
Reduction in the Incidence Density of Pressure Injuries in Intensive Care Units after Advance Preventive Protocols
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Methods
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Padula, W.V.; Black, J.M.; Davidson, P.M.; Kang, S.Y.; Pronovost, P.J. Adverse Effects of the Medicare PSI-90Hospital Penalty System on Revenue-Neutral Hospital-Acquired Conditions. J. Patient Saf. 2020, 16, e97–e102. [Google Scholar] [CrossRef]
- Alderden, J.; Rondinelli, J.; Pepper, G.; Cummins, M.; Whitney, J. Risk factors for pressure injuries among critical care patients: A systematic review. Int. J. Nurs. Stud. 2017, 71, 97–114. [Google Scholar] [CrossRef]
- Chaboyer, W.P.; Thalib, L.; Harbeck, E.L.; Coyer, F.M.; Blot, S.; Bull, C.F.; Nogueira, P.C.; Lin, F.F. Incidence and Prevalence of Pressure Injuries in Adult Intensive Care Patients: A Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, e1074–e1081. [Google Scholar] [CrossRef]
- Lin, F.; Wu, Z.; Song, B.; Coyer, F.; Chaboyer, W. The effectiveness of multicomponent pressure injury prevention programs in adult intensive care patients: A systematic review. Int. J. Nurs. Stud. 2020, 102, 103483. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.E.; Durrant, L.A.; Hutchinson, M.; Ballard, C.A.; Neville, S.; Usher, K. Living with multiple losses: Insights from patients living with pressure injury. Collegian 2018, 25, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Lovegrove, J.; Fulbrook, P.; Miles, S. Prescription of pressure injury preventative interventions following risk assessment: An exploratory, descriptive study. Int. Wound J. 2018, 15, 985–992. [Google Scholar] [CrossRef]
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline, 3rd ed.; EPUAP/NPIAP/PPPIA: Westford, MA, USA, 2019. [Google Scholar]
- Tayyib, N.; Coyer, F. Effectiveness of Pressure Ulcer Prevention Strategies for Adult Patients in Intensive Care Units: A Systematic Review. Worldviews Evid. Based Nurs. 2016, 13, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.; Finch Guthrie, P.; Kraft, W.; Reicks, P.; Skay, C.; Beal, A.L. Universal Pressure Ulcer Prevention Bundle with WOC Nurse Support. J. Wound Ostomy Continence Nurs. 2015, 42, 217–225. [Google Scholar] [CrossRef]
- Tayyib, N.; Coyer, F. Translating Pressure Ulcer Prevention Into Intensive Care Nursing Practice: Overlaying a Care Bundle Approach with a Model for Research Implementation. J. Nurs. Care Qual. 2017, 32, 6–14. [Google Scholar] [CrossRef]
- Santy-Tomlinson, J.; Limbert, E. Using the SSKIN care bundle to prevent pressure ulcers in the intensive care unit. Nurs. Stand. 2020, 35, 77–82. [Google Scholar]
- Byrne, S.; Patton, D.; Avsar, P.; Strapp, H.; Budri, A.; O’Connor, T.; Nugent, L.; Moore, Z. Sub epidermal moisture measurement and targeted SSKIN bundle interventions, a winning combination for the treatment of early pressure ulcer development. Int. Wound J. 2022, 20, 1987–1999. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, Z.; Zhao, B.; Zhang, Q.; Li, Z. Implementing a Pressure Injury Care Bundle in Chinese Intensive Care Units. Risk Manag. Healthc. Policy 2021, 14, 2435–2442. [Google Scholar] [CrossRef]
- Kennerly, S.M.; Sharkey, P.D.; Horn, S.D.; Alderden, J.; Yap, T.L. Nursing Assessment of Pressure Injury Risk with the Braden Scale Validated against Sensor-Based Measurement of Movement. Healthcare 2022, 10, 2330. [Google Scholar] [CrossRef]
- Rivera, J.; Donohoe, E.; Deady-Rooney, M.; Douglas, M.; Samaniego, N. Implementing a Pressure Injury Prevention Bundle to Decrease Hospital-Acquired Pressure Injuries in an Adult Critical Care Unit: An Evidence-Based, Pilot Initiative. Wound Manag. Prev. 2020, 66, 20–28. [Google Scholar] [CrossRef]
- Tayyib, N.; Asiri, M.Y.; Danic, S.; Sahi, S.L.; Lasafin, J.; Generale, L.F.; Malubay, A.; Viloria, P.; Palmere, M.G.; Parbo, A.R.; et al. The Effectiveness of the SKINCARE Bundle in Preventing Medical-Device Related Pressure Injuries in Critical Care Units: A Clinical Trial. Adv. Skin Wound Care 2021, 34, 75–80. [Google Scholar] [CrossRef]
- Coyer, F.; Gardner, A.; Doubrovsky, A.; Cole, R.; Ryan, F.M.; Allen, C.; McNamara, G. Reducing pressure injuries in critically ill patients by using a patient skin integrity care bundle (InSPiRE). Am. J. Crit. Care 2015, 24, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Shiju, S.; Chacko, G.; Thomas, M.; Abas, A.; Savarimuthu, I.; Omari, E.; Al-Balushi, S.; Jessymol, P.; Mathew, S.; et al. A quality improvement programme to reduce hospital-acquired pressure injuries. BMJ Open Qual. 2020, 9, e000905. [Google Scholar] [CrossRef]
- Lovegrove, J.; Fulbrook, P.; Miles, S. International consensus on pressure injury preventative interventions by risk level for critically ill patients: A modified Delphi study. Int. Wound J. 2020, 17, 1112–1127. [Google Scholar] [CrossRef]
- Rêgo, A.d.S.; Furtado, G.E.; Bernardes, R.A.; Santos-Costa, P.; Dias, R.A.; Alves, F.S.; Ainla, A.; Arruda, L.M.; Moreira, I.P.; Bessa, J.; et al. Development of Smart Clothing to Prevent Pressure Injuries in Bedridden Persons and/or with Severely Impaired Mobility: 4NoPressure Research Protocol. Healthcare 2023, 11, 1361. [Google Scholar] [CrossRef]
- Gibelli, F.; Bailo, P.; Sirignano, A.; Ricci, G. Pressure Ulcers from the Medico-Legal Perspective: A Case Report and Literature Review. Healthcare 2022, 10, 1426. [Google Scholar] [CrossRef]
- Chao, W.-Y.; Wu, Y.-L.; Liao, W.-C. Psychometric Properties of the Taiwanese Pressure Ulcer Management Self-Efficacy Scale in Nursing Practice. Healthcare 2022, 10, 1900. [Google Scholar] [CrossRef]
- Furtado, K.; Voorham, J.; Infante, P.; Afonso, A.; Morais, C.; Lucas, P.; Lopes, M. The Relationship between Nursing Practice Environment and Pressure Ulcer Care Quality in Portugal’s Long-Term Care Units. Healthcare 2023, 11, 1751. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Items | Action |
|---|---|
| Surface | Air suspension bed for patients with higher risk of pressure injuries. The others use a pressure-reduced bed. When lying flat, place a pillow under both knees and calves to keep the heels off the bed. When lying on the side, place a pillow (at a 30-degree angle) behind the back to relieve pressure on the coccyx. The shoulder and hip joints on the side should be slightly tilted outward to relieve pressure. Bend the leg on the upper side, place a pillow between the knees, and ensure that the knees are not under pressure and the ankles are elevated. After turning over, adjust the position of the head and place a rolled towel behind the ear. Artificial skin pressure reduction products should be used at the pressure points when using a nasal intermittent positive pressure ventilation and loosened every 2 hours to inspect the skin. Ensure nasogastric tube or endotracheal tube fixed with Ω sharp without stressing nasal wings, and oxygen mask without pressuring nasal bridges or auricles with foam dressings. |
| Skin investigation | New patients and during reposition period, a real-time “head-to-toe” assessment of overall skin temperature, color, moisture status, and integrity, with particular attention to bony prominences. During each shift period, the overall risk for pressure injuries was assessed using the Braden Scale [1], which includes factors such as sensory perception, moisture, activity, mobility, nutrition, and friction/shear. A score of ≤14 is used to identify patients at high risk for pressure injuries. Check that the tubes are not under pressure by skin. Avoid compressing area that includes redness and refrain from massaging bony prominences. |
| Kinetics/keep moving | The turning schedule and prohibited actions were strictly followed to assist in changing the patient’s position and limb placement correctly every 2 h. Encourage early movement, perform physical therapy, relieve spasticity, and limit sedative use. The bed should be leveled before turning the patient, and grasp the turning sheet closer to the patient’s side and lift, avoiding pushing or pulling. After turning over, raise the foot end of the bed before elevating the head end, ensuring that the angle does not exceed 30 degrees and replace the position of the pulse oximeter. |
| Incontinence/moisture | Identify the stage of incontinence-associated dermatitis and fungal infection. Cleanse the skin affected by incontinence with water. To protect irritable skin from the urine or stool, keep skin clean and dry. |
| Nutrition/hydration | The nutritionists evaluated each patient after hospitalization and assessed their nutritional statuses twice every week to ensure adequate intake of protein and calories. |
| Variables | Pre-Bundle Stage (n = 2134) | Post-Bundle Stage (n = 2146) | p |
|---|---|---|---|
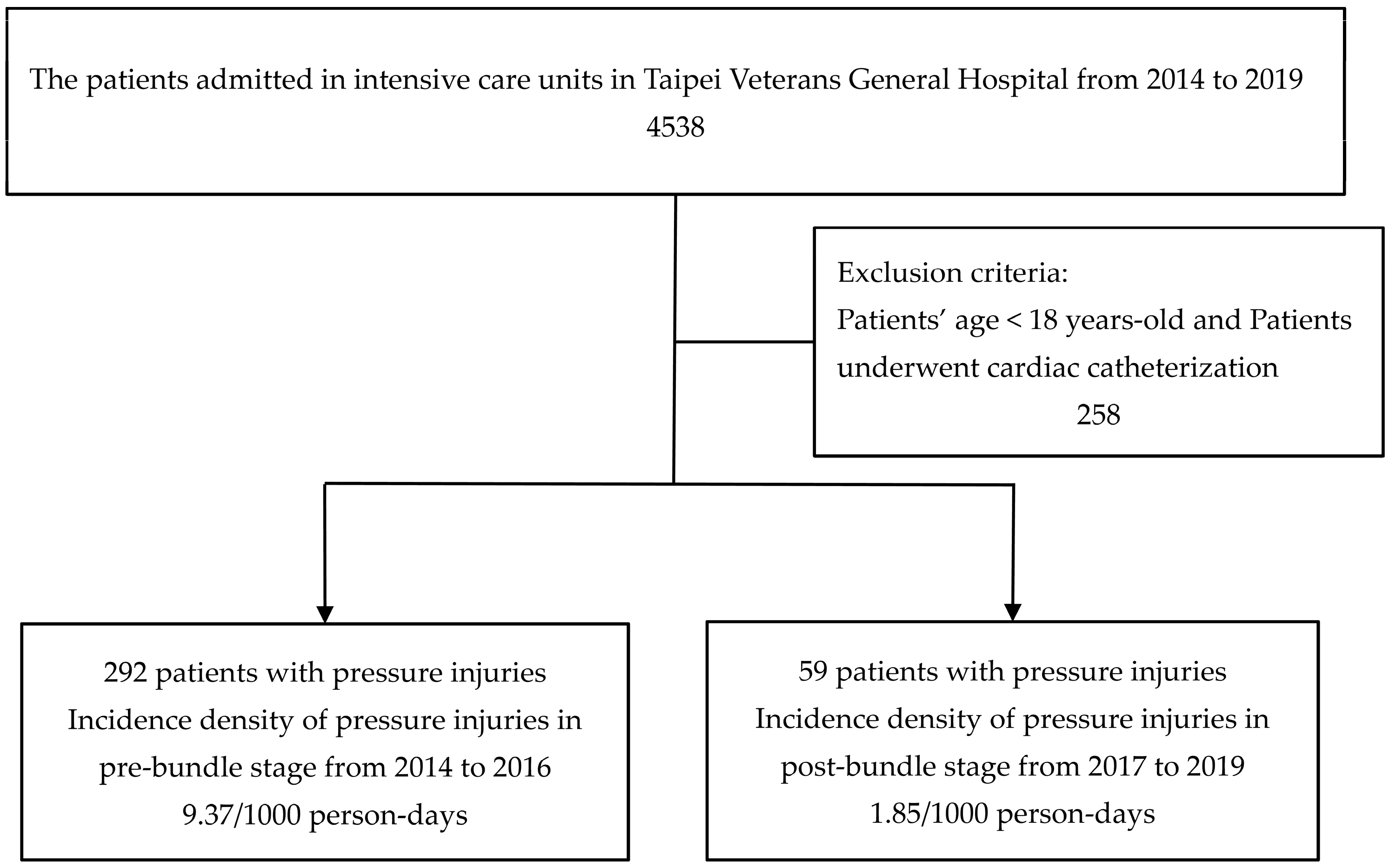
| The cases of PrIs | 292 | 59 | <0.001 * |
| Incidence density (/1000 person days) of PrIs | 9.37 | 1.85 | <0.001 * |
| Sex (Male) | 1356 (63.54%) | 1345 (62.67%) | 0.539 |
| Age | 67.18 ± 17.53 | 67.55 ± 15.98 | 0.839 |
| Length of stay | 14.60 ± 11.52 | 14.90 ± 12.55 | 0.555 |
| Glasgow Coma scale | 10.84 ± 4.111 | 10.88 ± 3.927 | 0.805 |
| Body weight | 62.86 ± 14.57 | 63.48 ± 14.83 | 0.179 |
| Albumin (g/dL) | 2.886 ± 0.597 | 3.100 ± 0.592 | 0.214 |
| Ventilation | 8.422 ± 7.466 | 8.205 ± 7.800 | 0.419 |
| Potassium (mEq/L) | 3.977 ± 0.813 | 3.921 ± 0.718 | 0.407 |
| Sodium (mEq/L) | 139.8 ± 7.491 | 140.3 ± 7.272 | 0.694 |
| Calorie achievement rate | 72.57 ± 21.19 | 69.37 ± 22.48 | 0.722 |
| Charlson comorbidity index | 5.29 ± 2.32 | 5.02 ± 2.27 | 0.184 |
| APACHE II score within first day | 21.20 ± 7.03 | 22.32 ± 8.36 | 0.169 |
| APACHE II score | 20.21 ± 7.58 | 19.75 ± 8.45 | 0.175 |
| Pain scores | 1.64 ± 1.52 | 1.49 ± 1.96 | 0.360 |
| Incontinence-associated dermatitis | 447 (20.95%) | 462 (21.53%) | 0.642 |
| Restraints | 1908 (89.41%) | 1871 (87.19%) | 0.024 * |
| Sedation | 1410 (66.07%) | 1473 (68.64%) | 0.073 |
| Muscle relaxant | 32 (1.5%) | 31 (1.44%) | 0.881 |
| Inotropic agents | 368 (17.24%) | 372 (17.33%) | 0.938 |
| Pain control | 1651 (77.37%) | 1669 (77.78%) | 0.75 |
| Ventilation | 1944 (91.1%) | 1931 (89.98%) | 0.213 |
| Life support system | 115 (5.39%) | 112 (5.22%) | 0.804 |
| Nurse–patient ratio | 2.53 (0.01) | 2.6 (0.02) | 0.374 |
| Pre-Bundle Stage Incidence Density (/00) | Post-Bundle Stage Incidence Density (/00) | Relative Risk | p | |
|---|---|---|---|---|
| Overall PrIs | 9.37 | 1.85 | 0.197 (95% C.I.: 0.149–0.26) | <0.001 * |
| Non-iatrogenic PrIs | 6.67 | 0.84 | 0.126 (95% C.I.: 0.085–0.189) | <0.001 * |
| Sacrum | 2.5 | 0.41 | 0.162 (95% C.I.: 0.09–0.292) | <0.001 * |
| Back | 0.42 | 0.16 | 0.375 (95% C.I.: 0.134–1.051) | 0.062 |
| Ischium | 1.44 | 0.03 | 0.022 (95% C.I.: 0.003–0.157) | <0.001 * |
| Occiput | 0.19 | 0 | ||
| Low limbs | 2.12 | 0.25 | 0.118 (95% C.I.: 0.057–0.246) | 0.001 * |
| Knee | 0.35 | 0.03 | 0.089 (95% C.I.: 0.011–0.686) | 0.02 * |
| Ankle | 0.45 | 0.13 | 0.278 (95% C.I.: 0.092–0.846) | 0.024 * |
| Heel | 1.32 | 0.09 | 0.071 (95% C.I.: 0.022–0.23) | <0.001 * |
| Iatrogenic PrIs | 2.7 | 1 | 0.371 (95% C.I.: 0.247–0.558) | <0.001 * |
| Nose | 1.22 | 0.47 | 0.385 (95% C.I.: 0.212–0.699) | 0.002 * |
| Nasal wings | 0.67 | 0.41 | 0.603 (95% C.I.: 0.302–1.205) | 0.152 |
| Nasal bridge | 0.55 | 0.06 | 0.115 (95% C.I.: 0.026–0.496) | 0.004 * |
| Auricle | 0.67 | 0.25 | 0.371 (95% C.I.: 0.164–0.838) | 0.017 * |
| Face | 0.51 | 0.13 | 0.244 (95% C.I.: 0.081–0.729) | 0.012 * |
| Upper limbs | 0.29 | 0.16 | 0.541 (95% C.I.: 0.181–1.615) | 0.271 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lien, R.-Y.; Wang, C.-Y.; Hung, S.-H.; Lu, S.-F.; Yang, W.-J.; Chin, S.-I.; Chiang, D.-H.; Lin, H.-C.; Cheng, C.-G.; Cheng, C.-A. Reduction in the Incidence Density of Pressure Injuries in Intensive Care Units after Advance Preventive Protocols. Healthcare 2023, 11, 2116. https://doi.org/10.3390/healthcare11152116
Lien R-Y, Wang C-Y, Hung S-H, Lu S-F, Yang W-J, Chin S-I, Chiang D-H, Lin H-C, Cheng C-G, Cheng C-A. Reduction in the Incidence Density of Pressure Injuries in Intensive Care Units after Advance Preventive Protocols. Healthcare. 2023; 11(15):2116. https://doi.org/10.3390/healthcare11152116
Chicago/Turabian StyleLien, Ru-Yu, Chien-Ying Wang, Shih-Hsin Hung, Shu-Fen Lu, Wen-Ju Yang, Shu-I Chin, Dung-Hung Chiang, Hui-Chen Lin, Chun-Gu Cheng, and Chun-An Cheng. 2023. "Reduction in the Incidence Density of Pressure Injuries in Intensive Care Units after Advance Preventive Protocols" Healthcare 11, no. 15: 2116. https://doi.org/10.3390/healthcare11152116