
Nursing Interventions for Client and Family Training in the Proper Use of Noninvasive Ventilation in the Transition from Hospital to Community: A Scoping Review
 ,
,
Abstract
:1. Introduction
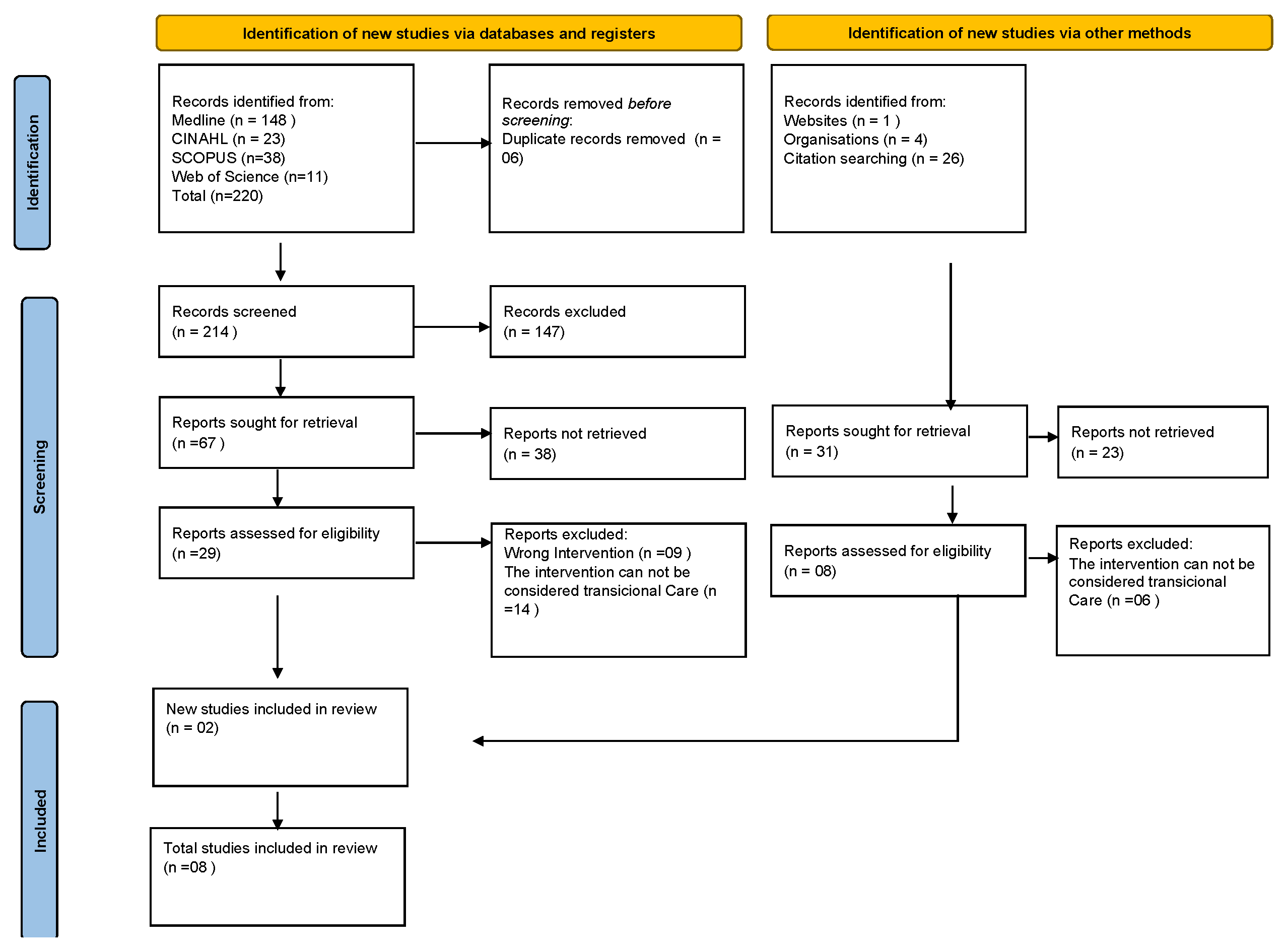
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Data Collection
2.4. Data Processing and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forum of International Respiratory Societies. The Global Impact of Respiratory Disease, 3rd ed.; European Respiratory Society. 2021. Available online: https://firsnet.org/images/publications/FIRS_Master_09202021.pdf (accessed on 22 September 2023).
- Park, S.C.; Kim, D.W.; Park, E.C.; Shin, C.S.; Rhee, C.K.; Kang, Y.A.; Kim, Y.S. Mortality of patients with chronic obstructive pulmonary disease: A nationwide populationbased cohort study. Korean J. Intern. Med. 2019, 34, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Le Bouar, G.; Boyer, D.; Artaud-Macari, E.; Molano, L.C.; Viacroze, C.; Cuvelier, A.; Patout, M. Noninvasive ventilation (NIV) adherence for chronic respiratory failure treatment. Eur. Respir. J. 2018, 52 (Suppl. S62), PA2376. [Google Scholar] [CrossRef]
- Gupta, S.; Ramasubban, S.; Dixit, S.; Mishra, R.; Zirpe, K.G.; Khilnani, G.C.; Khatib, K.I.; Dobariya, J.; Marwah, V.; Jog, S.A.; et al. ISCCM Guidelines for the Use of Non-invasive Ventilation in Acute Respiratory Failure in Adult ICUs. Indian J. Crit. Care Med. 2020, 24 (Suppl. S1), S61–S81. [Google Scholar] [CrossRef] [PubMed]
- Spurr, L. The treatment burden of long-term home noninvasive ventilation. Breathe 2021, 17, 200291. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.C.; Banham, S.; Elliott, M.; Kennedy, D.; Gelder, C.; Glossop, A.; Church, A.C.; Creagh-Brown, B.; Dodd, J.W.; Felton, T.; et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax 2016, 71, ii1–ii35. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.R. Noninvasive Ventilation for Acute Respiratory Failure. Respir. Care 2013, 58, 950–972. [Google Scholar] [CrossRef]
- Ferreira, S.; Nogueira, C.; Conde, S.; Taveira, N. Ventilação não-invasiva. Rev. Port. Pneumol. 2009, 15, 655–677. Available online: https://www.redalyc.org/pdf/1697/169718537006.pdf (accessed on 22 September 2023). [CrossRef]
- Pinto, C.; Sousa, P. Ventilação não invasiva: Uma revisão integrativa da literatura. In Construindo Conhecimento em Enfermagem à Pessoa em Situação Crítica; Dixe, L.M., Sousa, P., Gaspareiria, P., Eds.; Instituto Politécnico de Leiria: Leiria, Portugal, 2017; pp. 89–104. Available online: http://hdl.handle.net/10400.8/2882 (accessed on 22 May 2023).
- Ferreira, B.A.d.S.; Gomes, T.J.B.; Baixinho, C.R.S.L.; Ferreira, M.R. Transitional care to caregivers of dependent older people: An integrative literature review. Rev. Bras. Enferm. 2020, 73, e20200394. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Menezes, T.M.d.O.; de Oliveira, A.L.B.; Santos, L.B.; de Freitas, R.A.; Pedreira, L.C.; Veras, S.M.C.B. Hospital transition care for the elderly: An integrative review. Rev. Bras. Enferm. 2019, 72 (Suppl. S2), 294–301. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Raurell-Torredà, M.; Romero-Collado, A.; Rodríguez-Palma, M.; Farrés-Tarafa, M.; Martí, J.; Hurtado-Pardos, B.; Florencio, L.P.-S.; Saez-Paredes, P.; Esquinas, A. Prevención y tratamiento de las lesiones cutáneas asociadas a la ventilación mecánica no invasiva. Recomendaciones de expertos. Enferm Intensiva. 2017, 28, 31–41. [Google Scholar] [CrossRef]
- Rolfe, S. Non-invasive positive pressure ventilation in the home setting. Br. J. Community Nurs. 2019, 24, 102–109. [Google Scholar] [CrossRef]
- Jiang, W.P.; Wang, L.; Song, Y.L. Titration and follow-up for home noninvasive positive pressure ventilation in chronic obstructive pulmonary disease: The potential role of tele-monitoring and the Internet of things. Clin. Respir. J. 2021, 15, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Rio, A.S.P.C.; Ramos, F.A.M. Promotion the critically ill patient adaptation to noninvasive ventilation: An integrative literature review. BJHR 2022, 5, 21878–21899. [Google Scholar] [CrossRef]
- Jones, B.; James, P.; Vijayasiri, G.; Li, Y.; Bozaan, D.; Okammor, N.; Hendee, K.; Jenq, G. Patient Perspectives on Care Transitions From Hospital to Home. JAMA Netw. Open 2022, 5, e2210774. [Google Scholar] [CrossRef]
- Klingshirn, H.; Gerken, L.; Hofmann, K.; Heuschmann, P.U.; Haas, K.; Schutzmeier, M.; Brandstetter, L.; Ahnert, J.; Wurmb, T.; Kippnich, M.; et al. How to improve the quality of care for people on home mechanical ventilation from the perspective of healthcare professionals: A qualitative study. BMC Health Serv. Res. 2021, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, M.C.O. DPOC: Abordagem a 360º do Hospital para o Domicílio; Lusodidacta: Sintra, Portugal, 2021. [Google Scholar]
- Klingshirn, H.; Gerken, L.; Hofmann, K.; Heuschmann, P.U.; Haas, K.; Schutzmeier, M.; Brandstetter, L.; Wurmb, T.; Kippnich, M.; Reuschenbach, B. Comparing the quality of care for long-term ventilated individuals at home versus in shared living communities: A convergent parallel mixed-methods study. BMC Nurs. 2022, 21, 224. [Google Scholar] [CrossRef] [PubMed]
- Pierucci, P.; Portacci, A.; Carpagnano, G.E.; Banfi, P.; Crimi, C.; Misseri, G.; Gregoretti, C. The right interface for the right patient in noninvasive ventilation: A systematic review. Expert Rev. Respir. Med. 2022, 16, 931–944. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo Fernandes, A.F.; Romão da Veiga Branco, M.A. Interdependent nursing interventions as sensitive indicators of quality—Care in noninvasive mechanical ventilation. Millenium J. Educ. Technol. Health 2023, 2, e28233. [Google Scholar] [CrossRef]
- Shikama, M.; Nakagami, G.; Noguchi, H.; Mori, T.; Sanada, H. Development of Personalized Fitting Device with 3-Dimensional Solution for Prevention of NIV Oronasal Mask-Related Pressure Ulcers. Respir. Care 2018, 63, 1024–1032. [Google Scholar] [CrossRef]
- Perry, M.A.; Jones, B.; Jenkins, M.; Devan, H.; Neill, A.; Ingham, T. Health System Factors Affecting the Experience of Non-Invasive Ventilation Provision of People with Neuromuscular Disorders in New Zealand. Int. J. Environ. Res. Public Health 2023, 20, 4758. [Google Scholar] [CrossRef]
- D’orazio, A.; Dragonetti, A.; Campagnola, G.; Garza, C.; Bert, F.; Frigerio, S. Patient Compliance to Non-Invasive Ventilation in Sub-Intensive Care Unit: An Observational Study. J. Crit. Care Nurs. 2018, 11, e65300. [Google Scholar] [CrossRef]
- McCormick, J.L.; Clark, T.A.; Shea, C.M.; Hess, D.R.; Lindenauer, P.K.; Hill, N.S.; Allen, C.E.; Farmer, M.S.; Hughes, A.M.; Steingrub, J.S.; et al. Exploring the Patient Experience with Noninvasive Ventilation: A Human-Centered Design Analysis to Inform Planning for Better Tolerance. Chronic Obstr. Pulm. Dis. 2022, 9, 80–94. [Google Scholar] [CrossRef]
- Elena, B.; Tommaso, P.; Gianluca, F.; Mario, S.; Antonello, N. The importance of education and training for noninvasive ventilation: Suggestions from the literature. Egypt. J. Intern. Med. 2019, 31, 435–441. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; AlAhmari, M.D. Evidence based synthesis for prevention of noninvasive ventilation related facial pressure ulcers. Saudi Med. J. 2018, 39, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Strickland, S.L. The Patient Experience During Noninvasive Respiratory Support. Respir. Care 2019, 64, 689–700. [Google Scholar] [CrossRef] [PubMed]
- NSW Agency for Clinical Innovation. Domiciliary Non-Invasive Ventilation in Adult Patients; A Consensus Statement; ACI: Sydney, NSW, Australia, 2012. [Google Scholar]
- Baixinho, C.L.; Bernardes, R.A.; Henriques, M.A. How to evaluate the risk of falls in institutionalized elderly people. Rev. Baiana Enferm. 2020, 34, e34861. [Google Scholar] [CrossRef]
- Volpato, E.; Banfi, P.; Pagnini, F.P. Promoting Acceptance and Adherence to Noninvasive Ventilation in Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Psychosom. Med. 2022, 84, 488–504. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Song, Y. Internet of things-based home noninvasive ventilation in COPD patients with hypercapnic chronic respiratory failure: Study protocol for a randomized controlled trial. Trials 2022, 23, 393. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, E.S.F.; Baixinho, C.L.; Presado, M.H.C.V. Qualitative research in health: A reflective approach. Rev. Bras. Enferm. 2019, 72, 830–831. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criterion | Exclusion Criterion | |
|---|---|---|
| P | Adults and elderly people submitted to NIV. | Age < 18 years. |
| C | Interventions to qualify clients and family caregivers to use and manage NIV: education and training, monitoring, communication, and behavioral strategies. | Interventions to qualify clients and families to use and manage IV. Formal caregivers. |
| C | Transitional care between hospital and community (hospital stay, hospital discharge, transition from hospital to home, first 30 days after returning home). | Residential facilities for elderly people, long-term care in health or social institutions, and rehabilitation units. |
| Search Strategy | Number of Articles | |
|---|---|---|
| #1 | (((((((((((((((((((Elderl*(Title/Abstract))) OR (aged(Title/Abstract))) OR (age*(Title/Abstract))) OR (older person*(Title/Abstract))) OR (older adult*(Title/Abstract))) OR (middle age(Title/Abstract))) OR (younger adult(Title/Abstract))) OR (frail older adults(Title/Abstract))) OR (aged(MeSH Terms))) OR (frail elderly(MeSH Terms))) OR (adult, frail older(MeSH Terms))) OR (adults, frail older(MeSH Terms))) OR (adult, young(MeSH Terms))) OR (adults, young(MeSH Terms))) OR (middle age(MeSH Terms))) OR (middle aged(MeSH Terms))) NOT (children(MeSH Terms))) NOT (adolescent(MeSH Terms))) NOT (adolescence(MeSH Terms)))) Filters: Free full text, in the last 5 years | 15,148 |
| #2 | ((((((((((((((((((((Mechanical ventilator(Title/Abstract)) OR (Cpap ventilation Positive end expiratory pressures(Title/Abstract))) OR (Mechanical ventilation(Title/Abstract))) OR (Biphasic continuous positive airway pressure(Title/Abstract))) OR (Bilevel continuous positive airway pressure(Title/Abstract))) OR (Inspiratory positive pressure ventilation(Title/Abstract))) OR (Positive end expiratory pressure(Title/Abstract))) OR (Non-invasive ventilation(Title/Abstract))) OR (Noninvasive ventilation(Title/Abstract))) OR (NIV(Title/Abstract))) OR (BIPAP(Title/Abstract))) OR (CPAP(Title/Abstract))) OR (IPAP(Title/Abstract))) OR (EPAP(Title/Abstract))) OR (PEEP(Title/Abstract))) OR (Biphasic positive airway pressure(Title/Abstract))) OR (Continuous positive airway pressure(Title/Abstract))) OR (Non-invasive positive pressure ventilation(Title/Abstract))) OR (Artificial Ventilation(Title/Abstract))) OR (non invasive positive pressure ventilation(MeSH Terms))) OR (positive pressure non invasive ventilation(MeSH Terms)) Filters: Free full text, in the last 5 years | 20,668 |
| #3 | (((((((transitional care(Title/Abstract)) OR (discharge(Title/Abstract))) OR (patient discharge(Title/Abstract))) OR (TCM(Title/Abstract))) OR (home nursing(Title/Abstract))) OR (discharge planning(MeSH Terms))) OR (discharge, patient(MeSH Terms))) OR (aides, home care(MeSH Terms)) Filters: Free full text, in the last 5 years | 47,391 |
| #4 | ((((((intervention(Title/Abstract)) OR (capacitation(Title/Abstract))) OR (health education(Title/Abstract))) OR (information(Title/Abstract))) OR (early intervention education(MeSH Terms))) OR (habilitation(MeSH Terms))) OR (health education(MeSH Terms))Filters: Free full text, in the last 5 years | 495,644 |
| #5 | #1 AND #2 AND #3 AND #4 | 148 |
| Reference, Origin Country, and Publication Year | Study Design and Objectives | Results |
|---|---|---|
| [9] Portugal 2017 | Integrative review | It is essential to define criteria for the care of people under NIV, including those for its prescription, maintenance, and evaluation. Equally fundamental are interface selection, initial setup, adjustments, and knowledge of NIV failure predictors. Noninvasive ventilation implies specific surveillance by clients, in which nurses play a prominent role. |
| [14] Spain 2017 | Literature review. Identifying risk factors for incidence of skin injuries associated with clinical devices caused by NIV, preventive strategies to reduce them, and the most effective treatment for injuries that cannot be avoided. | The mask of choice was the facial one, and foam or hydrocolloid dressings were always applied on the nasal bridge. The condition of the skin under the interface and harness must be evaluated every 4 h (recommended) or every 11 h (maximum). The interface rotation strategy must be evaluated at 24 h if NIV is still needed on an ongoing basis. |
| [15] UK 2019 | Systematic literature review. Evaluating the reason why clients needed long-term noninvasive positive pressure ventilation, describing some necessary nursing care procedures, and identifying some challenges experienced by nurses who provided home support when they interacted with these clients. | Noninvasive ventilation is a therapy that has been widely used in the home environment. Consequently, it is important that healthcare professionals understand the principles of its use in this setting and the challenges it can present for clients. Some crucial aspects that must be considered include the importance of proper mask adjustment, complications that clients can experience because of ventilation therapy, and how they can influence its effectiveness. Therefore, nurses are the professionals responsible for improving the way client care is managed at home by developing knowledge and specialized understanding of use of NIV in the domestic setting. This will promote client adherence, prevent complications, and decrease the number of hospital admissions. Using humidification units coupled to the ventilator can help some clients, but these units require daily cleaning. The container must be filled with boiled water so risk of contamination is reduced. |
| [18] United States 2019 | Survey study. Collecting data about the experiences and care transition of clients, as well as factors associated with post-discharge follow-up. | There were inconsistencies in care transition processes. The authors recommended health education sessions, follow-up appointments, phone calls, and support for home care. |
| [19] Germany 2019 | Qualitative study. Describing the quality of nursing care for clients submitted to NIV at home in Bavaria, Germany, and providing improvement recommendations from the perspective of health professionals. | This study described a heterogeneous and partly deficient care situation of people with NIV but showed that high quality care is possible if person-centered care is successfully implemented in all areas of service provision. Delivering person-centered care should be based on empowering ventilated patients to be completely involved in all decisions regarding their care and support. Care should support autonomy, focus on individuals’ needs and preferences, and enable ventilated patients and their families to consider treatment options and make informed decisions. Successful person-centered care initially requires the appropriate attitude to meet people’s needs (outcomes and impact), the involvement of ventilated patients in all decisions related to their care (service delivery), and a common vision of person-centered care provided by inspiring leadership (vision and leadership). |
| [16] China 2022 | Literature review. Providing an overview of titration and follow-up of clients under noninvasive positive pressure ventilation. Focused on different technologies, modalities, managements, and cost-effectiveness used in Internet of Things-based telemonitoring of home mechanical ventilation. | Actively monitoring and communicating information during follow-up were crucial for long-term adherence. The medical Internet of Things will shift care from hospitals and clinics to homes and mobile devices. Patients may communicate with doctors or nurses at home via smart phones, mobile applications (apps), or the Internet. The Internet of Things allows users to access these “things” wherever and whenever they require them. There are a lot of opportunities for the Internet of Things to help remote caregivers ensure the safety of patients with noninvasive positive pressure ventilation and other wearable devices and raise warnings over critical situations. In this situation, providers should respond immediately to patient needs. |
| [17] Brazil 2022 | Integrative review. Identifying the needs of critically ill patients who had to be submitted to NIV and their families, as well as nursing interventions that promoted adaptation of these patients and their families to NIV. | Adaptation of clients under NIV was promoted by implementing nursing interventions, both pharmacological and nonpharmacological. It is important to first adopt a nonpharmacological intervention, which includes four essential domains: communication, technology, comfort promotion, and environmental management. It is critical that nurses develop nursing technology competencies so that these professionals can allow technology and care to coexist harmoniously and develop activities oriented toward promoting clients’ physical integrity. |
| [20] Portugal 2021 | Book with evidence on COPD. Identifying nursing care that must be implemented to help clients with COPD regarding use of NIV during exacerbations and at home and informing them about the importance of motor and cardiorespiratory training for clients’ activities of daily living with the purpose of maintaining their quality of life. | It is important to take a few breaks in the use of the mask for clients to moisten their face, humidify the oral mucosa, and clean the mouth with mouthwash. Some breathing techniques stood out, such as inhaling through the nose with the mouth closed, directing the air into the abdomen, carrying out diaphragmatic breathing, and slowly exhaling through the mouth with the lips half-closed. The study presented care procedures for different complications associated with NIV. |
| Nursing Interventions to Train Clients and Families to Correctly Use NIV in the Transition from Hospital to Community |
|---|
| Masks or interfaces [9,14,15,17,20] Teaching of mask or interface placement and training in their adjustment. - Full face masks: upper edge supported on the nose wings, lower edge resting on the chin. - Nose mask: resting on the nose wings between the nose and the upper lip. - First adjust the mask and then the harness, without exerting too much pressure. |
| Prevention of complications associated with NIV [9,14,15,16,17,20] Pressure injuries: - Correctly moisturize the skin. - Check the skin condition every two hours. - Use hydrocolloid or polyurethane dressings in the areas under highest pressure. - Remove the mask intermittently to provide the areas under highest pressure with some relief. Eye discomfort: - Apply artificial tears and wet eye dressings. Nasal congestion: - Wash the nose with saline solution. - Apply steroids and antihistamines. Dry mouth and nasal mucosae: - Clean the mouth with mouthwash. - Orally hydrate the mucosae by drinking liquids. - Use humidification units coupled to the ventilator (use boiled water to reduce risk of contamination). Abdominal distension: - Keep the mouth closed when using the NIV device. - Promote mobilization and elimination of secretions. - Use antiflatulents if necessary. - Do exercises that recruit the lower limbs. Risk of vomit aspiration: - Watch the clients for some time after they take solid and liquid food. - Keep clients in Fowler’s position for at least 30 min after meals. - Remove the equipment in case of nausea or vomiting. |
| Leakage control [9,14,15,17,20] - Choose the mask correctly, opting for one with smaller dimensions, or change the mask type according to new needs and meet the requirements of each model. - During mask placement, make sure that it does not collide with the corners of the eyes and/or the mouth. - Observe the correct body position and make sure that the mask is placed when clients are in the proper position for receiving NIV. - Look around the mask in search of small leakages. - In case of the use of dental prosthesis, keep it in during the NIV procedure. - Avoid the presence of facial hair, namely beards. - Use fixation systems (for example, support for the chin). |
| Maintenance and cleaning of ventilators and accessories [17,20] - Clean the external surface of the ventilator with a wet cloth. - Wash the filters once a month with warm water and soap, then dry them properly before inserting them again. It is essential to replace them every six months. - Disassemble the mask and accessories fully once a week, wash whatever possible with warm water and soap, and dry it properly before assembling it again. - Clean the circuit externally with a wet cloth, without using cleaning products. - Place the equipment on a flat and stable surface in an airy, low-humidity place. - Always have a spare mask and circuit. |
| Respiratory training [9,20] Instructing in and monitoring breathing techniques: - Inhale through the nose with the mouth closed, directing the air into the abdomen. - Carry out diaphragmatic breathing. - Slowly exhale through the mouth with the lips half-closed. Positions for relaxation and respiratory control: - Sitting: feet firmly touching the floor, body slightly tilted forward, and elbows resting on the thighs. - Lying down: right lateral decubitus with the headboard elevated. - Standing up: elbows resting on a surface (for instance a low wall, a counter), with the body slightly tilted forward. -Semi-Fowler’s position. Techniques to clean the airway: - Inhale deeply. - Ensure proper hydration to guarantee secretion fluidification. - Carry out respiratory physical therapy. - Cough vigorously in one go, with the mouth open, to eliminate secretions. |
| Ventilator monitoring [9,14,15,16,19,20] - Reevaluate parameters up to three months after the beginning of the therapy. Subsequently, evaluation must occur annually. - Make sure the company that provided the equipment pays home visits at the beginning of the therapy and four weeks later. - Provide information about the presence of an alarm in the equipment, which allows identification of air leakage and consequent need to adjust the mask. |
| Communication and behavioral strategies [17,18,19,20] - Ensure a calm and quiet environment. - Speak in a soft and calm tone of voice. - Maintain eye contact with clients. - Keep a calm attitude, which conveys self-confidence and competence. - Promote resting and relaxation positions (for example, diaphragmatic breathing). - Learn how to put the mask on and attach it and do these procedures by yourself (if you are a client). - Provide information about the possible presence of alarms. - Suggest that clients try music therapy. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernando, J.M.G.; Marçal, M.M.G.; Ferreira, Ó.R.; Oliveira, C.; Pedreira, L.; Baixinho, C.L. Nursing Interventions for Client and Family Training in the Proper Use of Noninvasive Ventilation in the Transition from Hospital to Community: A Scoping Review. Healthcare 2024, 12, 545. https://doi.org/10.3390/healthcare12050545
Fernando JMG, Marçal MMG, Ferreira ÓR, Oliveira C, Pedreira L, Baixinho CL. Nursing Interventions for Client and Family Training in the Proper Use of Noninvasive Ventilation in the Transition from Hospital to Community: A Scoping Review. Healthcare. 2024; 12(5):545. https://doi.org/10.3390/healthcare12050545
Chicago/Turabian StyleFernando, Jéssica Moura Gabirro, Margarida Maria Gaio Marçal, Óscar Ramos Ferreira, Cleoneide Oliveira, Larissa Pedreira, and Cristina Lavareda Baixinho. 2024. "Nursing Interventions for Client and Family Training in the Proper Use of Noninvasive Ventilation in the Transition from Hospital to Community: A Scoping Review" Healthcare 12, no. 5: 545. https://doi.org/10.3390/healthcare12050545