1. Introduction
Self-medication practices have increased in Japan since the revised Pharmaceutical Affairs Act was enacted in 2009 [
1]. As medicines that can be purchased without a prescription, over-the-counter (OTC) medication plays an important role in self-medication [
2,
3,
4,
5,
6,
7]. Consumers make decisions for self-medication based on the information published by manufacturers and the additional information from other sources. Obtaining inappropriate information about OTC medication presents potential barriers and health risks for self-medication [
8,
9,
10]. On the one hand, manufacturers gather factual medical information before launching a medication and subsequently releasing it to the public. However, previous studies have reported potential barriers and risks in obtaining information for consumers from packaging and labels [
11,
12,
13,
14,
15]. On the other hand, obtaining medical information in addition to what is provided by manufacturers also poses potential barriers and risks, especially when such information is obtained through the Internet [
16,
17,
18,
19]. As a country promoting self-health management, health information technology (HIT) plays an active role in Japan [
20,
21]. During the COVID-19 pandemic, Japanese consumers were able to use health-related applications to self-monitor their physical condition and record their medication information on smartphones. Considering the positive roles of mobile Internet, health-related applications on smartphones, and the advantages of information processing in HIT [
22,
23,
24,
25], we assume that an OTC medication electronic health records (OTC-EHR) design based on obtaining and sharing health information in relation to self-medication may improve potential health risks caused by inappropriate information acquisition. This study attempts to investigate consumers’ attitudes towards obtaining and sharing health information and attitudes towards health-related applications and their characteristics to test the hypotheses regarding the conceptual design of the OTC-EHR.
The electronic health record (EHR) is a well-established concept in the field of HIT, with more positive characteristics than negative ones [
26]. It actively contributes to patient-physician communication [
22,
27] and helps serve public health [
26]. Studies have shown that co-interventions involving EHR and nurses’ assistance positively impacted medication self-management [
28,
29], and improvements in EHR design are required for effective self-management [
30]. Due to the positive impacts of EHR, it has been widely used in the clinical field, but it is usually overlooked for non-prescription medicines [
31,
32,
33]. OTC medication plays an essential role in Japan [
1,
20]. Researchers in Japan have investigated the potential positive effects of EHR, and most respondents have a positive attitude towards it. However, studies on EHR are limited in Japan [
21,
34,
35]. As for OTC-EHR, related research is required to be continued [
31], especially from the consumers’ perspective.
Regarding Japanese consumers’ attitudes towards OTC-EHR, considering their favorable attitudes towards technology may facilitate a greater use of OTC-EHR.
Moreover, the perceived usefulness of EHR may positively affect EHR use [
27,
36]. Considering the abovementioned information, the following hypotheses were formulated:
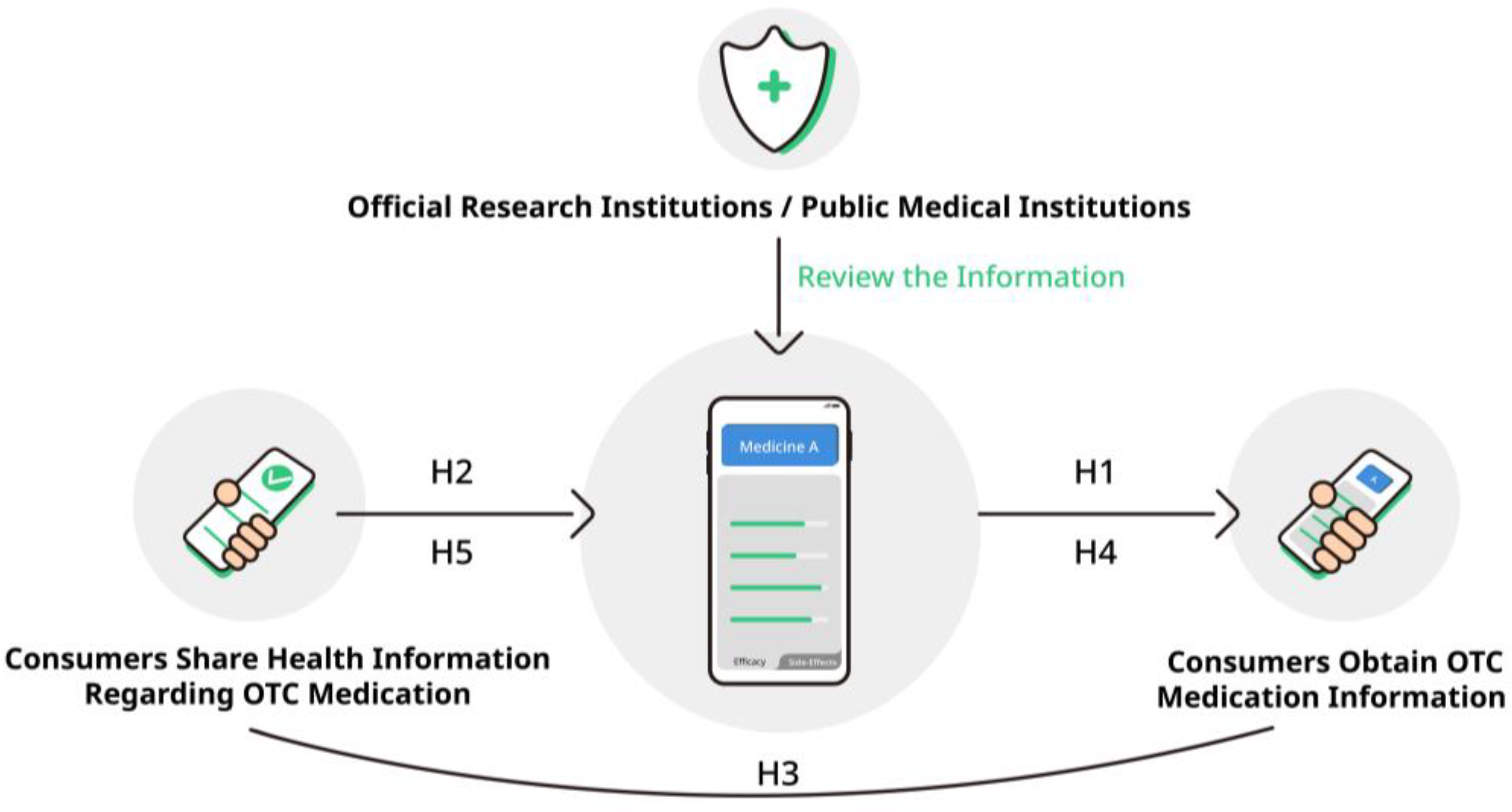
H1. Consumers exhibit a positive attitude towards obtaining user-shared health information on OTC medication.
H2. Consumers exhibit a positive attitude towards sharing anonymized health information while using OTC medication.
H3. There is a positive association between consumers obtaining and sharing health information regarding OTC medication.
Moreover, since the conceptual design of OTC-EHR will be based on the medication information system design, it is necessary to consider the influence of consumers’ experience with related health applications on their attitude towards OTC-EHR use.
During the COVID-19 pandemic, in Japan, people could record their health status and report it through smartphone applications [
37,
38], thereby encouraging them to use HIT for self-health management. Examples include the medication notebook application and the health observation application. Users can use the medication notebook application to record the name of the medicine and usage, along with past experiences of allergies and side effects [
37]. The health observation application is a kind of physical condition observation application, which was widely used in Japan to record one’s physical condition during the COVID-19 pandemic [
38]. Considering the potential positive and negative factors of OTC-EHR [
31], and based on the kind of database of medication notebook and health observation application that records and reports personal health information [
37,
38], this study proposes a consumer-centered OTC-EHR conceptual design based on obtaining and sharing OTC medication information with official research institutions and public medical institutions as review agencies [
39].
Figure 1 shows the conceptual design speculative model for the OTC-EHR. Specifically, consumers share health information while using the OTC medication, called user-shared health information, which the review agencies review and make accessible to the users of the OTC-EHR. This design is expected to improve the potential risks facing consumers obtaining additional OTC medication information that has not been authenticated for use in self-medication. Since this study focuses on consumer attitudes toward obtaining and sharing information in the OTC-EHR, how agencies review relevant information will not be discussed in the present study.
In addition, consumer behavior regarding self-medication and HIT may vary according to eHealth literacy, gender and age. eHealth literacy is the consumer’s capacity to use digital health information to address health-related issues and is essential in digital healthcare [
8,
10,
40]. Previous studies suggest eHealth literacy’s positive role in Japanese consumers’ related health behaviors and digital health information acquisition [
39,
41]. Other studies have suggested that women may have a stronger motivation to seek Internet health information. Although younger adults use the Internet more overall, middle-aged adults are more likely to seek health information online [
39,
42,
43,
44]. Moreover, regarding OTC medication purchases, women and younger adults may buy OTC medicines more frequently [
1,
7].
We therefore propose the following hypotheses considering eHealth literacy and consumers’ attitudes:
H4. Consumers with high eHealth literacy have a greater inclination to obtain user-shared information regarding OTC medication.
H5. Consumers with high eHealth literacy are more optimistic about sharing anonymized health information regarding OTC medication.
The present study aims to investigate consumers’ relevant attitudes to test the research hypotheses for the OTC-EHR conceptual design from two perspectives: (i) attitudes towards obtaining user-shared OTC medication information; and (ii) the usage of health-related applications and the inclination to share anonymized health information.
4. Discussion
This study tested the hypotheses for the OTC-EHR conceptual design from the perspectives of obtaining and sharing anonymized health information regarding OTC medication usage for self-medication.
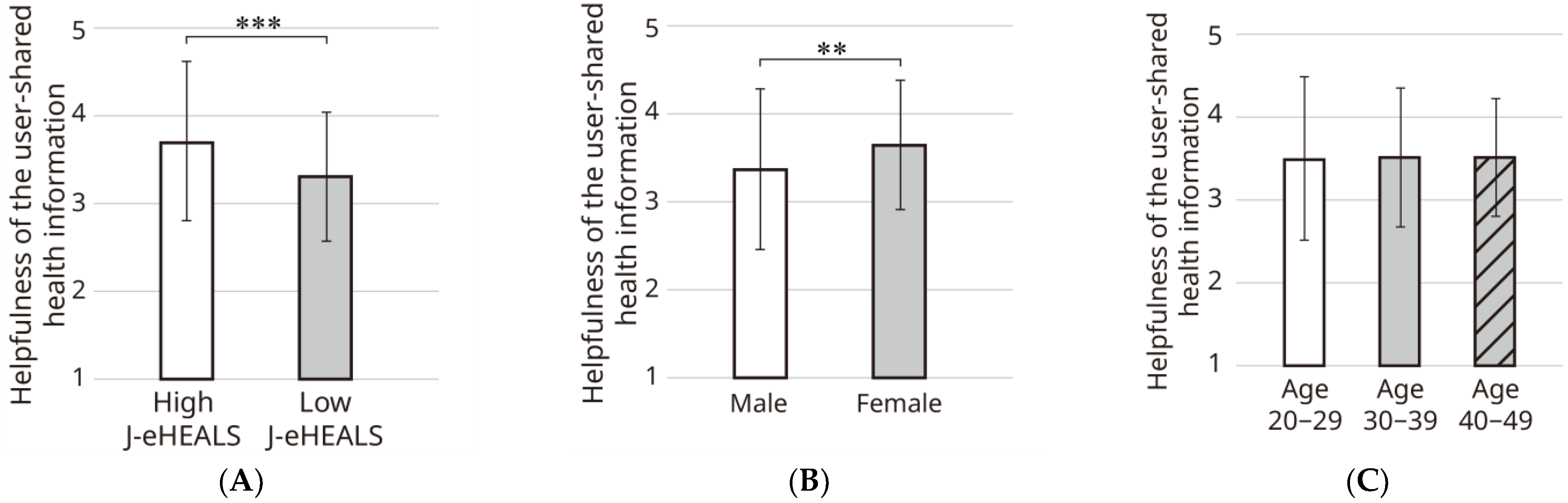
Participants, especially women and those with high eHealth literacy indicated relatively positive attitudes towards the use of user-shared OTC medication information, thus partially supporting hypotheses H1 and H3. This phenomenon may be explained by the fact that high eHealth literacy consumers are better at obtaining and judging medical and health information from digital sources [
8,
10,
40], and the perceived utility of health information technology tools is correlated with health literacy levels [
22]. The higher motivation of women in this study may be because they are more likely to seek health information [
43,
44,
63].
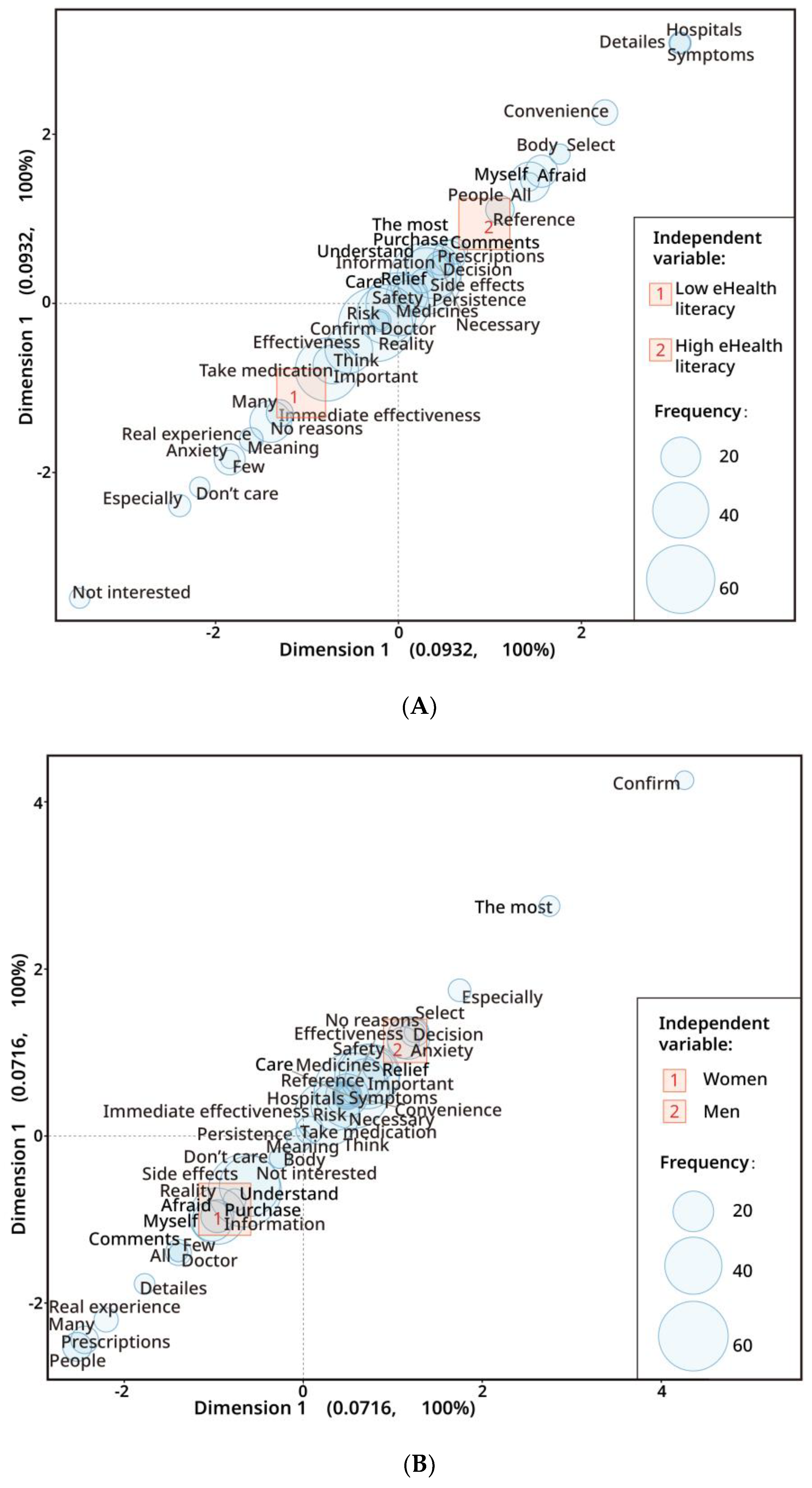
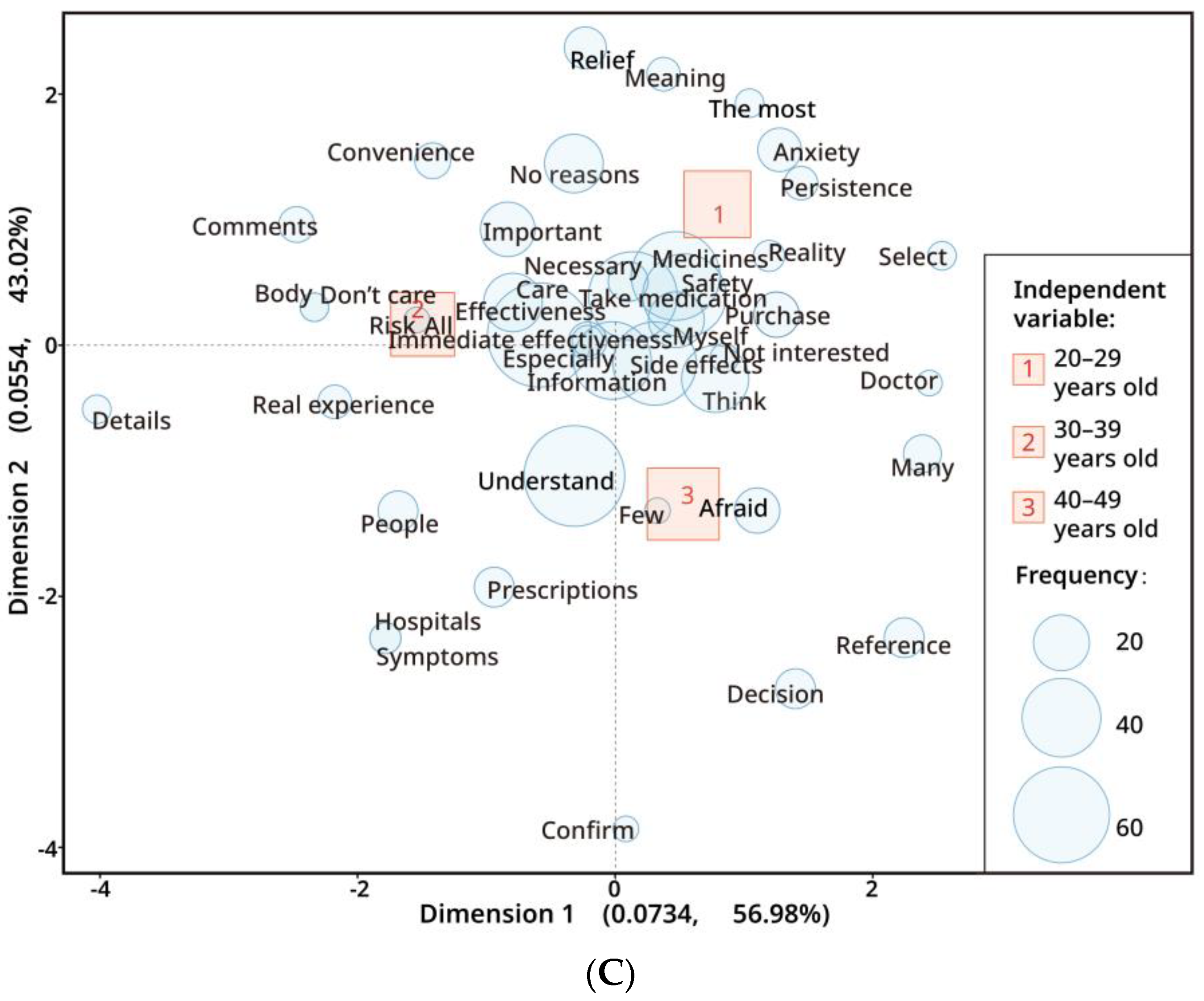
Combining the quantitative and text-mining analysis results, most consumers were concerned about the OTC medication information, including efficacy, safety, side effects, and persistence. Furthermore, regarding the user-shared medication information, a portion of consumers with high eHealth literacy, women, and consumers in the older age groups were inclined to know more medication-related details, such as the physical condition of the person reporting the medication information, their real experiences, and whether they have been to the hospital, to help their self-decision. These differences in information needs may be influenced by experience, information accessibility, and different medication needs [
1,
40,
44], and more evidence is needed to explain these phenomena.
Hence, it is necessary to design the OTC medication information through an appropriate interface, including personalized detailed medication information of those who shared their information, to reach different users with different characteristics more efficiently and comprehensively, while improving their potential barriers and risks in accessing medical information. In addition, reducing the potential digital divide caused by different consumer characteristics and ensuring equal access to information on OTC-EHR through design must be addressed, which requires more studies [
27].
In terms of the results of the attitudes towards sharing anonymized health information regarding OTC medication, the proportion of participants who use health applications is low; most consumers only have smartphones and do not use applications to record and report their health information. The study findings did not indicate that consumers with higher eHealth literacy have a more positive attitude towards medication information-sharing. Thus, hypotheses H2 and H4 were not supported. This potential resistance to anonymized health information sharing may emerge from, on the one hand, consumers’ concerns about information security and privacy [
34,
39,
64]. Even though we clarified to the participants that the information shared would be anonymized, it did not reduce their psychological barriers. On the other hand, resistance may also be because of the penetration rate of EHRs [
27,
35], and the low usage rate of health-related applications found in this study.
It is noteworthy, however, that consumers’ favorable attitudes towards technology may facilitate greater use, as the perceived usefulness of EHR may have a positive effect on EHR use [
27,
36]. Our results also suggest that the perceived helpfulness of OTC-EHR by participants in this study may be positively associated with the usage of health-related applications and attitude towards sharing anonymized health information. Hypothesis H5 is partially confirmed. Therefore, first, it is important to use appropriate information and interface design to emphasize information security to reduce users’ psychological barriers. Second, the penetration rate of OTC-EHR should be improved to enhance the limited motivation to share anonymized health information regarding OTC medication. Considering the positive role of personal feedback on EHR [
65], conducting OTC-EHR using a small database and encouraging consumers to have more access to OTC-EHR so as to improve their attitude towards information sharing is recommended. In addition, regarding OTC-EHR as a database of medication usage, maintaining design consistency and developing uniform design standards may positively reduce barriers for consumers in various usage scenarios, reduce user confusion, and potentially improve the use of OTC-EHR.
Limitations
The present study has some limitations. First, this study did not explain in detail how agencies review relevant information, which will be studied in further research. Second, due to the limitations of research methods, this study did not explain in detail the interaction between the motivation to obtain and share anonymized health information regarding OTC medication, particularly the reasons for the psychological barriers to sharing anonymized health information. Considering the penetration rate of EHRs and health-related applications, this needs to be studied soon in conjunction with prototyping. Experiments based on prototyping will improve the knowledge on user behavior and perception. Third, the study sample has a user recruitment bias, as age groups older than 49 years are not addressed in this study. There is a need for a separate study on EHRs and the behavior of the elderly, given Japan’s aging population [
66] and the potential for digital behavior change [
44]. In addition, the present study was only conducted in the Kanto area of Japan to reduce the potential influence of cultural differences. It also excluded the impact of professional knowledge as those in medicine-related occupations. Therefore, future studies will expand the research scope by addressing these issues.









{kind=link}
{kind=link}
{kind=link}
{kind=link}