Subjective and Objective Mental and Physical Functions Affect Subjective Cognitive Decline in Community-Dwelling Elderly Japanese People

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- (i)
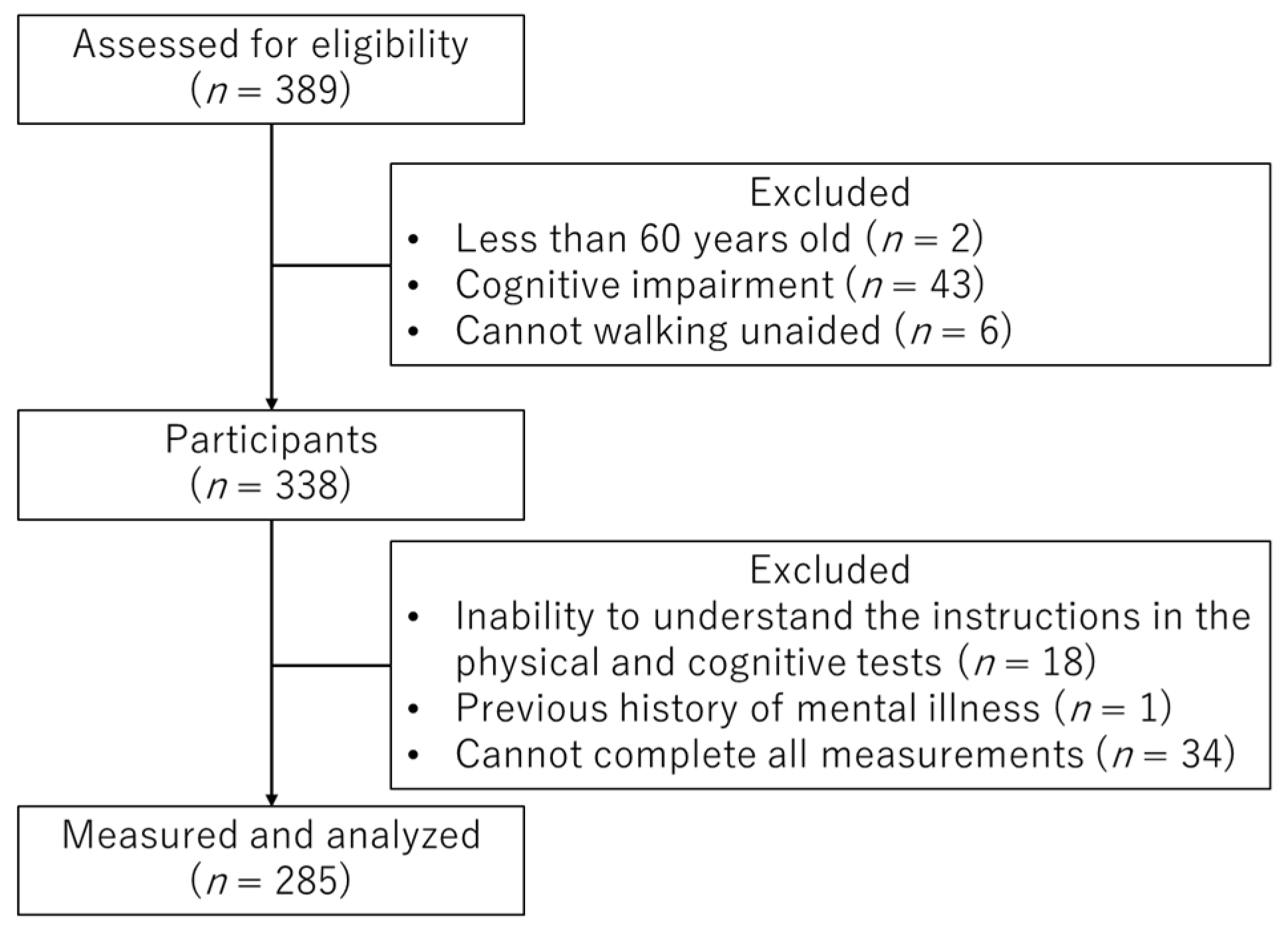
- Aged over 60 years;
- (ii)
- No warning signs of marked cognitive impairment, with a score of less than 24 in the Mini-Mental State Examination (MMSE);
- (iii)
- No difficulties in walking unaided.
- (i)
- Inability to understand instructions in the physical and cognitive tests;
- (ii)
- Previous history of mental illness;
- (iii)
- Cannot complete all measurements.
3. Results
4. Discussion
- (i)
- Multidomain lifestyle intervention, comprising exercise and dietary guidance, cognitive training, social participation, and individualized health guidance to alleviate depressive symptoms [54].
- (ii)
- (i)
- The KCL-CF scores were high only in a small number of subjects. In the future, it will be necessary to have larger sample sizes and thus investigate the effects of subjective and objective mental and physical functions on SCD severity.
- (ii)
- The only tool used for the evaluation of SCD was a self-reporting questionnaire. The biomarker tests needed to define APOEε4 genotypes and preclinical AD were not performed [57]. In the future, it will be necessary to perform biomarker tests to evaluate SCD and thus judge whether similar results will be obtained.
- (iii)
- We used a cross-sectional design; thus, the causality of the relationships found cannot be ascertained. To clarify the relationships between changes in each index and SCD onset, a longitudinal study will be necessary in the future.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ohara, T.; Hata, J.; Yoshida, D.; Mukai, N.; Nagata, M.; Iwaki, T.; Kitazono, T.; Kanba, S.; Kiyohara, Y.; Ninomiya, T. Trends in dementia prevalence, incidence, and survival rate in a Japanese community. Neurology 2017, 88, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Dodge, H.H.; Du, Y.; Saxton, J.A.; Ganguli, M. Cognitive domains and trajectories of functionsal independence in nondemented elderly persons. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- Crous-Bou, M.; Minguillón, C.; Gramunt, N.; Molinuevo, J.L. Alzheimer’s disease prevention: From risk factors to early intervention. Alzheimers Res. 2017, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Sone, D.; Maruo, K.; Shimada, H.; Suzuki, K.; Watanabe, H.; Matsuda, H.; Mizusawa, H. Analysis of risk factors for mild cognitive decline based on word list memory test results and questionnaire responses in healthy Japanese individuals registered in an online database. PLoS ONE 2018, 13, e197466. [Google Scholar] [CrossRef] [Green Version]
- Dubois, B.; Hampel, H.; Feldman, H.H.; Scheltens, P.; Aisen, P.; Andrieu, S.; Bakardjian, H.; Benali, H.; Bertram, L.; Blennow, K.; et al. Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement. 2016, 12, 292–323. [Google Scholar] [CrossRef]
- Molinuevo, J.L.; Rabin, L.A.; Amariglio, R.; Buckley, R.; Dubois, B.; Ellis, K.A.; Ewers, M.; Hampel, H.; Klöppel, S.; Rami, L.; et al. Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. 2017, 13, 296–311. [Google Scholar] [CrossRef] [Green Version]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Gifford, K.A.; Liu, D.; Carmona, H.; Lu, Z.; Romano, R.; Tripodis, Y.; Martin, B.; Kowall, N.; Jefferson, A.L. Inclusion of an informant yields strong associations between cognitive complaint and longitudinal cognitive outcomes in non-demented elders. J. Alzheimers Dis. 2015, 43, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Glodzik-Sobanska, L.; Reisberg, B.; De Santi, S.; Babb, J.S.; Pirraglia, E.; Rich, K.E.; Brys, M.; de Leon, M.J. Subjective memory complaints: Presence, severity and future outcome in normal older subjects. Dement. Geriatr. Cogn. Disord. 2007, 24, 177–184. [Google Scholar] [CrossRef]
- Gifford, K.A.; Liu, D.; Lu, Z.; Tripodis, Y.; Cantwell, N.G.; Palmisano, J.; Kowall, N.; Jefferson, A.L. The source of cognitive complaints predicts diagnostic conversion differentially among nondemented older adults. Alzheimers Dement. 2014, 10, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; van Belle, G.; Crane, P.K.; Kukull, W.A.; Bowen, J.D.; McCormick, W.C.; Larson, E.B. Subjective memory deterioration and future dementia in people aged 65 and older. J. Am. Geriatr. Soc. 2004, 52, 2045–2051. [Google Scholar] [CrossRef] [PubMed]
- Clarnette, R.M.; Almeida, O.P.; Forstl, H.; Paton, A.; Martins, R.N. Clinical characteristics of individuals with subjective memory loss in Western Australia: Results from a cross-sectional survey. Int. J. Geriatr. Psychiatry 2001, 16, 168–174. [Google Scholar] [CrossRef]
- Montejo, P.; Montenegro, M.; Fernandez, M.A.; Maestu, F. Subjective memory complaints in the elderly: Prevalence and influence of temporal orientation, depression and quality of life in a population-based study in the city of Madrid. Aging Ment. Health 2011, 15, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Siddarth, P.; Ercoli, L.M.; Merrill, D.A.; Torres-Gil, F.; Small, G.W. Modifiable risk factors for Alzheimer disease and subjective memory impairment across age groups. PLoS ONE 2014, 9, e98630. [Google Scholar] [CrossRef] [Green Version]
- Corlier, F.W.; Shaw, C.; Hayes-Larson, E.; Mungas, D.; Tomaszewski Farias, S.; Glymour, M.M.; Whitmer, R.A.; Mayeda, E.R. Association between cognitive test performance and subjective cognitive decline in a diverse cohort of older adults: Findings from the KHANDLE study. Alzheimer Dis. Assoc. Disord. 2020. [Google Scholar] [CrossRef]
- Dux, M.C.; Woodard, J.L.; Calamari, J.E.; Messina, M.; Arora, S.; Chik, H.; Pontarelli, N. The moderating role of negative affect on objective verbal memory performance and subjective memory complaints in healthy older adults. J. Int. Neuropsychol. Soc. 2008, 14, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Grambaite, R.; Hessen, E.; Auning, E.; Aarsland, D.; Selnes, P.; Fladby, T. Correlates of subjective and mild cognitive decline: Depressive symptoms and CSF biomarkers. Dement. Geriatr. Cogn. Dis. Extra 2013, 3, 291–300. [Google Scholar] [CrossRef]
- Montejo Carrasco, P.; Montenegro-Peña, M.; López-Higes, R.; Estrada, E.; Prada Crespo, D.; Montejo Rubio, C.; García Azorín, D. Subjective memory complaints in healthy older adults: Fewer complaints associated with depression and perceived health, more complaints also associated with lower memory performance. Arch. Gerontol. Geriatr. 2017, 70, 28–37. [Google Scholar] [CrossRef]
- Sánchez-Benavides, G.; Grau-Rivera, O.; Cacciaglia, R.; Suárez-Calvet, M.; Falcon, C.; Minguillon, C.; Gramunt, N.; Sala-Vila, A.; Gispert, J.D.; Molinuevo, J.L. Distinct cognitive and brain morphological features in healthy subjects unaware of informant-reported cognitive decline. J. Alzheimers Dis. 2018, 65, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Turvey, C.L.; Schultz, S.; Arndt, S.; Wallace, R.B.; Herzog, R. Memory complaint in a community sample aged 70 and older. J. Am. Geriatr. Soc. 2000, 48, 1435–1441. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.C.; Huang, L.Y.; Chen, C.K.; Lin, C.; Shyu, Y.C.; Chen, Y.L.; Huang, W.Y.; Lin, C.P. Subjective cognitive decline in the community is affected at multiple aspects of mental health and life quality: A cross-sectional study of the community medicine of Keelung Chang Gung Memorial Hospital. Dement. Geriatr. Cogn. Dis. Extra 2019, 9, 152–162. [Google Scholar] [CrossRef]
- Comijs, H.C.; Deeg, D.J.; Dik, M.G.; Twisk, J.W.; Jonker, C. Memory complaints; the association with psycho-affective and health problems and the role of personality characteristics. A 6-year follow-up study. J. Affect. Disord. 2002, 72, 157–165. [Google Scholar] [CrossRef]
- Gallacher, J.; Bayer, A.; Fish, M.; Pickering, J.; Pedro, S.; Dunstan, F.; Ebrahim, S.; Ben-Shlomo, Y. Does anxiety affect risk of dementia? Findings from the Caerphilly Prospective Study. Psychosom. Med. 2009, 71, 659–666. [Google Scholar] [CrossRef]
- Hirose, J.; Nagata, T.; Ogushi, M.; Okamoto, N.; Taniwaki, T.; Oka, K.; Togami-Tomiguchi, W.; Koga, H.; Hayashi, K.; Usuku, K.; et al. Validation of each category of Kihon Checklist for assessing physical functioning, nutrition and cognitive status in a community-dwelling older Japanese cohort. Epidemiol. Open Access 2017, 7, 326. [Google Scholar] [CrossRef]
- Yoon, B.; Choi, S.H.; Jeong, J.H.; Park, K.W.; Kim, E.J.; Hwang, J.; Jang, J.W.; Kim, H.J.; Hong, J.Y.; Lee, J.M.; et al. Balance and mobility performance along the Alzheimer’s disease spectrum. J. Alzheimers Dis. 2020, 73, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.; Tree, J.J.; Thornton, I.M.; Tales, A. Subjective cognitive decline in 55–65-year-old adults is associated with negative affective symptoms, neuroticism, and poor quality of life. J. Alzheimers Dis. 2019, 67, 1367–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stites, S.D.; Harkins, K.; Rubright, J.D.; Karlawish, J. Relationships between cognitive complaints and quality of life in older adults with mild cognitive decline, mild Alzheimer disease dementia, and normal cognition. Alzheimer Dis. Assoc. Disord. 2018, 32, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, S.; Devanand, D.; Gurland, B. A link between subjective perceptions of memory and physical function: Implications for subjective cognitive decline. J. Alzheimers Dis. 2018, 61, 1387–1398. [Google Scholar] [CrossRef]
- Toyoshima, K.; Inoue, T.; Masuya, J.; Ichiki, M.; Fujimura, Y.; Kusumi, I. Evaluation of subjective cognitive functions using the cognitive complaints in bipolar disorder rating assessment (COBRA) In Japanese Adults. Neuropsychiatr. Dis. Treat 2019, 15, 2981–2990. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y.; Kim, J.K.; Davarian, S.; Hagedorn, A.; Crimmins, E.M. Cognitive performance among older persons in Japan and the United States. J. Am. Geriatr. Soc. 2020, 68, 354–361. [Google Scholar] [CrossRef]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, P.; Sampaio, R.A.C.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Kihon Checklist: Systematic review. Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Sugawara, Y.; Hozawa, A.; Tsuji, I. Predictive ability of a simple subjective memory complaints scale for incident dementia: Evaluation of Japan’s national checklist, the “Kihon Checklist”. Geriatr. Gerontol. Int. 2017, 17, 1300–1305. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, Y.; Sato, S.; Takahashi, M.; Takeda, N.; Matsushita, M.; Kitabatake, Y.; Maruo, K.; Arao, T. The association of single and combined factors of sedentary behavior and physical activity with subjective cognitive complaints among community-dwelling older adults: Cross-sectional study. PLoS ONE 2018, 13, e195384. [Google Scholar] [CrossRef]
- Okura, M.; Ogita, M.; Arai, H. Self-reported cognitive frailty predicts adverse health outcomes for community-dwelling older adults based on an analysis of sex and age. J. Nutr. Health Aging 2019, 23, 654–664. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ideno, Y.; Takayama, M.; Hayashi, K.; Takagi, H.; Sugai, Y. Evaluation of a Japanese version of the Mini-Mental State Examination in elderly persons. Geriatr. Gerontol. Int. 2012, 12, 310–316. [Google Scholar] [CrossRef]
- Sugishita, M.; Hemmi, I.; Takeuchi, T. Reexamination of the validity and reliability of the Japanese version of the Mini-Mental State Examination (MMSE-J). J. Cogn. Neurosci. 2016, 18, 168–183. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Test-retest reliability of hand-held dynamometry during a single session of strength assessment. Phys. Ther. 1986, 66, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Martin, H.J.; Yule, V.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Aihie Sayer, A. Is hand-held dynamometry useful for the measurement of quadriceps strength in older people? A comparison with the gold standard Bodex dynamometry. Gerontology 2006, 52, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Katoh, M.; Isozaki, K.; Sakanoue, N.; Miyahara, T. Reliability of isometric knee extension muscle Strength measurement using a hand-held zynamometer with a Belt: A study of test-retest reliability in healthy elderly subjects. J. Phys. Sci 2010, 22, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Fukuhara, S.; Suzukamo, Y. Manual of the SF-8 Japanese Version; Institute for Health Outcome & Process Evaluation Research: Kyoto, Japan, 2004; pp. 47–70. Available online: https://www.sf-36.jp/qol/sf8.html (accessed on 16 July 2020).
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Dewey, J.; Gandek, B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8 Health Survey; Quality Metric: Boston, MA, USA, 2001. [Google Scholar]
- Buitenweg, J.I.V.; Van De Ven, R.M.; Ridderinkhof, K.R.; Murre, J.M.J. Does cognitive flexibility training enhance subjective mental functioning in healthy older adults? Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2019, 26, 688–710. [Google Scholar] [CrossRef]
- Serra, M.C.; Addison, O.; Giffuni, J.; Paden, L.; Morey, M.C.; Katzel, L. Physical function does not predict care assessment need score in older veterans. J. Appl. Gerontol. 2019, 38, 412–423. [Google Scholar] [CrossRef]
- Okura, M.; Ogita, M.; Yamamoto, M.; Nakai, T.; Numata, T.; Arai, H. The relationship of community activities with cognitive decline and depressive mood independent of mobility disorder in Japanese older adults. Arch. Gerontol. Geriatr. 2017, 70, 54–61. [Google Scholar] [CrossRef]
- Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Honkura, K.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Green tea consumption and the risk of incident dementia in elderly Japanese: The Ohsaki Cohort 2006 Study. Am. J. Geriatr. Psychiatry 2016, 24, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Watson, D. Intraindividual and interindividual analyses of positive and negative affect: Their relation to health complaints, perceived stress, and daily activities. J. Pers. Soc. Psychol. 1988, 54, 1020–1030. [Google Scholar] [CrossRef]
- Jason, L.A.; Torres-Harding, S.R.; Jurgens, A.; Helgerson, J. Comparing the Fukuda et al. criteria and the Canadian case definition for chronic fatigue syndrome. J. Chronic Fatigue Syndr. 2004, 12, 37–52. [Google Scholar] [CrossRef]
- Kumar, S.; Tran, J.; Moseson, H.; Tai, C.; Glenn, J.M.; Madero, E.N.; Krebs, C.; Bott, N.; Juusola, J.L. The impact of the virtual cognitive health program on the cognition and mental health of older adults: Pre-post 12-month pilot study. JMIR Aging 2018, 1, e12031. [Google Scholar] [CrossRef] [PubMed]
- Metternich, B.; Schmidtke, K.; Härter, M.; Dykierek, P.; Hüll, M. Development and evaluation of a group therapy for functionsal memory and attention disorder. Psychother. Psychosom. Med. Psychol. 2010, 60, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Bhome, R.; Berry, A.J.; Huntley, J.D.; Howard, R.J. Interventions for subjective cognitive decline: Systematic review and meta-analysis. BMJ Open 2018, 8, e21610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, L.A.; Smart, C.M.; Amariglio, R.E. Subjective cognitive decline in preclinical Alzheimer’s disease. Annu. Rev. Clin. Psychol. 2017, 13, 369–396. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Number of Subjects/Frequencies |
|---|---|
| KCL-CF score (0/1/2/3; n) | 184/78/22/1 |
| Frequency of subjective memory item endorsement | |
| Do your family or your friends point out your memory loss? | 15.1% |
| Do you make a call by looking up phone numbers? | 2.1% |
| Do you find yourself not knowing today’s date? | 26.7% |
| Variable | Total (n = 285) | SCD (n = 101) | Non-SCD (n = 184) | Effect Size (r, V) | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attribute | Age (yr) | 73.3 | ± | 6.3 | 73.7 | ± | 6.2 | 73.1 | ± | 6.3 | 0.05 | 0.444 | |
| Sex: Male/female | 51/234 | 16/85 | 35/149 | 0.04 | 0.628 | a | |||||||
| Height (cm) | 153.0 | ± | 7.9 | 152.7 | ± | 7.5 | 153.2 | ± | 8.1 | <0.01 | 0.981 | ||
| Weight (kg) | 52.6 | ± | 9.4 | 51.6 | ± | 8.7 | 53.1 | ± | 9.7 | 0.08 | 0.201 | b | |
| BMI (kg/m2) | 22.4 | ± | 3.3 | 22.1 | ± | 3.1 | 22.6 | ± | 3.3 | 0.07 | 0.222 | b | |
| Educational history (yr) | 11.6 | ± | 2.1 | 11.3 | ± | 1.9 | 11.7 | ± | 2.2 | 0.09 | 0.137 | ||
| Objective mental function | MMSE (score) | 27.6 | ± | 2.2 | 27.3 | ± | 2.4 | 27.8 | ± | 2.1 | 0.12 | 0.049 | |
| GDS-5 (score) | 0.6 | ± | 1.0 | 1 | ± | 1.2 | 0.4 | ± | 0.8 | 0.26 | <0.001 | ||
| Objective physical function | TUG (s) | 6.1 | ± | 1.7 | 6.2 | ± | 1.2 | 6.1 | ± | 1.9 | 0.12 | 0.044 | |
| Knee extension strength (kg) | 17.8 | ± | 5.7 | 16.6 | ± | 5.2 | 18.4 | ± | 5.8 | 0.15 | 0.012 | ||
| Subjective mental function | MCS | 52.2 | ± | 4.9 | 50.7 | ± | 5.9 | 53 | ± | 4.1 | 0.18 | 0.003 | |
| Subjective physical function | PCS | 48.7 | ± | 6.2 | 48.2 | ± | 6.4 | 49 | ± | 6.1 | 0.08 | 0.181 | |
| Variable | B | S.E. | Wald | p | Exp (B) | 95% CI for Exp (B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Attribute | Age (yr) | −0.010 | 0.028 | 0.128 | 0.720 | 0.990 | 0.937 | 1.046 |
| Sex | 0.172 | 0.382 | 0.203 | 0.652 | 1.188 | 0.562 | 2.512 | |
| Educational history (yr) | −0.027 | 0.077 | 0.122 | 0.727 | 0.974 | 0.838 | 1.131 | |
| Objective mental function | MMSE | −0.108 | 0.069 | 2.432 | 0.119 | 0.898 | 0.784 | 1.028 |
| GDS-5 | 0.474 | 0.159 | 8.865 | 0.003 | 1.607 | 1.176 | 2.196 | |
| Objective physical function | TUG | −0.099 | 0.108 | 0.841 | 0.359 | 0.906 | 0.734 | 1.119 |
| Knee extension strength | −0.026 | 0.029 | 0.760 | 0.383 | 0.975 | 0.920 | 1.033 | |
| Subjective mental function | MCS | −0.084 | 0.031 | 7.496 | 0.006 | 0.919 | 0.866 | 0.976 |
| Subjective physical function | PCS | −0.032 | 0.024 | 1.736 | 0.188 | 0.968 | 0.923 | 1.016 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goda, A.; Murata, S.; Nakano, H.; Shiraiwa, K.; Abiko, T.; Nonaka, K.; Iwase, H.; Anami, K.; Horie, J. Subjective and Objective Mental and Physical Functions Affect Subjective Cognitive Decline in Community-Dwelling Elderly Japanese People. Healthcare 2020, 8, 347. https://doi.org/10.3390/healthcare8030347
Goda A, Murata S, Nakano H, Shiraiwa K, Abiko T, Nonaka K, Iwase H, Anami K, Horie J. Subjective and Objective Mental and Physical Functions Affect Subjective Cognitive Decline in Community-Dwelling Elderly Japanese People. Healthcare. 2020; 8(3):347. https://doi.org/10.3390/healthcare8030347
Chicago/Turabian StyleGoda, Akio, Shin Murata, Hideki Nakano, Kayoko Shiraiwa, Teppei Abiko, Koji Nonaka, Hiroaki Iwase, Kunihiko Anami, and Jun Horie. 2020. "Subjective and Objective Mental and Physical Functions Affect Subjective Cognitive Decline in Community-Dwelling Elderly Japanese People" Healthcare 8, no. 3: 347. https://doi.org/10.3390/healthcare8030347