

Prevalence and Risk Factors for Renal Insufficiency among Adults Living with HIV in Tanzania: Results from a Cross-Sectional Study in 2020–2021
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Participants
2.3. Current Standard of Care at the CTC
2.4. Data Collection
2.5. Variables
2.6. Data Analysis
3. Ethical Consideration
4. Results
4.1. Characteristics of the Study Population
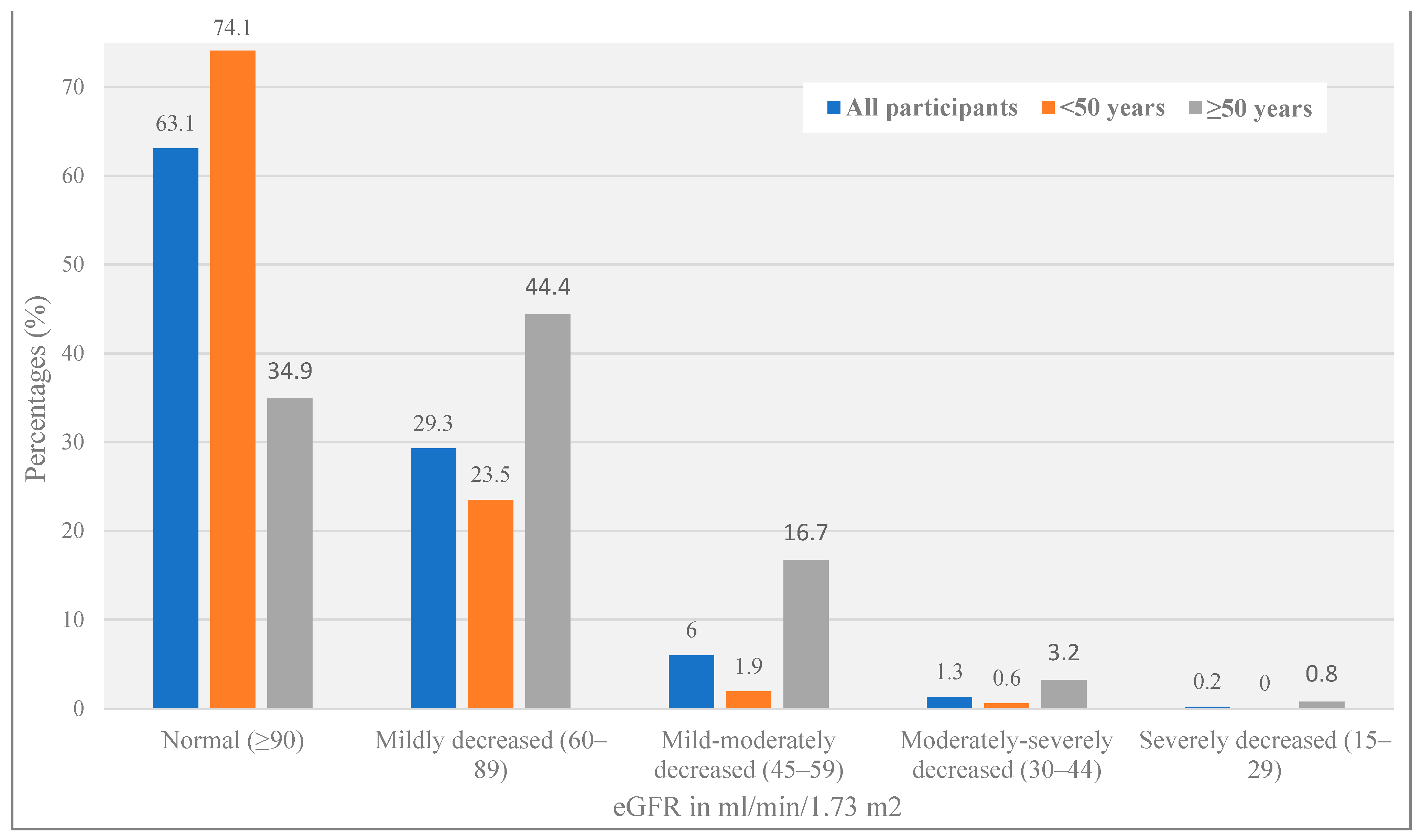
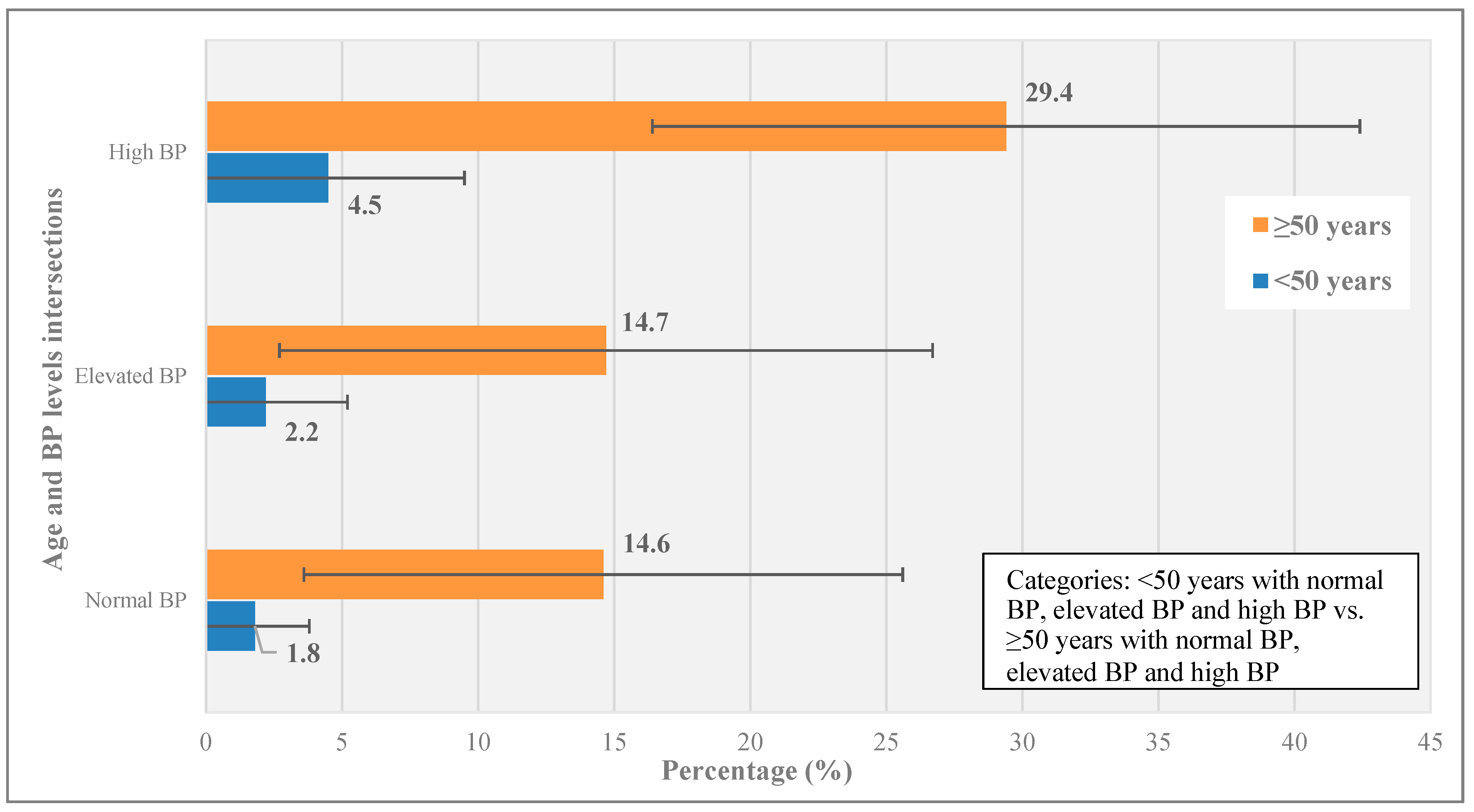
4.2. Distribution of eGFR Stage According to KDIGO 2012 Criteria by Age
4.3. Associations with Reduced eGFR
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katz, I.T.; Maughan-Brown, B. Improved life expectancy of people living with HIV: Who is left behind? Lancet HIV 2017, 4, e324–e326. [Google Scholar] [CrossRef]
- HIV/AIDS. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 21 December 2019).
- AIDSinfo. UNAIDS. Available online: http://aidsinfo.unaids.org/ (accessed on 21 May 2020).
- Venkat Narayan, K.M.; Miotti, P.G.; Anand, N.P.; Kline, L.M.; Harmston, C.; Gulakowski, R.; Vermund, S.H. HIV and noncommunicable disease comorbidities in the era of antiretroviral therapy: A vital agenda for research in low-and middle-income country settings. J. Acquir. Immune Defic. Syndr. 2014, 67 (Suppl. S1), S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Sackoff, J.E.; Hanna, D.B.; Pfeiffer, M.R.; Torian, L.V. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann. Intern. Med. 2006, 145, 397–406. [Google Scholar] [CrossRef]
- Gardner, L.I.; Holmberg, S.D.; Williamson, J.M.; Szczech, L.A.; Carpenter, C.C.J.; Rompalo, A.M.; Schuman, P.; Klein, R.S. Development of proteinuria or elevated serum creatinine and mortality in HIV-infected women. J. Acquir. Immune Defic. Syndr. 2003, 32, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.M.; Wu, J.; Jansson, J.; Wilson, D.P. Relative risk of renal disease among people living with HIV: A systematic review and meta-analysis. BMC Public Health 2012, 12, 234. [Google Scholar] [CrossRef] [PubMed]
- Ekrikpo, U.E.; Kengne, A.P.; Bello, A.K.; Effa, E.E.; Noubiap, J.J.; Salako, B.L.; Rayner, B.L.; Remuzzi, G.L.; Okpechi, I.G. Chronic kidney disease in the global adult HIV-infected population: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195443. [Google Scholar] [CrossRef] [PubMed]
- Kaze, A.D.; Ilori, T.; Jaar, B.G.; Echouffo-Tcheugui, J.B. Burden of chronic kidney disease on the African continent: A systematic review and meta-analysis. BMC Nephrol. 2018, 19, 125. [Google Scholar] [CrossRef] [PubMed]
- Mwemezi, O.; Ruggajo, P.; Mngumi, J.; Furia, F.F. Renal Dysfunction among HIV-Infected Patients on Antiretroviral Therapy in Dar es Salaam, Tanzania: A Cross-Sectional Study. Int. J. Nephrol. 2020, 2020, 8378947. [Google Scholar] [CrossRef] [PubMed]
- Kavishe, B.B.; Kweka, B.V.; Nitsch, D.; PrayGod, G.; Jeremiah, K.; Faurholt-Jepsen, D.; Filteau, S.; Olsen, M.F.; Kitilya, B.W.; Krogh-Madsen, R.; et al. Risk factors for impaired renal function in HIV-infected and HIV-uninfected adults: Cross-sectional study in North-Western Tanzania. BMC Nephrol. 2021, 22, 355. [Google Scholar] [CrossRef]
- Mapesi, H.; Okuma, J.; Franzeck, F.; Wilson, H.I.; Senkoro, E.; Byakuzana, T.; Ndege, R.; Vanobberghen, F.; Glass, T.R.; Battegay, M.; et al. Prevalence, incidence and predictors of renal impairment in persons with HIV receiving protease-inhibitors in rural Tanzania. PLoS ONE 2021, 16, e0261367. [Google Scholar] [CrossRef]
- Peck, R.N.; Shedafa, R.; Kalluvya, S.; Downs, J.A.; Todd, J.; Suthanthiran, M.; Fitzgerald, D.W.; Kataraihya, J.B. Hypertension, kidney disease, HIV and antiretroviral therapy among Tanzanian adults: A cross-sectional study. BMC Med. 2014, 12, 125. [Google Scholar] [CrossRef]
- Huang, Y.S.; Chan, C.K.; Tsai, M.S.; Lee, K.Y.; Lin, S.W.; Chang, S.Y.; Hung, C.-C.; Chang, S.-C. Kidney dysfunction associated with tenofovir exposure in human immunodeficiency virus-1-infected Taiwanese patients. J. Microbiol. Immunol. Infect. 2017, 50, 595–603. [Google Scholar] [CrossRef]
- Suzuki, S.; Nishijima, T.; Kawasaki, Y.; Kurosawa, T.; Mutoh, Y.; Kikuchi, Y.; Gatanaga, H.; Oka, S. Effect of Tenofovir Disoproxil Fumarate on Incidence of Chronic Kidney Disease and Rate of Estimated Glomerular Filtration Rate Decrement in HIV-1-Infected Treatment-Naïve Asian Patients: Results from 12-Year Observational Cohort. AIDS Patient Care STDS 2017, 31, 105–112. [Google Scholar] [CrossRef]
- Swanepoel, C.R.; Atta, M.G.; D’Agati, V.D.; Estrella, M.M.; Fogo, A.B.; Naicker, S.; Post, F.A.; Wearne, N.; Winkler, S.A.; Cheung, M.; et al. Kidney disease in the setting of HIV infection: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2018, 93, 545–559. [Google Scholar] [CrossRef]
- Jotwani, V.; Li, Y.; Grunfeld, C.; Choi, A.I.; Shlipak, M.G. Risk factors for ESRD in HIV-infected individuals: Traditional and HIV-related factors. Am. J. Kidney Dis. 2012, 59, 628–635. [Google Scholar] [CrossRef]
- Ottaru, T.A.; Kwesigabo, G.P.; Butt, Z.; Rivera, A.S.; Chillo, P.; Siril, H.; Hirschhorn, L.R.; Feinstein, M.J.; Hawkins, C. Ideal Cardiovascular Health: Distribution, Determinants and Relationship with Health Status among People Living with HIV in Urban Tanzania. Glob. Heart 2022, 17, 74. [Google Scholar] [CrossRef]
- Xu, Y.; Chen, X.; Wang, K. Global prevalence of hypertension among people living with HIV: A systematic review and meta-analysis. J. Am. Soc. Hypertens. 2017, 11, 530–540. [Google Scholar] [CrossRef]
- Daultrey, H.; Youseff, E.; Wright, J.; Davies, K.; Chakera, A.J.; Levett, T. The investigation of diabetes in people living with HIV: A systematic review. Diabet. Med. 2021, 38, e14454. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Romieu, A.C.; Garg, S.; Rosenberg, E.S.; Thompson-Paul, A.M.; Skarbinski, J. Is diabetes prevalence higher among HIV-infected individuals compared with the general population? Evidence from MMP and NHANES 2009–2010. BMJ Open Diabetes Res. Care 2017, 5, 304. [Google Scholar] [CrossRef] [PubMed]
- Kagaruki, G.B.; Mayige, M.T.; Ngadaya, E.S.; Kimaro, G.D.; Kalinga, A.K.; Kilale, A.M.; Kahwa, A.M.; Materu, G.S.; Mfinanga, S.G. Magnitude and risk factors of non-communicable diseases among people living with HIV in Tanzania: A cross sectional study from Mbeya and Dar es Salaam regions. BMC Public Health 2014, 14, 904. [Google Scholar] [CrossRef] [PubMed]
- Kagaruki, G.; Kimaro, G.; Mweya, C.; Kilale, A.; Mrisho, R.; Shao, A.; Kalinga, A.K.; Kahwa, A.M.; Ngadaya, E.S.; Materu, G.S.; et al. Prevalence and Risk Factors of Metabolic Syndrome among Individuals Living with HIV and Receiving Antiretroviral Treatment in Tanzania. Br. J. Med. Med. Res. 2015, 5, 1317–1327. [Google Scholar] [CrossRef]
- Mlay, M.; Bakari, M. The prevalence of HIV among patients admitted with stroke at the Muhimbili National Hospital, Dar es Salaam, Tanzania. Tanzan. J. Health Res. 2010, 12, 105–113. [Google Scholar] [CrossRef]
- Wu, H.; Larsen, C.P.; Hernandez-Arroyo, C.F.; Mohamed, M.M.B.; Caza, T.; Sharshir, M.; Chughtai, A.; Xie, L.; Gimenez, J.M.; Sandow, T.A.; et al. AKI and collapsing glomerulopathy associated with COVID-19 and apol1 high-risk genotype. J. Am. Soc. Nephrol. 2020, 31, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.C.; Coresh, J.; Fornage, M.; Astor, B.C.; Grams, M.; Franceschini, N.; Boerwinkle, E.; Parekh, R.S.; Kao, W.H.L. APOL1 variants associate with increased risk of CKD among African Americans. J. Am. Soc. Nephrol. 2013, 24, 1484–1491. [Google Scholar] [CrossRef]
- Weldegiorgis, M.; Woodward, M. The impact of hypertension on chronic kidney disease and end-stage renal disease is greater in men than women: A systematic review and meta-analysis. BMC Nephrol. 2020, 21, 506, Erratum in BMC Nephrol. 2020, 21, 545. . [Google Scholar]
- Islam, F.; Wu, J.; Jansson, J.; Wilson, D. Relative risk of cardiovascular disease among people living with HIV: A systematic review and meta-analysis. HIV Med. 2012, 13, 453–468. [Google Scholar] [CrossRef]
- NACP. National Guidelines for the Management of HIV and AIDS; Ministry of Health, Community Development, Gender Eac; NACP: Dodoma, Tanzania, 2019. [Google Scholar]
- Kidney International Supplements. Official Journal of the international Society of nephrology KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. IFAC Proc. Vol. IFAC-Pap. 2013, 3, 30–130. [Google Scholar]
- Stevens, L.A.; Claybon, M.A.; Schmid, C.H.; Chen, J.; Horio, M.; Imai, E.; Nelson, R.G.; Van Deventer, M.; Wang, H.-Y.; Zuo, L.; et al. Evaluation of the CKD-EPI Equation in Multiple Races and Ethnicities. Kidney Int. 2011, 79, 555. [Google Scholar] [CrossRef]
- Uppal, P.; Golden, B.L.; Panicker, A.; Khan, O.A.; Burday, M.J. The Case Against Race-Based GFR. Del. J. Public. Health 2022, 8, 86. [Google Scholar] [CrossRef]
- Rungkitwattanakul, D.; Chaijamorn, W.; Han, E.; Aldhaeefi, M. Kidney Function Assessment in African American Patients: A Narrative Review for Pharmacists. Pharm. J. Pharm. Educ. Pract. 2022, 10, 65. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance; WHO Global Report; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef]
- Tsur, A.M.; Akavian, I.; Derazne, E.; Tzur, D.; Vivante, A.; Grossman, E.; Rotem, R.S.; Fishman, B.; Afek, A.; Coresh, J.; et al. Adolescent Blood Pressure and the Risk for Early Kidney Damage in Young Adulthood. Hypertension 2022, 79, 974–983. [Google Scholar] [CrossRef] [PubMed]
- Dungan, K.M.; Braithwaite, S.S.; Preiser, J.C. Stress hyperglycaemia. Lancet 2009, 373, 1798–1807. [Google Scholar] [CrossRef] [PubMed]
- Pasternak RC 2001 National Cholesterol Education Program (NCEP) guidelines on the detection, evaluation and treatment of elevated cholesterol in adults: Adult treatment panel III (ATP III). ACC Curr. J. Rev. 2002, 11, 37–45. [CrossRef]
- Patel, P.; Rose, C.E.; Collins, P.Y.; Nuche-Berenguer, B.; Sahasrabuddhe, V.V.; Peprah, E.; Vorkoper, S.; Pastakia, S.D.; Rausch, D.; Levitt, N.S.; et al. Noncommunicable diseases among HIV-infected persons in low-income and middle-income countries: A systematic review and meta-analysis HHS Public Access. AIDS 2018, 32, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Fiseha, T.; Alemu, W.; Dereje, H.; Tamir Id, Z.; Gebreweld, A. Prevalence of Dyslipidaemia among HIV-Infected Patients Receiving Combination Antiretroviral Therapy in North Shewa, Ethiopia. PLoS ONE 2021, 16, e0250328. [Google Scholar] [CrossRef] [PubMed]
- Sowden, S.; Matłosz, B.; Skrzat-Klapaczy, A.; Antoniak, S.; Balayan, T.; Begovac, J.; Gusev, D.; Jevtovic, D.; Jilich, D.; Aimla, K.; et al. Chronic Kidney Disease and Nephrology Care in People Living with HIV in Central/Eastern Europe and Neighbouring Countries-Cross-Sectional Analysis from the ECEE Network. Int. J. Environ. Res. Public Health 2022, 19, 12554. [Google Scholar]
- Tanuma, J.; Jiamsakul, A.; Makane, A.; Avihingsanon, A.; Ng, O.T.; Kiertiburanakul, S.; Chaiwarith, R.; Kumarasamy, N.; Van Nguyen, K.; Pham, T.T.; et al. Renal Dysfunction during Tenofovir Use in a Regional Cohort of HIV-Infected Individuals in the Asia-Pacific. PLoS ONE 2016, 11, e0161562. [Google Scholar] [CrossRef]
- Zhao, N.; Ditan, B.; Xiang, P.; Zeng, Z.; Liang, H.; Wang, F.; Xiao, J.; Yang, D.; Chen, M.; Gao, G. Prevalence and Risk Factors for Kidney Disease in Chinese HIV-Infected Patients: A Cross-Sectional Study. 2022. Available online: https://doi.org/10.21203/rs.3.rs-1383158/v1 (accessed on 20 May 2020).
- Kim, E.J.; Ahn, J.Y.; Kim, Y.J.; Wie, S.H.; Park, D.W.; Song, J.Y.; Choi, H.J.; Chang, H.-H.; Choi, B.Y.; Choi, Y.; et al. The Prevalence and Risk Factors of Renal Insufficiency among Korean HIV-Infected Patients: The Korea HIV/AIDS Cohort Study. Infect. Chemother. 2017, 49, 194. [Google Scholar] [CrossRef]
- Diana, N.E.; Naicker, S. Update on current management of chronic kidney disease in patients with HIV infection. Int. J. Nephrol. Renov. Dis. 2016, 9, 223–234. [Google Scholar]
- Wyatt, C.M.; Klotman, P.E. HIV-1 and HIV-associated nephropathy 25 years later. Clin. J. Am. Soc. Nephrol. 2007, 2 (Suppl. S1), 20–24. [Google Scholar] [CrossRef]
- Kudose, S.; Santoriello, D.; Bomback, A.S.; Stokes, M.B.; Batal, I.; Markowitz, G.S.; Wyatt, C.M.; D’Agati, V.D. The spectrum of kidney biopsy findings in HIV-infected patients in the modern era. Kidney Int. 2020, 97, 1006–1016. [Google Scholar] [CrossRef]
- Wever, K.; Van Agtmael, M.A.; Carr, A. Incomplete reversibility of tenofovir-related renal toxicity in HIV-infected men. J. Acquir. Immune Defic. Syndr. 2010, 55, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Quesada, P.R.; Esteban, L.L.; García, J.R.; Sánchez, R.V.; García, T.M.; Alonso-Vega, G.G.; Ferrández, J.S.R. Incidence and risk factors for tenofovir-associated renal toxicity in HIV-infected patients. Int. J. Clin. Pharm. 2015, 37, 865–872. [Google Scholar] [CrossRef]
- Hamid, S.; Groot, W.; Pavlova, M. Trends in cardiovascular diseases and associated risks in sub-Saharan Africa: A review of the evidence for Ghana, Nigeria, South Africa, Sudan and Tanzania. Aging Male 2019, 22, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Haruna, T.; Somba, M.; Siril, H.; Mahiti, G.; August, F.; Minja, A.; Urassa, D.; Tarimo, E.; Mugusi, F. Factors hindering integration of care for non-communicable diseases within HIV care services in Dar es Salaam, Tanzania: The perspectives of health workers and people living with HIV. PLoS ONE 2021, 16, e0254436. [Google Scholar] [CrossRef] [PubMed]
- Hontelez, J.A.C.; De Vlas, S.J.; Baltussen, R.; Newell, M.L.; Bakker, R.; Tanser, F.; Lurie, M.; Bärnighausen, T. The impact of antiretroviral treatment on the age composition of the HIV epidemic in sub-Saharan Africa. AIDS 2012, 26, S19–S30. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Community Development, Gender E and Chidren. Strategic and Action Plan for the Prevention and Control of Non Communicable Diseases in Tanzania 2016–2020. Strategic and Action Plan 2016–2020; Ministry of Health, Community Development, Gender E and Children: Dar el Salaam, Tanzania, 2016; pp. 1–128. [Google Scholar]
- Lee, K.; Kim, J. Estimated glomerular filtration rate and albuminuria in Korean population evaluated for cardiovascular risk. Int. Urol. Nephrol. 2016, 48, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, W.; De Bacquer, D.; Verbeke, F.; Delanghe, J.; Lameire, N.; Vanholder, R. The glomerular filtration rate in an apparently healthy population and its relation with cardiovascular mortality during 10 years. Eur. Heart J. 2007, 28, 478–483. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Renal Insufficiency (eGFR < 60 mL/min/1.73 m2) | |||
|---|---|---|---|---|
| Total (N = 450) | Yes (n = 34) | No (n = 416) | p-Value | |
| Demographics | ||||
| n (%) a | n (%) b | n (%) b | ||
| Age (in years) | ||||
| Below 50 | 324 (72.0) | 8 (2.5) | 316 (97.5) | Ref. |
| 50 and above | 126 (28.0) | 26 (20.6) | 100 (79.4) | <0.001 |
| Sex | ||||
| Female | 332 (73.8) | 20 (6) | 312 (94) | Ref. |
| Male | 118 (26.2) | 14 (11.9) | 104 (88.1) | 0.03 |
| Health insurance status | ||||
| No | 383 (85.1) | 26 (6.8) | 357 (93.2) | Ref. |
| Yes | 67 (14.9) | 8 (11.9) | 59 (88.1) | 0.15 |
| Clinical characteristics | ||||
| BP levels (mm/Hg) * | ||||
| Normal (BP < 120/80) | 206 (45.8) | 9 (4.4) | 197 (95.6) | Ref. |
| Elevated (BP 120–129/<80) | 127 (28.2) | 7 (5.5) | 120 (94.5) | 0.64 |
| High (BP ≥ 130/80) or on antihypertensive therapy | 117 (26.0) | 18 (15.4) | 99 (84.6) | 0.001 |
| Diabetes (RBG ≥ 11.1 mmol/L) or on antidiabetic therapy * | ||||
| No | 437 (97.1) | 32 (7.32) | 405 (92.7) | Ref. |
| Yes | 13 (2.9) | 2 (15.4) | 11 (84.6) | 0.28 |
| Total Cholesterol (mmol/L) | ||||
| <5.2 | 376 (84) | 20 (5.3) | 356 (94.7) | Ref. |
| ≥5.2 | 74 (16) | 14 (18.9) | 60 (81.1) | <0.001 |
| Triglycerides (mmol/L) | ||||
| <1.7 | 373 (82.8) | 21 (5.6) | 352 (94.4) | Ref. |
| ≥1.7 | 77 (17) | 13 (16.9) | 64 (83.1) | 0.001 |
| LDL-C (mmol/L) | ||||
| <3.4 | 380 (84) | 21 (5.5) | 359 (94.5) | Ref. |
| ≥3.4 | 70 (16) | 13 (18.6) | 57 (81.4) | <0.001 |
| HDL-C (mmol/L) | ||||
| ≥1.0 among male and ≥1.3 among Female | 268 (59.6) | 19 (7) | 249 (93) | Ref. |
| <1.0 among Male and <1.3 among Female | 182 (40.4) | 15 (8.2) | 167 (91.8) | 0.65 |
| Dyslipidemia | ||||
| No | 201 (45) | 9 (4.5) | 192 (95.5) | Ref. |
| Yes | 249 (55) | 25 (10) | 224 (90) | 0.03 |
| BMI (kg/m2) | ||||
| Normal weight (<25) | 228 (50.7) | 17 (7.5) | 211 (92.5) | Ref. |
| Overweight (25–30) | 114 (25.3) | 8 (7) | 106 (93) | 0.88 |
| Obese (≥30) | 108 (24.0) | 9 (8.3) | 99 (91.7) | 0.78 |
| Smoking status | ||||
| No | 377 (83.8) | 27 (7.2) | 350 (92.8) | Ref. |
| Yes | 73 (16.2) | 7 (9.6) | 66 (90.4) | 0.47 |
| Alcohol use | ||||
| No | 338 (75.1) | 24 (7.1) | 314 (92.9) | Ref. |
| Yes | 112 (24.9) | 10 (8.9) | 102 (91.1) | 0.53 |
| HIV infection related characteristics | ||||
| Years lived with HIV infection (median, IQR) in years | 6 (3–11) | 6.5 (3–11) | 6 (3–11) | 0.50 |
| Duration on ART (median, IQR) in years | 5 (3–10) | 6 (3–10) | 5 (3–10) | 0.49 |
| ART regimen | ||||
| TDF + 3TC + DTG (TLD) | 401 (89.1) | 32 (8) | 369 (92) | Ref. |
| Other regimens | 49 (10.9) | 2 (4) | 47 (96) | 0.33 |
| HIV VL load | ||||
| ≤50 copies | 394 (87.6) | 32 (8.1) | 362 (91.9) | Ref. |
| >50 copies | 56 (12.4) | 2 (3.6) | 54 (96.4) | 0.23 |
| Characteristic | Crude OR (95% CI) (N = 444) | p-Value | Adjusted OR (95% CI) (N = 444) | p-Value |
|---|---|---|---|---|
| Age (in years) | 1.09 (1.07–1.12) | <0.001 | 1.09 (1.07–1.12) | <0.001 |
| Sex | ||||
| Female | Ref. | Ref. | ||
| Male | 1.51 (0.99–2.30) | 0.05 | 1.25 (0.74–2.10) | 0.35 |
| BP levels (mmHg) | ||||
| Normal (BP < 120/80) | Ref. | Ref. | ||
| Elevated (BP 120–129/<80) | 1.04 (0.65–1.65) | 0.87 | 0.93 (0.55–1.55) | 0.25 |
| High (BP ≥ 130/80) or on antihypertensive therapy | 2.18 (1.38–3.44) | <0.001 | 1.28 (0.77–2.13) | 0.31 |
| Dyslipidemia | ||||
| No | Ref. | Ref. | ||
| Yes | 2.18 (1.39–3.42) | <0.001 | 1.55 (0.94–2.54) | 0.15 |
| BMI (kg/m2) | 0.99 (0.96–1.00) | 0.29 | 0.98 (0.94–1.00) | 0.24 |
| Smoking status | ||||
| No | Ref. | |||
| Yes | 0.92 (0.54–1.53) | 0.74 | 0.62 (0.32–1.17) | 0.15 |
| Alcohol use | ||||
| No | Ref. | |||
| Yes | 1.16 (0.75–1.78) | 0.50 | 1.56 (0.95–2.54) | 0.06 |
| Years lived with HIV infection (in years) | 1.03 (0.99–1.07) | 0.21 | 0.98 (0.94–1.03) | 0.33 |
| ART regimen | ||||
| TDF + 3TC + DTG (TLD) | Ref. | Ref. | ||
| Other regimens | 0.64 (0.33–1.20) | 0.18 | 0.78 (0.36–1.59) | 0.53 |
| HIV VL (copies/mL) | ||||
| ≤50 copies | Ref. | Ref. | ||
| >50 copies | 0.63 (0.34–1.14) | 0.14 | 0.63 (0.31–1.22) | 0.19 |
| Facility | ||||
| Site 1 | 1.31 (0.72–2.41) | 0.38 | ||
| Site 2 | Ref. | |||
| Site 3 | 1.58 (0.88–2.85) | 0.13 | ||
| Site 4 | 1.19 (0.65–2.20) | 0.57 | ||
| Site 5 | 1.03 (0.52–2.02) | 0.92 | ||
| Site 6 | 0.92 (0.44–1.86) | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottaru, T.A.; Kwesigabo, G.P.; Butt, Z.; Caputo, M.; Chillo, P.; Siril, H.; Hirschhorn, L.R.; Hawkins, C. Prevalence and Risk Factors for Renal Insufficiency among Adults Living with HIV in Tanzania: Results from a Cross-Sectional Study in 2020–2021. Healthcare 2024, 12, 657. https://doi.org/10.3390/healthcare12060657
Ottaru TA, Kwesigabo GP, Butt Z, Caputo M, Chillo P, Siril H, Hirschhorn LR, Hawkins C. Prevalence and Risk Factors for Renal Insufficiency among Adults Living with HIV in Tanzania: Results from a Cross-Sectional Study in 2020–2021. Healthcare. 2024; 12(6):657. https://doi.org/10.3390/healthcare12060657
Chicago/Turabian StyleOttaru, Theresia A., Gideon P. Kwesigabo, Zeeshan Butt, Matthew Caputo, Pilly Chillo, Hellen Siril, Lisa R. Hirschhorn, and Claudia Hawkins. 2024. "Prevalence and Risk Factors for Renal Insufficiency among Adults Living with HIV in Tanzania: Results from a Cross-Sectional Study in 2020–2021" Healthcare 12, no. 6: 657. https://doi.org/10.3390/healthcare12060657