Association of Low Bone Mass with Decreased Skeletal Muscle Mass: A Cross-Sectional Study of Community-Dwelling Older Women

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
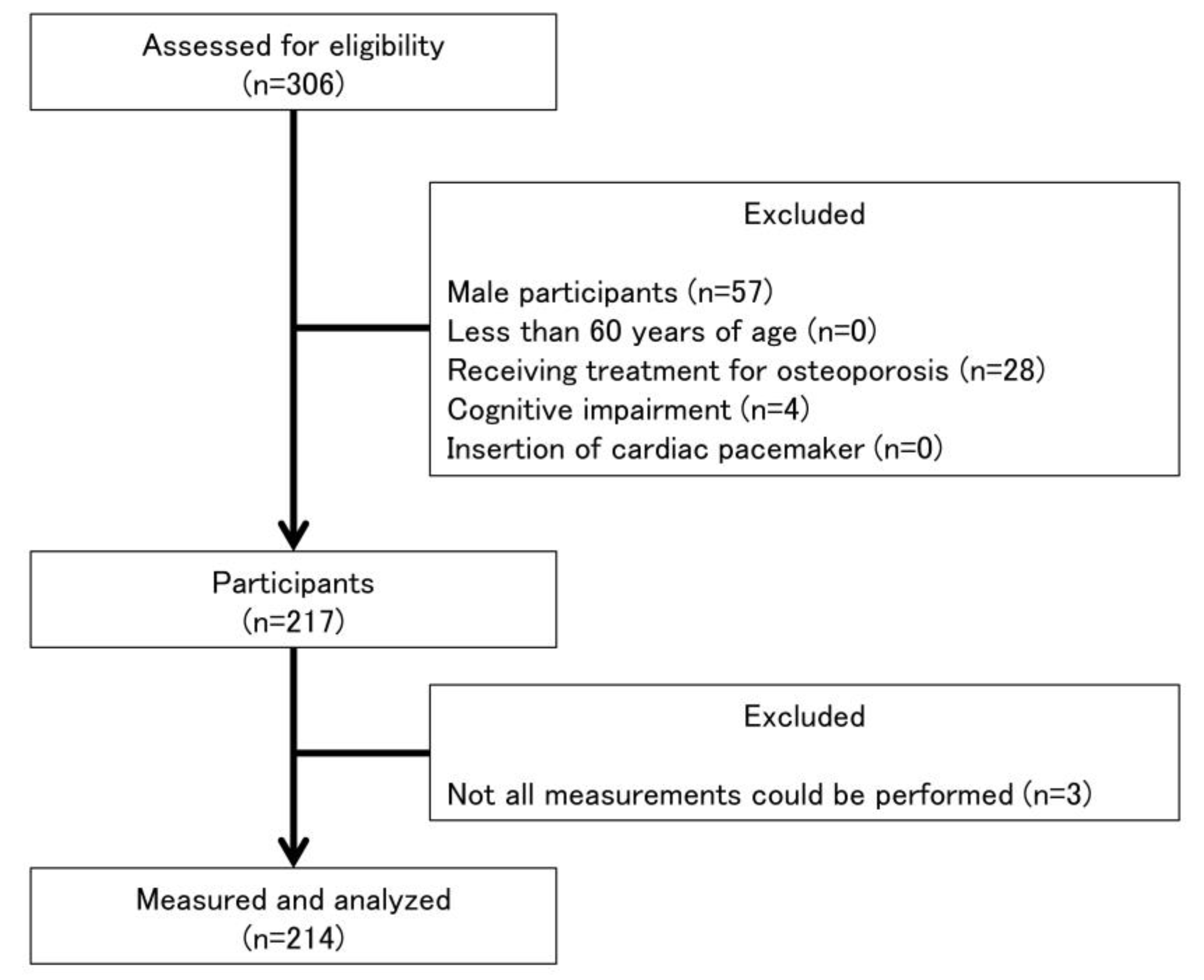
2.1. Participants
2.2. Bone Mass
2.3. Skeletal Muscle Mass
2.4. Muscle Strength
2.5. Physical Performance
2.6. Sarcopenia
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kiebzak, G.M. Age-Related Bone Changes. Exp. Gerontol. 1991, 26, 171–187. [Google Scholar] [CrossRef]
- WHO Scientific Group. Prevention and Management of Osteoporosis. World Health Organ. Tech. Res. Ser. 2003, 921, 1–164. [Google Scholar]
- Cummings, S.R.; Nevitt, M.C.; Browner, W.S.; Stone, K.; Fox, K.M.; Ensrud, K.E.; Cauley, J.; Black, D.; Vogt, T.M. Risk Factors for Hip Fracture in White Women. Study of Osteoporotic Fractures Research Group. N. Engl. J. Med. 1995, 332, 767–773. [Google Scholar] [CrossRef]
- Tang, V.L.; Sudore, R.; Cenzer, I.S.; Boscardin, W.J.; Smith, A.; Ritchie, C.; Wallhagen, M.; Finlayson, E.; Petrillo, L.; Covinsky, K. Rates of Recovery to Pre-Fracture Function in Older Persons with Hip Fracture: An Observational Study. J. Gen. Intern. Med. 2017, 32, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, E.; Litwic, A.; Cooper, C.; Dennison, E. Determinants of Muscle and Bone Aging. J. Cell Physiol. 2015, 230, 2618–2625. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, D.J.; Piasecki, M.; Atherton, P.J. The Age-Related Loss of Skeletal Muscle Mass and Function: Measurement and Physiology of Muscle Fibre Atrophy and Muscle Fibre Loss in Humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.M.; Han, J.; Won, Y.Y. Sarcopenia and Osteoporosis. Hip. Pelvis. 2015, 27, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Kawao, N.; Kaji, H. Interactions Between Muscle Tissues and Bone Metabolism. J. Cell. Biochem. 2015, 116, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Won, C.W.; Kim, B.S.; Choi, H.R. The Association Between the Low Muscle Mass and Osteoporosis in Elderly Korean People. J. Korean Med. Sci. 2014, 29, 995–1000. [Google Scholar] [CrossRef]
- Coin, A.; Perissinotto, E.; Enzi, G.; Zamboni, M.; Inelmen, E.M.; Frigo, A.C.; Manzato, E.; Busetto, L.; Buja, A.; Sergi, G. Predictors of Low Bone Mineral Density in the Elderly: The Role of Dietary Intake, Nutritional Status and Sarcopenia. Eur. J. Clin. Nutr. 2008, 62, 802–809. [Google Scholar] [CrossRef] [Green Version]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation Between Muscle Strength and Muscle Mass, and Their Association with Walking Speed, in Community-Dwelling Elderly Japanese Individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef]
- Krieg, M.A.; Barkmann, R.; Gonnelli, S.; Stewart, A.; Bauer, D.C.; Del Rio Barquero, L.; Kaufman, J.J.; Lorenc, R.; Miller, P.D.; Olszynski, W.P.; et al. Quantitative Ultrasound in the Management of Osteoporosis: The 2007 ISCD Official Positions. J. Clin. Densitom. 2008, 11, 163–187. [Google Scholar] [CrossRef]
- Nonaka, K.; Murata, S.; Shiraiwa, K.; Abiko, T.; Nakano, H.; Iwase, H.; Naito, K.; Horie, J. Physical Characteristics Vary According to Body Mass Index in Japanese Community-Dwelling Elderly Women. Geriatrics 2018, 3, 87. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Yaginuma, Y.; Fujita, E.; Thiebaud, R.S.; Kawanishi, M.; Akamine, T. Associations of Sit-Up Ability with Sarcopenia Classification Measures in Japanese Older Women. Interv. Med. Appl. Sci. 2016, 8, 152–157. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-Retest Reliability of Hand-Held Dynamometry During a Single Session of Strength Assessment. Phys. Ther. 1986, 66, 206–209. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Kamide, N.; Fukuda, M.; Miura, H. The Relationship between Bone Density and the Physical Performance of Ambulatory Patients with Parkinson’s Disease. J. Physiol. Anthropol. 2008, 27, 7–10. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Makizako, H.; Kiyama, R.; Tomioka, K.; Nakai, Y.; Kubozono, T.; Takenaka, T.; Ohishi, M. The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women. Int. J. Environ. Res. Public Health 2019, 16, 1228. [Google Scholar] [CrossRef] [Green Version]
- Miyakoshi, N.; Hongo, M.; Mizutani, Y.; Shimada, Y. Prevalence of Sarcopenia in Japanese Women with Osteopenia and Osteoporosis. J. Bone. Miner. Metab. 2013, 31, 556–561. [Google Scholar] [CrossRef]
- Genaro, P.S.; Pereira, G.A.; Pinheiro, M.M.; Szejnfeld, V.L.; Martini, L.A. Influence of Body Composition on Bone Mass in Postmenopausal Osteoporotic Women. Arch. Gerontol. Geriatr. 2010, 51, 295–298. [Google Scholar] [CrossRef]
- He, H.; Liu, Y.; Tian, Q.; Papasian, C.J.; Hu, T.; Deng, H.W. Relationship of Sarcopenia and Body Composition with Osteoporosis. Osteoporos. Int. 2016, 27, 473–482. [Google Scholar] [CrossRef]
- Kaji, H. Interaction between Muscle and Bone. J. Bone. Metab. 2014, 21, 29–40. [Google Scholar] [CrossRef] [Green Version]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The Loss of Skeletal Muscle Strength, Mass, and Quality in Older Adults: The Health, Aging and Body Composition Study. J. Gerontol. Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Oh, S.L.; Kim, H.J.; Woo, S.; Cho, B.L.; Song, M.; Park, Y.H.; Lim, J.Y.; Song, W. Effects of an Integrated Health Education and Elastic Band Resistance Training Program on Physical Function and Muscle Strength in Community-Dwelling Elderly Women: Healthy Aging and Happy Aging II Study. Geriatr. Gerontol. Int. 2017, 17, 825–833. [Google Scholar] [CrossRef]
- Bijlsma, A.Y.; Meskers, M.C.; Molendijk, M.; Westendorp, R.G.; Sipilä, S.; Stenroth, L.; Sillanpää, E.; McPhee, J.S.; Jones, D.A.; Narici, M.; et al. Diagnostic Measures for Sarcopenia and Bone Mineral Density. Osteoporos. Int. 2013, 24, 2681–2691. [Google Scholar] [CrossRef]
- Lindsey, C.; Brownbill, R.A.; Bohannon, R.A.; Ilich, J.Z. Association of Physical Performance Measures with Bone Mineral Density in Postmenopausal Women. Arch. Phys. Med. Rehabil. 2005, 86, 1102–1107. [Google Scholar] [CrossRef]
- Blain, H.; Vuillemin, A.; Teissier, A.; Hanesse, B.; Guillemin, F.; Jeandel, C. Influence of Muscle Strength and Body Weight and Composition on Regional Bone Mineral Density in Healthy Women Aged 60 Years and Over. Gerontology 2001, 47, 207–212. [Google Scholar] [CrossRef]
- Falsarella, G.R.; Coimbra, I.B.; Barcelos, C.C.; Iartelli, I.; Montedori, K.T.; Santos, M.N.; Neri, A.L.; Coimbra, A.M. Influence of Muscle Mass and Bone Mass on the Mobility of Elderly Women: An observational Study. BMC Geriatr. 2014, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- Pasco, J.A.; Holloway, K.L.; Brennan-Olsen, S.L.; Moloney, D.J.; Kotowicz, M.A. Muscle Strength and Areal Bone Mineral Density at the Hip in Women: A Cross-Sectional Study. BMC Musculoskelet. Disord. 2015, 16, 124. [Google Scholar] [CrossRef] [Green Version]
- Sjöblom, S.; Suuronen, J.; Rikkonen, T.; Honkanen, R.; Kröger, H.; Sirola, J. Relationship between Postmenopausal Osteoporosis and the Components of Clinical Sarcopenia. Maturitas 2013, 75, 175–180. [Google Scholar] [CrossRef]
- Lima, R.M.; de Oliveira, R.J.; Raposo, R.; Neri, S.G.R.; Gadelha, A.B. Stages of Sarcopenia, Bone Mineral Density, and the Prevalence of Osteoporosis in Older Women. Arch. Osteoporos. 2019, 14, 38. [Google Scholar] [CrossRef]
- Yamada, M.; Nishiguchi, S.; Fukutani, N.; Tanigawa, T.; Yukutake, T.; Kayama, H.; Aoyama, T.; Arai, H. Prevalence of Sarcopenia in Community-Dwelling Japanese Older Adults. J. Am. Med. Dir. Assoc. 2013, 14, 911–915. [Google Scholar] [CrossRef]
- Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Degens, H.; Fuleihan, G.E.H.; Josse, R.; Lips, P.; Torres, J.M.; Rizzoli, R.; et al. Impact of Nutrition on Muscle Mass, Strength, and Performance in Older Adults. Osteoporos. Int. 2013, 24, 1555–1566. [Google Scholar] [CrossRef]
- Liberman, K.; Forti, L.N.; Beyer, I.; Bautmans, I. The Effects of Exercise on Muscle Strength, Body Composition, Physical Functioning and the Inflammatory Profile of Older Adults: A Systematic Review. Curr. Opin. Clin. Nutr. Metab. Care. 2017, 20, 30–53. [Google Scholar] [CrossRef]
- Huh, J.Y. The Role of Exercise-Induced Myokines in Regulating Metabolism. Arch. Pharm. Res. 2018, 41, 14–29. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Normal Bone Mass (n = 18) | Low Bone Mass (n = 112) | Very Low Bone Mass (n = 84) | F, χ2 | p |
|---|---|---|---|---|---|
| Age (years) | 72.6 ± 7.2 | 73.7 ± 5.0 | 75.5 ± 5.4 | 3.783 | 0.024 |
| Height (cm) | 151.6 ± 6.5 | 152.1 ± 4.5 | 150.9 ± 5.9 | 1.193 | 0.305 |
| Weight (kg) | 51.6 ± 6.2 | 52.4 ± 6.5 | 48.4 ± 6.9 *** | 8.845 | <0.001 |
| BMI (kg/cm2) | 22.4 ± 2.5 | 22.7 ± 2.7 | 21.2 ± 2.7 ** | 6.11 | 0.003 |
| Diseases | |||||
| Hypertension (n, %) | 9 (50%) | 43 (38%) | 25 (30%) | 3.229 | 0.199 |
| Hyperglycemia (n, %) | 4 (22%) | 27 (24%) | 14 (17%) | 1.617 | 0.446 |
| Orthopedic disease (n, %) | 2 (11%) | 20 (18%) | 20 (24%) | 1.981 | 0.371 |
| Diabetes mellitus (n, %) | 2 (11%) | 8 (7%) | 3 (4%) | 1.947 | 0.378 |
| Cardiovascular disease (n, %) | 0 (0%) | 5 (4%) | 8 (10%) | 3.425 | 0.180 |
| Pulmonary disease (n, %) | 0 (0%) | 2 (2%) | 3 (4%) | 1.141 | 0.565 |
| Renal disease (n, %) | 0 (0%) | 2 (2%) | 1 (1%) | 0.402 | 0.817 |
| Cancer (n, %) | 0 (0%) | 0 (0%) | 1 (1%) | 1.555 | 0.460 |
| Others (n, %) | 1 (6%) | 17 (15%) | 6 (7%) | 3.745 | 0.154 |
| Variable | Normal Bone Mass (n = 18) | Low Bone Mass (n = 112) | Very Low Bone Mass (n = 84) | F, χ2 | p |
|---|---|---|---|---|---|
| Arm SMI (kg/cm2) | 1.42 ± 0.20 | 1.41 ± 0.20 | 1.34 ± 0.19 * | 3.525 | 0.031 |
| Leg SMI (kg/cm2) | 4.72 ± 0.43 | 4.69 ± 0.42 | 4.49 ± 0.39 * | 4.681 | 0.010 |
| Appendicular SMI (kg/cm2) | 6.14 ± 0.59 | 6.10 ± 0.58 | 5.83 ± 0.54 ** | 4.931 | 0.008 |
| Grip strength (kgf) | 24.4 ± 4.2 | 24.0 ± 4.0 | 23.8 ± 4.0 | 0.063 | 0.939 |
| Knee extension strength (kgf) | 21.4 ± 5.5 | 21.3 ± 4.0 | 20.0 ± 5.0 | 0.780 | 0.460 |
| Usual gait speed (m/s) | 1.44 ± 0.18 | 1.49 ± 0.23 | 1.47 ± 0.27 | 0.560 | 0.572 |
| Fastest gait speed (m/s) | 1.85 ± 0.22 | 1.86 ± 0.27 | 1.82 ± 0.30 | 0.205 | 0.814 |
| TUG (s) | 5.55 ± 0.94 | 5.58 ± 0.96 | 5.83 ± 1.16 | 0.240 | 0.787 |
| Sarcopenia (n, %) | 0 (0%) | 6 (5.4%) | 3 (3.6%) | 1.243 | 0.537 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nonaka, K.; Murata, S.; Nakano, H.; Anami, K.; Shiraiwa, K.; Abiko, T.; Goda, A.; Iwase, H.; Horie, J. Association of Low Bone Mass with Decreased Skeletal Muscle Mass: A Cross-Sectional Study of Community-Dwelling Older Women. Healthcare 2020, 8, 343. https://doi.org/10.3390/healthcare8030343
Nonaka K, Murata S, Nakano H, Anami K, Shiraiwa K, Abiko T, Goda A, Iwase H, Horie J. Association of Low Bone Mass with Decreased Skeletal Muscle Mass: A Cross-Sectional Study of Community-Dwelling Older Women. Healthcare. 2020; 8(3):343. https://doi.org/10.3390/healthcare8030343
Chicago/Turabian StyleNonaka, Koji, Shin Murata, Hideki Nakano, Kunihiko Anami, Kayoko Shiraiwa, Teppei Abiko, Akio Goda, Hiroaki Iwase, and Jun Horie. 2020. "Association of Low Bone Mass with Decreased Skeletal Muscle Mass: A Cross-Sectional Study of Community-Dwelling Older Women" Healthcare 8, no. 3: 343. https://doi.org/10.3390/healthcare8030343