Creoles of Mauritius: Comparison with Caucasians. Int. J. Obes. (Lond.) 2016, 40, 1906–1914. [Google Scholar] [CrossRef] [Green Version]
- Desuter, G.; Dedry, M.; Schaar, B.; van Lith-Bijl, J.; van Benthem, P.P.; Sjogren, E.V. Voice outcome indicators for unilateral vocal fold paralysis surgery: A review of the literature. Eur. Arch. Otorhinolaryngol. 2018, 275, 459–468. [Google Scholar] [CrossRef]
- Zhang, L.; Ma, W.S.; Bai, J.P.; Li, X.X.; Li, H.D.; Zhu, T.; Sun, J.Y.; Ge, H.G.; Pang, Y.; Xue, F.; et al. Comprehensive Application of Autologous Costal Cartilage Grafts in Rhino- and Mentoplasty. J. Craniofac. Surg. 2019, 30, 2174–2177. [Google Scholar] [CrossRef]
- Cui, C.; Hoon, S.Y.; Zhang, R.; Zhang, Q.; Xu, Z.; Xu, F.; Li, D.; Li, Y. Patient Satisfaction and Its Influencing Factors of Microtia Reconstruction Using Autologous Cartilage. Aesthetic Plast. Surg. 2017, 41, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Saran, M.; Georgakopoulos, B.; Bordoni, B. Anatomy, Head and Neck, Larynx Vocal Cords; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Farzal, Z.; Overton, L.J.; Farquhar, D.R.; Stephenson, E.D.; Shah, R.N.; Buckmire, R.A. Sex-based outcomes in type I thyroplasty for nonparalytic glottic incompetence. Laryngoscope 2019, 129, 2543–2548. [Google Scholar] [CrossRef] [PubMed]
- Conoyer, J.M.; Netterville, J.L.; Chen, A.; Vos, J.D. Pedicled fat flap reconstruction of the atrophic or “empty” paraglottic space following resection of teflon granuloma or oversized implant. Ann. Otol. Rhinol. Laryngol. 2006, 115, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Bowen, A.J.; Huang, T.L.; Benninger, M.S.; Bryson, P.C. Medialization Laryngoplasty in the Elderly: Outcomes and Expectations. Otolaryngol. Head Neck Surg. 2017, 157, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Chang, W.D.; Ko, L.W.; Tsou, Y.A.; Chen, S.H. Impact of patient-related factors on successful autologous fat injection laryngoplasty in thyroid surgical treated related unilateral vocal fold paralysis- observational study. Medicine (Baltimore) 2020, 99, e18579. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | Range |
|---|---|---|
| Age (years) | 58.16 ± 11.61 | 33–85 y/o |
| age ≥ 60, n (%) | 15 (43) | data |
| age < 60, n (%) | 20 (57) | |
| Sex | ||
| Men, n (%) | 23 (56) | |
| Women, n (%) | 12 (34) | |
| Total following time (months) | 37.96 ± 35.07 | 3–113.88 |
| Causes | ||
| Paralysis, n (%) | 31 (89) | |
| Atrophy, n (%) | 4 (11) | |
| Cause of paralysis | ||
| Surgical sequala, n (%) | 24 (77) | |
| Non-surgical reason, n (%) | 5 (16) | |
| Idiopathy, n (%) | 2 (6) | |
| Site of paralysis | ||
| Left, n (%) | 26 (84) | |
| Right, n (%) | 4 (13) | |
| Bilateral, n (%) | 1 (3) | |
| BMI (mean) | 24.49 ± 3.80 | 18.49–32.69 |
| BMI ≥ 24, n (%) | 16 (43) | |
| BMI < 24, n (%) | 15 (46) |
| Variables | Pre-Operation | Post-Operation | p-Value |
|---|---|---|---|
| Grade | 2.43 ± 0.77 | 1.63 ± 0.89 | 0.004 |
| Roughness | 1.74 ± 0.89 | 1.33 ± 0.80 | 0.09 |
| Breathiness | 2.34 ± 0.86 | 1.07 ± 0.94 | 0.004 |
| Asthenia | 1.28 ± 0.92 | 0.73 ± 0.94 | 0.118 |
| Strain | 0.97 ± 1.05 | 0.60 ± 0.67 | 0.11 |
| Variable | Age ≥ 60 (n = 15) | Age < 60 (n = 20) | Age ≥ 60 vs. Age < 60 | |||
|---|---|---|---|---|---|---|
| Pre-Operation | Post-Operation | Pre-Operation | Post-Operation | p-Value 1 | p-Value 2 | |
| VHI-10 | 27.25 ± 4.27 | 11.67 ± 6.35 3 | 38.00 ± 1.41 | 12.25 ± 8.52 3 | 0.062 | 0.951 |
| MPT (sec) | 3.88 ± 2.00 | 9.43 ± 4.79 3 | 5.26 ± 4.22 | 9.49 ± 5.82 3 | 0.343 | 0.978 |
| F0 (Hz) | 184.27 ± 54.83 | 159.33 ± 36.34 3 | 216.23 ± 94.97 | 178.65 ± 63.04 | 0.289 | 0.342 |
| Jitter | 6.31 ± 4.24 | 3.51 ± 2.42 | 6.32 ± 5.98 | 2.96 ± 1.77 3 | 0.996 | 0.467 |
| Shimmer | 2.45 ± 3.38 | 1.93 ± 4.04 | 0.95 ± 0.75 | 0.62 ± 0.29 | 0.088 | 0.158 |
| NHR | 0.35 ± 0.25 | 0.22 ± 0.10 | 0.35 ± 0.34 | 0.17 ± 0.06 | 0.965 | 0.093 |
| GRBAS sum | 8.71 ± 2.36 | 5.30 ± 1.83 3 | 8.00 ± 4.04 | 5.40 ± 3.93 3 | 0.587 | 0.940 |
| Grade | 2.42 ± 0.67 | 1.70 ± 0.48 | 2.44 ± 0.86 | 1.60 ± 1.05 3 | 0.925 | 0.777 |
| Roughness | 1.63 ± 0.83 | 1.30 ± 0.48 | 1.82 ± 0.95 | 1.35 ± 0.93 3 | 0.565 | 0.875 |
| Breathiness | 2.42 ± 0.79 | 1.10 ± 0.74 3 | 2.29 ± 0.92 | 1.05 ± 1.05 3 | 0.712 | 0.894 |
| Asthenia | 1.17 ± 0.94 | 0.50 ± 0.71 | 1.35 ± 0.93 | 0.85 ± 1.04 | 0.601 | 0.348 |
| Strain | 1.08 ± 1.08 | 0.70 ± 0.67 | 0.88 ± 1.05 | 0.85 ± 1.04 | 0.621 | 0.575 |
| Variable | Men (n = 23) | Women (n = 12) | Men vs. Women | |||
|---|---|---|---|---|---|---|
| Pre-Operation | Post-Operation | Pre-Operation | Post-Operation | p-Value 1 | p-Value 2 | |
| VHI-10 | 29.00 ± 4.24 | 4.28 ± 2.30 3 | 31.75 ± 7.80 | 7.00 ± 1.41 3 | 0.677 | 0.494 |
| MPT (sec) | 5.04 ± 4.23 | 10.12 ± 6.15 3 | 4.02 ± 0.88 | 7.99 ± 2.89 3 | 0.509 | 0.362 |
| F0 (Hz) | 178.90 ± 82.58 | 151.78 ± 48.28 | 242.93 ± 60.49 | 204.11 ± 50.46 3 | 0.033 | 0.007 |
| Jitter | 6.61 ± 5.76 | 2.96 ± 2.23 3 | 5.81 ± 4.32 | 3.52 ± 1.63 | 0.695 | 0.456 |
| Shimmer | 1.66 ± 2.41 | 1.43 ± 3.15 | 1.49 ± 2.41 | 0.58 ± 0.24 | 0.854 | 0.363 |
| NHR | 0.38 ± 0.33 | 0.20 ± 0.09 | 0.30 ± 0.24 | 0.18 ± 0.07 | 0.454 | 0.492 |
| GRBAS sum | 7.98 ± 3.39 | 4.84 ± 3.25 3 | 8.90 ± 3.70 | 6.27 ± 3.44 3 | 0.496 | 0.265 |
| Grade | 2.38 ± 0.86 | 1.53 ± 0.963 | 2.56 ± 0.53 | 1.82 ± 0.75 | 0.580 | 0.396 |
| Roughness | 1.58 ± 0.91 | 1.16 ± 0.83 | 2.11 ± 0.78 | 1.64 ± 0.67 | 0.137 | 0.117 |
| Breathiness | 2.30 ± 0.92 | 1.00 ± 0.94 3 | 2.44 ± 0.73 | 1.18 ± 0.98 3 | 0.682 | 0.620 |
| Asthenia | 1.25 ± 1.02 | 0.63 ± 0.90 | 1.33 ± 0.71 | 0.91 ± 1.04 | 0.826 | 0.448 |
| Strain | 0.75 ± 1.07 | 0.53 ± 0.70 | 1.44 ± 0.88 | 0.73 ± 0.65 3 | 0.101 | 0.441 |
| Variable | BMI ≥ 24 (n = 16) | BMI < 24 (n = 15) | High BMI vs. Low BMI | |||
|---|---|---|---|---|---|---|
| Pre-Operation | Post-Operation | Pre-Operation | Post-Operation | p-Value 1 | p-Value 2 | |
| VHI-10 | 32.75 ± 6.24 | 7.33 ± 1.15 3 | 28.43 ± 5.32 | 9.33 ± 4.61 3 | 0.857 | 0.703 |
| MPT (sec) | 4.58 ± 3.69 | 9.36 ± 6.74 3 | 5.20 ± 3.71 | 9.60 ± 4.73 3 | 0.686 | 0.922 |
| F0 (Hz) | 185.15 ± 61.71 | 175.00 ± 57.50 3 | 208.34 ± 93.32 | 159.26 ± 56.51 | 0.450 | 0.473 |
| Jitter | 6.54 ± 4.73 | 2.95 ± 1.50 3 | 5.57 ± 5.01 | 3.43 ± 2.59 | 0.608 | 0.564 |
| Shimmer | 0.93 ± 0.48 | 0.63 ± 0.35 | 1.83 ± 2.93 | 1.65 ± 3.63 | 0.268 | 0.325 |
| NHR | 0.35 ± 0.25 | 0.19 ± 0.09 | 0.34 ± 0.34 | 0.20 ± 0.08 | 0.949 | 0.873 |
| GRBAS sum | 9.11 ± 3.29 | 6.15 ± 3.31 3 | 7.33 ± 3.66 | 4.36 ± 3.50 3 | 0.182 | 0.184 |
| Grade | 2.50 ± 0.76 | 1.69 ± 0.75 3 | 2.36 ± 0.84 | 1.43 ± 1.02 3 | 0.641 | 0.453 |
| Roughness | 1.68 ± 1.10 | 1.46 ± 0.88 | 1.85 ± 0.69 | 1.14 ± 0.77 3 | 0.643 | 0.325 |
| Breathiness | 2.43 ± 0.76 | 1.23 ± 0.93 3 | 2.23 ± 1.01 | 0.86 ± 1.03 3 | 0.568 | 0.332 |
| Asthenia | 1.36 ± 0.74 | 0.92 ± 0.95 | 1.08 ± 1.04 | 0.57 ± 1.02 | 0.425 | 0.364 |
| Strain | 1.14 ± 1.10 | 0.85 ± 0.69 | 0.77 ± 1.01 | 0.36 ± 0.63 | 0.368 | 0.066 |
| Variable | Operation Effect (Pre- vs. Post- op) | Age Effect (Age vs. Variable) | BMI Effect (BMI vs. Variable) | Sex Effect (Sex vs. Variable) | ||||
|---|---|---|---|---|---|---|---|---|
| F | p | F | p | F | p | F | p | |
| VHI-10 | 29.909 | 0.012 | 3.528 | 0.201 | 1.728 | 0.319 | 3.528 | 0.201 |
| MPT (sec) | 6.152 | 0.020 | 0.006 | 0.940 | 0.026 | 0.873 | 0.003 | 0.956 |
| F0 (Hz) | 8.017 | 0.009 | 0.031 | 0.861 | 0.568 | 0.458 | 0.241 | 0.627 |
| Jitter | 7.097 | 0.013 | 0.217 | 0.645 | 0.602 | 0.445 | 0.152 | 0.700 |
| Shimmer | 1.476 | 0.235 | 0.167 | 0.686 | 1.110 | 0.302 | 1.390 | 0.249 |
| NHR | 4.694 | 0.039 | 0.544 | 0.467 | 0.029 | 0.865 | 0.018 | 0.893 |
| GRBAS sum | 18.761 | <0.001 | 0.007 | 0.933 | 0.439 | 0.514 | 0.137 | 0.715 |
| Grade | 13.848 | 0.001 | 0.280 | 0.602 | 1.223 | 0.280 | 0.065 | 0.800 |
| Roughness | 5.297 | 0.030 | 0.006 | 0.941 | 0.002 | 0.964 | 0.037 | 0.848 |
| Breathiness | 20.911 | <0.001 | 0.478 | 0.496 | 0.337 | 0.567 | 0.111 | 0.742 |
| Asthenia | 5.233 | 0.031 | 0.531 | 0.473 | 0.018 | 0.895 | 5.836 | 0.024 |
| Strain | 4.239 | 0.05 | 0.076 | 0.785 | 0.012 | 0.914 | 0.060 | 0.809 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-T.; Tsai, M.-S.; Chang, G.-H.; Lee, L.-A.; Yang, M.-Y.; Yang, Y.-H.; Wu, C.-Y.; Hsu, C.-M. Patient-Related Factors of Medialization Laryngoplasty with Autologous Thyroid Cartilage. Healthcare 2020, 8, 521. https://doi.org/10.3390/healthcare8040521
Tsai Y-T, Tsai M-S, Chang G-H, Lee L-A, Yang M-Y, Yang Y-H, Wu C-Y, Hsu C-M. Patient-Related Factors of Medialization Laryngoplasty with Autologous Thyroid Cartilage. Healthcare. 2020; 8(4):521. https://doi.org/10.3390/healthcare8040521
Chicago/Turabian StyleTsai, Yao-Te, Ming-Shao Tsai, Geng-He Chang, Li-Ang Lee, Ming-Yu Yang, Yao-Hsu Yang, Chin-Yuan Wu, and Cheng-Ming Hsu. 2020. "Patient-Related Factors of Medialization Laryngoplasty with Autologous Thyroid Cartilage" Healthcare 8, no. 4: 521. https://doi.org/10.3390/healthcare8040521