
Living with Multimorbidity through Time: A Meta-Synthesis of Qualitative Longitudinal Evidence


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Literature Search
2.3. Eligibility Criteria and Study Selection
2.4. Quality Appraisal
2.5. Data Extraction
2.6. Data Analysis
3. Results
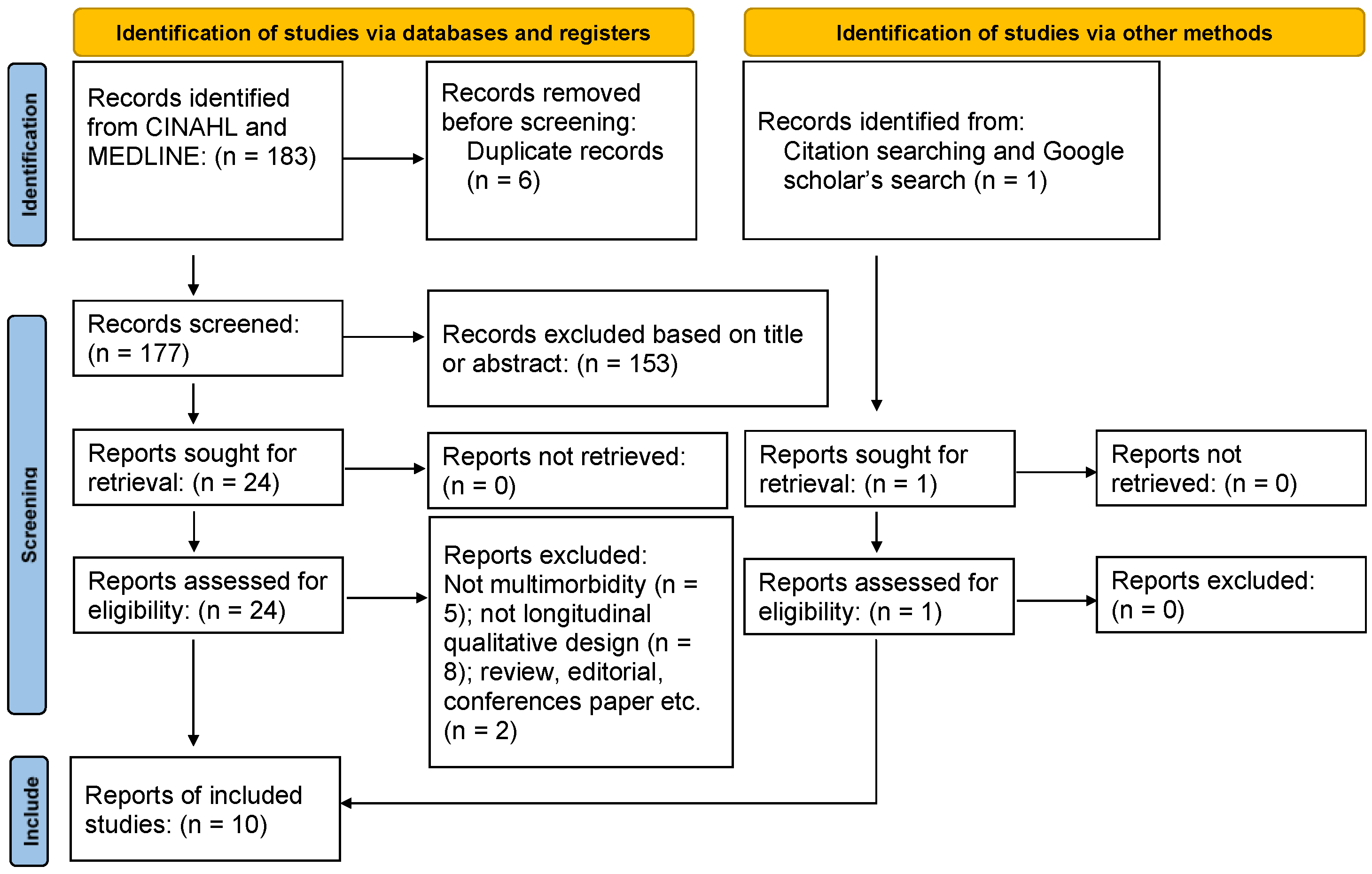
3.1. Search Results
3.2. Quality Appraisal
3.3. Overview of the Included Studies
3.4. Findings of the Thematic Analysis
3.4.1. Perceiving Multimorbidity
3.4.2. Managing Chronic Conditions
3.4.3. Emotional Struggles in Everyday Life with Multimorbidity
3.4.4. Interactions with the Healthcare System and Healthcare Professionals
3.4.5. Family Support
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Skou, S.T.; Mair, F.S.; Fortin, M.; Guthrie, B.; Nunes, B.P.; Miranda, J.J.; Boyd, C.M.; Pati, S.; Mtenga, S.; Smith, S.M. Multimorbidity. Nat. Rev. Dis. Primers 2022, 8, 48. [Google Scholar] [CrossRef]
- Chowdhury, S.R.; Das, D.C.; Sunna, T.C.; Beyene, J.; Hossain, A. Global and regional prevalence of multimorbidity in the adult population in community settings: A systematic review and meta-analysis. eClinicalMedicine 2023, 57, 101860. [Google Scholar] [CrossRef]
- Palladino, R.; Pennino, F.; Finbarr, M.; Millett, C.; Triassi, M. Multimorbidity and health outcomes in older adults in ten European health systems, 2006–2015. Health Aff. 2019, 38, 613–623. [Google Scholar] [CrossRef]
- Pedersen, A.F.; Nørøxe, K.B.; Vedsted, P. Influence of patient multimorbidity on GP burnout: A survey and register-based study in Danish general practice. Br. J. Gen. Pract. 2020, 70, e95–e101. [Google Scholar] [CrossRef]
- Soley-Bori, M.; Ashworth, M.; Bisquera, A.; Dodhia, H.; Lynch, R.; Wang, Y.; Fox-Rushby, J. Impact of multimorbidity on healthcare costs and utilisation: A systematic review of the UK literature. Br. J. Gen. Pract. 2021, 71, e39–e46. [Google Scholar] [CrossRef] [PubMed]
- Damarell, R.A.; Morgan, D.D.; Tieman, J.J. General practitioner strategies for managing patients with multimorbidity: A systematic review and thematic synthesis of qualitative research. BMC Fam. Pract. 2020, 21, 131. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Hynes, L.; Murphy, A.W.; Molloy, G.J. ‘Just keep taking them, keep hoping they’ll work’: A qualitative study of adhering to medications for multimorbidity. Br. J. Health Psychol. 2022, 27, 691–715. [Google Scholar] [CrossRef] [PubMed]
- Corbett, T.; Cummings, A.; Calman, L.; Farrington, N.; Fenerty, V.; Foster, C.; Richardson, A.; Wiseman, T.; Bridges, J. Self-management in older people living with cancer and multi-morbidity: A systematic review and synthesis of qualitative studies. Psychooncology 2020, 29, 1452–1463. [Google Scholar] [CrossRef]
- Van der Aa, M.J.; van den Broeke, J.R.; Stronks, K.; Plochg, T. Patients with multimorbidity and their experiences with the healthcare process: A scoping review. J. Comorbidity 2017, 7, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Rosbach, M.; Andersen, J.S. Patient-experienced burden of treatment in patients with multimorbidity—A systematic review of qualitative data. PLoS ONE 2017, 12, e0179916. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.-W.; Kim, E.Y.; Son, Y.-J. Home-dwelling older adults’ experiences of living with both frailty and multimorbidity: A meta-ethnography. Geriatr. Nurs. 2022, 47, 191–200. [Google Scholar] [CrossRef]
- Whitehead, L.; Palamara, P.; Allen, J.; Boak, J.; Quinn, R.; George, C. Nurses’ perceptions and beliefs related to the care of adults living with multimorbidity: A systematic qualitative review. J. Clin. Nurs. 2022, 31, 2716–2736. [Google Scholar] [CrossRef]
- Audulv, Å.; Hall, E.O.C.; Kneck, Å.; Westergren, T.; Fegran, L.; Pedersen, M.K.; Aagaard, H.; Dam, K.L.; Ludvigsen, M.S. Qualitative longitudinal research in health research: A method study. BMC Med. Res. Methodol. 2022, 22, 255. [Google Scholar] [CrossRef]
- Finlayson, K.W.; Dixon, A. Qualitative meta-synthesis: A guide for the novice. Nurse Res. 2008, 15, 59–71. [Google Scholar] [CrossRef]
- Lachal, J.; Revah-Levy, A.; Orri, M.; Moro, M.R. Metasynthesis: An Original Method to Synthesize Qualitative Literature in Psychiatry. Front. Psychiatry 2017, 8, 269. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Larkin, J.; Foley, L.; Smith, S.M.; Harrington, P.; Clyne, B. The experience of financial burden for people with multimorbidity: A systematic review of qualitative research. Health Expect. 2021, 24, 282–295. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. CASP Qualitative Studies Checklist. Available online: https://casp-uk.net/checklists/casp-qualitative-studies-checklist-fillable.pdf (accessed on 30 October 2023).
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- Rampin, R.; Rampin, V. Taguette: Open-source qualitative data analysis. J. Open Source Softw. 2021, 6, 3522. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.D.; Martin, L.A.; Moye, J.; Karel, M.J. Health Values and Treatment Goals of Older, Multimorbid Adults Facing Life-Threatening Illness. J. Am. Geriatr. Soc. 2016, 64, 625–631. [Google Scholar] [CrossRef]
- Francis, H.; Carryer, J.; Wilkinson, J. Self-management support? Listening to people with complex co-morbidities. Chronic Illn. 2020, 16, 161–172. [Google Scholar] [CrossRef]
- Collier, A.; Balmer, D.; Dai, L.; Hikaka, J.; Bloomfield, K.; Boyd, M. Older people, medication safety, and the role of the community pharmacist: A longitudinal ethnographic study. J. Pharm. Pract. Res. 2023, 53, 18–25. [Google Scholar] [CrossRef]
- Brandberg, C.; Ekstedt, M.; Flink, M. Self-management challenges following hospital discharge for patients with multimorbidity: A longitudinal qualitative study of a motivational interviewing intervention. BMJ Open 2021, 11, e046896. [Google Scholar] [CrossRef]
- Bravo, R.L.; Gutiérrez, Á.; Levy-Storms, L.F. Patient-Provider Relationships in an All-Inclusive Specialized Geriatric Program: A Longitudinal Qualitative Study among Older Foreign-Born Latinos with Multimorbidities. J. Elder Policy Vol. 2022, 2, 191–214. [Google Scholar] [CrossRef]
- Morris, R.L.; Sanders, C.; Kennedy, A.P.; Rogers, A. Shifting priorities in multimorbidity: A longitudinal qualitative study of patient’s prioritization of multiple conditions. Chronic Illn. 2011, 7, 147–161. [Google Scholar] [CrossRef]
- Mason, B.; Nanton, V.; Epiphaniou, E.; Murray, S.A.; Donaldson, A.; Shipman, C.; Daveson, B.A.; Harding, R.; Higginson, I.J.; Munday, D.; et al. ‘My body’s falling apart.’ Understanding the experiences of patients with advanced multimorbidity to improve care: Serial interviews with patients and carers. BMJ Support. Palliat. Care 2016, 6, 60–65. [Google Scholar] [CrossRef]
- Hays, R.; Daker-White, G.; Esmail, A.; Barlow, W.; Minor, B.; Brown, B.; Blakeman, T.; Sanders, C.; Bower, P. Threats to patient safety in primary care reported by older people with multimorbidity: Baseline findings from a longitudinal qualitative study and implications for intervention. BMC Health Serv. Res. 2017, 17, 754. [Google Scholar] [CrossRef]
- Daker-White, G.; Hays, R.; Blakeman, T.; Croke, S.; Brown, B.; Esmail, A.; Bower, P. Safety work and risk management as burdens of treatment in primary care: Insights from a focused ethnographic study of patients with multimorbidity. BMC Fam. Pract. 2018, 19, 155. [Google Scholar] [CrossRef] [PubMed]
- Porter, T.; Ong, B.N.; Sanders, T. Living with multimorbidity? The lived experience of multiple chronic conditions in later life. Health Interdiscip. J. Soc. Study Health Illn. Med. 2020, 24, 701–718. [Google Scholar] [CrossRef]
- Bower, P.; Harkness, E.; Macdonald, W.; Coventry, P.; Bundy, C.; Moss-Morris, R. Illness representations in patients with multimorbid long-term conditions: Qualitative study. Psychol. Health 2012, 27, 1211–1226. [Google Scholar] [CrossRef]
- Van Merode, T.; Van De Ven, K.; Van Den Akker, M. Patients with multimorbidity and their treatment burden in different daily life domains: A qualitative study in primary care in the Netherlands and Belgium. J. Comorbidity 2018, 8, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Marthias, T.; Anindya, K.; Ng, N.; McPake, B.; Atun, R.; Arfyanto, H.; Hulse, E.S.; Zhao, Y.; Jusril, H.; Pan, T. Impact of non-communicable disease multimorbidity on health service use, catastrophic health expenditure and productivity loss in Indonesia: A population-based panel data analysis study. BMJ Open 2021, 11, e041870. [Google Scholar] [CrossRef]
- St John, P.D.; Menec, V.; Tyas, S.L.; Tate, R.; Griffith, L. Multimorbidity in Canadians living in the community: Results from the Canadian Longitudinal Study of Aging. Can. Fam. Physician 2021, 67, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.A.; Cahir, C.; Bennett, K.E. Longitudinal medication adherence in older adults with multimorbidity and association with health care utilization: Results from the Irish longitudinal study on ageing. Ann. Pharmacother. 2021, 55, 5–14. [Google Scholar] [CrossRef]
- Zhao, Y.W.; Haregu, T.N.; He, L.; Lu, S.; Katar, A.; Wang, H.; Yao, Z.; Zhang, L. The effect of multimorbidity on functional limitations and depression amongst middle-aged and older population in China: A nationwide longitudinal study. Age Ageing 2021, 50, 190–197. [Google Scholar] [CrossRef]
- Bankole, A.O.; Jiwani, R.B.; Avorgbedor, F.; Wang, J.; Osokpo, O.H.; Gill, S.L.; Braden, C.J. Exploring illness perceptions of multimorbidity among community-dwelling older adults: A mixed methods study. Aging Health Res. 2023, 3, 100158. [Google Scholar] [CrossRef]
- Cheraghi-Sohi, S.; Morden, A.; Bower, P.; Kennedy, A.; Rogers, A.; Richardson, J.; Sanders, T.; Stevenson, F.; Ong, B.N. Exploring patient priorities among long-term conditions in multimorbidity: A qualitative secondary analysis. SAGE Open Med. 2013, 1, 2050312113503955. [Google Scholar] [CrossRef]
- Sathanapally, H.; Sidhu, M.; Fahami, R.; Gillies, C.; Kadam, U.; Davies, M.J.; Khunti, K.; Seidu, S. Priorities of patients with multimorbidity and of clinicians regarding treatment and health outcomes: A systematic mixed studies review. BMJ Open 2020, 10, e033445. [Google Scholar] [CrossRef]
- Cheng, C.; Inder, K.; Chan, S.W. Patients’ experiences of coping with multiple chronic conditions: A meta-ethnography of qualitative work. Int. J. Ment. Health Nurs. 2019, 28, 54–70. [Google Scholar] [CrossRef] [PubMed]
- Horn, A.B.; Boettcher, V.S.; Holzer, B.M.; Siebenhuener, K.; Maercker, A.; Battegay, E.; Zimmerli, L. Couples Adjusting to Multimorbidity: A Dyadic Study on Disclosure and Adjustment Disorder Symptoms. Front. Psychol. 2019, 10, 2499. [Google Scholar] [CrossRef]
- Ogedegbe, G.O.; Boutin-Foster, C.; Wells, M.T.; Allegrante, J.P.; Isen, A.M.; Jobe, J.B.; Charlson, M.E. A randomized controlled trial of positive-affect intervention and medication adherence in hypertensive African Americans. Arch. Intern. Med. 2012, 172, 322–326. [Google Scholar] [CrossRef]
- Peterson, J.C.; Charlson, M.E.; Hoffman, Z.; Wells, M.T.; Wong, S.C.; Hollenberg, J.P.; Jobe, J.B.; Boschert, K.A.; Isen, A.M.; Allegrante, J.P. A randomized controlled trial of positive-affect induction to promote physical activity after percutaneous coronary intervention. Arch. Intern. Med. 2012, 172, 329–336. [Google Scholar] [CrossRef]
- Sabouri, F.; Rambod, M.; Khademian, Z. The effect of positive thinking training on hope and adherence to treatment in hemodialysis patients: A randomized controlled trial. BMC Psychol. 2023, 11, 6. [Google Scholar] [CrossRef]
- Kangovi, S.; Mitra, N.; Smith, R.A.; Kulkarni, R.; Turr, L.; Huo, H.; Glanz, K.; Grande, D.; Long, J.A. Decision-making and goal-setting in chronic disease management: Baseline findings of a randomized controlled trial. Patient Educ. Couns. 2017, 100, 449–455. [Google Scholar] [CrossRef]
- O’Brien, R.; Wyke, S.; Watt, G.; Guthrie, B.; Mercer, S.W. The ‘everyday work’ of living with multimorbidity in socioeconomically deprived areas of Scotland. J. Comorb 2014, 4, 1–10. [Google Scholar] [CrossRef]
- Deatrick, J.A.; Knafl, K.A.; Murphy-Moore, C. Clarifying the concept of normalization. Image J. Nurs. Sch. 1999, 31, 209–214. [Google Scholar] [CrossRef]
- Benyamini, Y.; Gozlan, M.; Weissman, A. Normalization as a strategy for maintaining quality of life while coping with infertility in a pronatalist culture. Int. J. Behav. Med. 2017, 24, 871–879. [Google Scholar] [CrossRef]
- Milo, F.; Ranocchiari, S.; Lucidi, V.; Tabarini, P. Coping with cystic fibrosis: An analysis from the sibling’s point of view. Child Care Health Dev. 2021, 47, 825–833. [Google Scholar] [CrossRef]
- Rehm, R.S.; Franck, L.S. Long-term goals and normalization strategies of children and families affected by HIV/AIDS. Adv. Nurs. Sci. 2000, 23, 69–82. [Google Scholar] [CrossRef]
- Gerteis, M.; Edgman-Levitan, S.; Daley, J.; Delbanco, T.L. Through the Patient’s Eyes: Understanding and Promoting Patient-Centered Care. J. Healthc. Qual. 1997, 19, 43. [Google Scholar] [CrossRef]
- Kuipers, S.J.; Cramm, J.M.; Nieboer, A.P. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv. Res. 2019, 19, 13. [Google Scholar] [CrossRef]
- Kuipers, S.J.; Nieboer, A.P.; Cramm, J.M. Views of patients with multi-morbidity on what is important for patient-centered care in the primary care setting. BMC Fam. Pract. 2020, 21, 71. [Google Scholar] [CrossRef]
- Poitras, M.E.; Maltais, M.E.; Bestard-Denommé, L.; Stewart, M.; Fortin, M. What are the effective elements in patient-centered and multimorbidity care? A scoping review. BMC Health Serv. Res. 2018, 18, 446. [Google Scholar] [CrossRef]
- Stewart, M.; Brown, J.B.; Weston, W.; McWhinney, I.R.; McWilliam, C.L.; Freeman, T. Patient-Centered Medicine: Transforming the Clinical Method; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- The American Geriatrics Society Expert Panel on Person-Centered Care. Person-Centered Care: A Definition and Essential Elements. J. Am. Geriatr. Soc. 2016, 64, 15–18. [Google Scholar] [CrossRef]
- Agha, L.; Frandsen, B.; Rebitzer, J.B. Causes and Consequences of Fragmented Care Delivery: Theory, Evidence, and Public Policy; National Bureau of Economic Research: Cambridge, MA, USA, 2017. [Google Scholar]
- Joo, J.Y. Fragmented care and chronic illness patient outcomes: A systematic review. Nurs. Open 2023, 10, 3460–3473. [Google Scholar] [CrossRef]
- Prior, A.; Vestergaard, C.H.; Vedsted, P.; Smith, S.M.; Virgilsen, L.F.; Rasmussen, L.A.; Fenger-Grøn, M. Healthcare fragmentation, multimorbidity, potentially inappropriate medication, and mortality: A Danish nationwide cohort study. BMC Med. 2023, 21, 305. [Google Scholar] [CrossRef] [PubMed]
- Read, J.R.; Sharpe, L.; Modini, M.; Dear, B.F. Multimorbidity and depression: A systematic review and meta-analysis. J. Affect. Disord. 2017, 221, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Benkel, I.; Arnby, M.; Molander, U. Living with a chronic disease: A quantitative study of the views of patients with a chronic disease on the change in their life situation. SAGE Open Med. 2020, 8, 2050312120910350. [Google Scholar] [CrossRef] [PubMed]
- Olsman, E.; Leget, C.; Duggleby, W.; Willems, D. A singing choir: Understanding the dynamics of hope, hopelessness, and despair in palliative care patients. A longitudinal qualitative study. Palliat. Support. Care 2015, 13, 1643–1650. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.L.; Bergeron, C.D.; Adler, C.H.; Patel, A.; Ahn, S.; Towne, S.D.; Bien, M.; Ory, M.G. Factors associated with healthcare-related frustrations among adults with chronic conditions. Patient Educ. Couns. 2017, 100, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Triolo, F.; Harber-Aschan, L.; Belvederi Murri, M.; Calderón-Larrañaga, A.; Vetrano, D.L.; Sjöberg, L.; Marengoni, A.; Dekhtyar, S. The complex interplay between depression and multimorbidity in late life: Risks and pathways. Mech. Ageing Dev. 2020, 192, 111383. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) & Country | Aim | Design | Sample | Data Collection Process | Data Analysis |
|---|---|---|---|---|---|
| Morris et al. (2011), UK [28] | To explore factors that impact self-management priorities for people with multimorbidity and their changes. | Longitudinal qualitative study | Purposive sampling. 21 participants (Female: 11) with multimorbidity. Ages 36–84 years. Common diseases were diabetes and COPD. | Face-to-face interviews, telephone follow-ups, and final face-to-face interviews a year later | Semi-structured and narrative approach |
| Mason et al. (2016), UK [29] | To explore the experiences and perceptions of people with multimorbidity. | Serial multi-perspective interviews | Purposive sampling. 37 participants (Female: 14), mean age 76 years, range 55–92 years. Common diseases were heart, respiratory, liver, and renal failure, lung cancer, neurological conditions, and mild dementia. | Semi-structured serial interviews with people with multimorbidity and their family carers at 8–12 weekly intervals | Thematic analysis, cross-case analysis, and interpretive analysis |
| Naik et al. (2016), USA [23] | To explore health-related values concerning care in older adults with multimorbidity. | Qualitative component of a longitudinal mixed-methods study | 146 participants (Female: 3), 107 aged >60 years. (73.3%). Common diseases were diabetes mellitus, chronic pulmonary disease, peripheral vascular disease, and cerebrovascular disease. | Open-ended questions and interviews with 6-month intervals | Deductive (a priori) and inductive (emerging from the data) coding approaches |
| Hays et al. (2017), UK [30] | To explore threats to patient safety in older adults with multimorbidity. | Longitudinal qualitative study | Purposive sampling. 26 participants (Female: 15), mean age 76 years, range 66–87 years. Common diseases were painful and respiratory conditions, hypertension and coronary heart disease, thyroid and prostate disorders, diverticular and chronic kidney disease, diabetes, anxiety, stroke, psoriasis, and glaucoma. | In-depth semi-structured interviews | Thematic analysis with a framework approach |
| Daker-White et al. (2018), UK [31] | To explore safety issues in people with multimorbidity. | Ethnography and longitudinal qualitative study | Purposive sampling. 25 participants (Female: 14), all aged over 65 years. | Face-to-face interviews every 12 months observation, and field note material were also collected | Thematic analysis |
| Francis et al. (2020), New Zealand [24] | To explore experiences of long-term care in people with multimorbidity. | Qualitative, multiple cases | 16 participants (Female: 9), most aged 50–69 years (68.8%). Common diseases were diabetes, heart diseases, COPD, and hypertension. | Four weekly face-to-face semi-structured interviews | Narrative inquiry and thematic analysis |
| Porter et al. (2020), UK [32] | To explore lived experiences of multimorbidity from the point of view of patients. | Longitudinal qualitative study | Purposive sampling. 15 participants (Female: 8), all aged 65+ years. Common diseases were osteoarthritis and cardiovascular disease including hypertension, heart disease, and heart failure. | Two in-depth qualitative interviews from three to six months | Constructivist grounded theory |
| Brandberg et al. (2021), Sweden [26] | To explore self-management challenges in people with multimorbidity. | Longitudinal qualitative study | Purposive sampling. 16 participants (Female: 7), mean age 71 ± 10 years. Common diseases were congestive heart failure, COPD, hypertension, diabetes, renal failure, and anemia. | Four to five interview sessions per patient, seventy recorded sessions in total | Inductive qualitative content analysis and longitudinal analysis |
| Bravo et al. (2022), Canada [27] | To explore the experiences of patient–provider relationships among older foreign-born Latinos with multimorbidity. | Longitudinal qualitative study | Convenience sampling. 13 participants (Female: 10), mean age 75 years, range 65–85 years. Common diseases were unknown. | Three rounds of semi-structured in-depth qualitative interviews over nine months | Inductive approach |
| Collier et al. (2023), New Zealand [25] | To explore the experiences of older people with frailty, multimorbidity, and polypharmacy regarding the role of pharmacists. | Longitudinal ethnographic study | 20 participants, age range 68–89 years. Eight participants (Female: 6) followed up | Semi-structured interviews, observation field notes, and photographs | Iterative framework |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.; Christensen, M. Living with Multimorbidity through Time: A Meta-Synthesis of Qualitative Longitudinal Evidence. Healthcare 2024, 12, 446. https://doi.org/10.3390/healthcare12040446
Cheng C, Christensen M. Living with Multimorbidity through Time: A Meta-Synthesis of Qualitative Longitudinal Evidence. Healthcare. 2024; 12(4):446. https://doi.org/10.3390/healthcare12040446
Chicago/Turabian StyleCheng, Cheng, and Martin Christensen. 2024. "Living with Multimorbidity through Time: A Meta-Synthesis of Qualitative Longitudinal Evidence" Healthcare 12, no. 4: 446. https://doi.org/10.3390/healthcare12040446