

Geriatric Care Management System Powered by the IoT and Computer Vision Techniques

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Related Works
2.1. The Use of Wearable Devices
2.2. Contactless Measurement of Vital Signs
2.3. Benefits of Computer Vision Techniques
3. Materials and Methods
Performance Metrics
4. Results
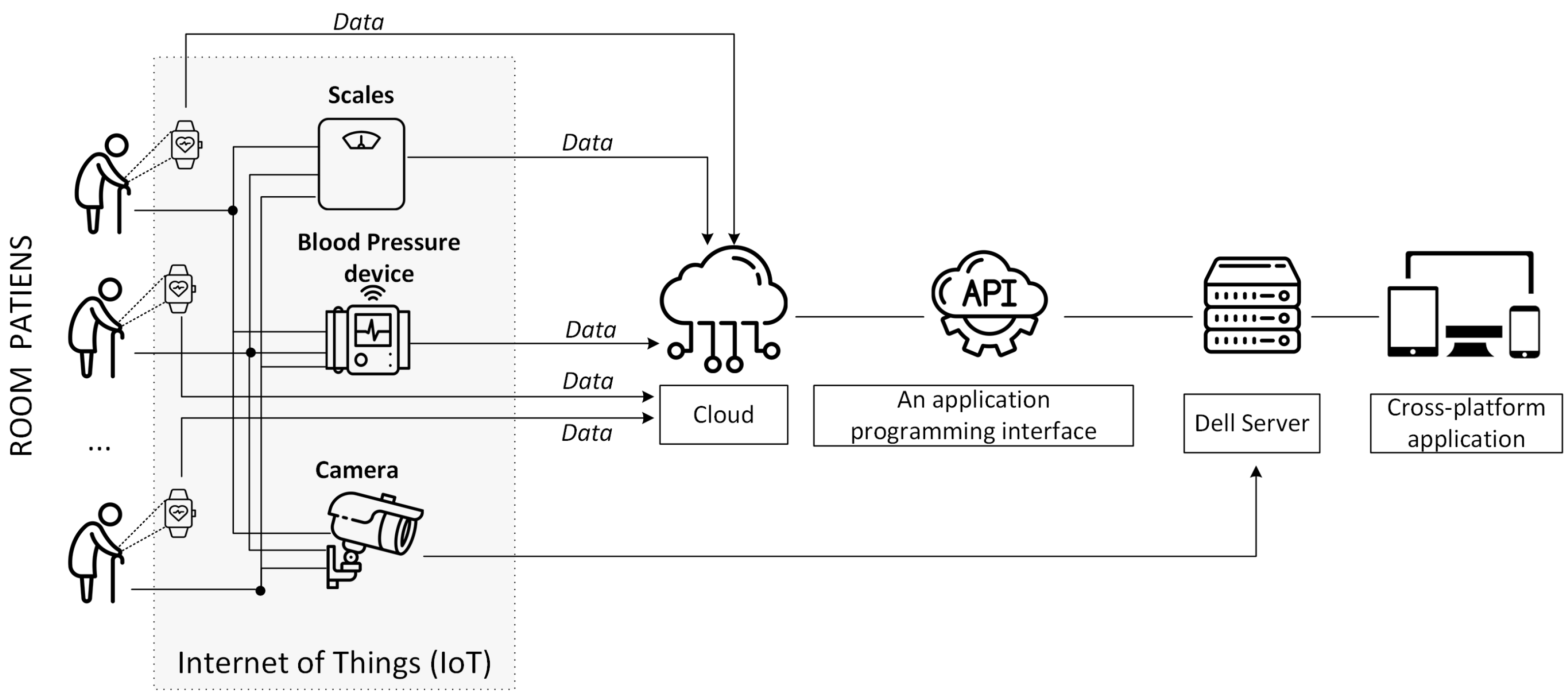
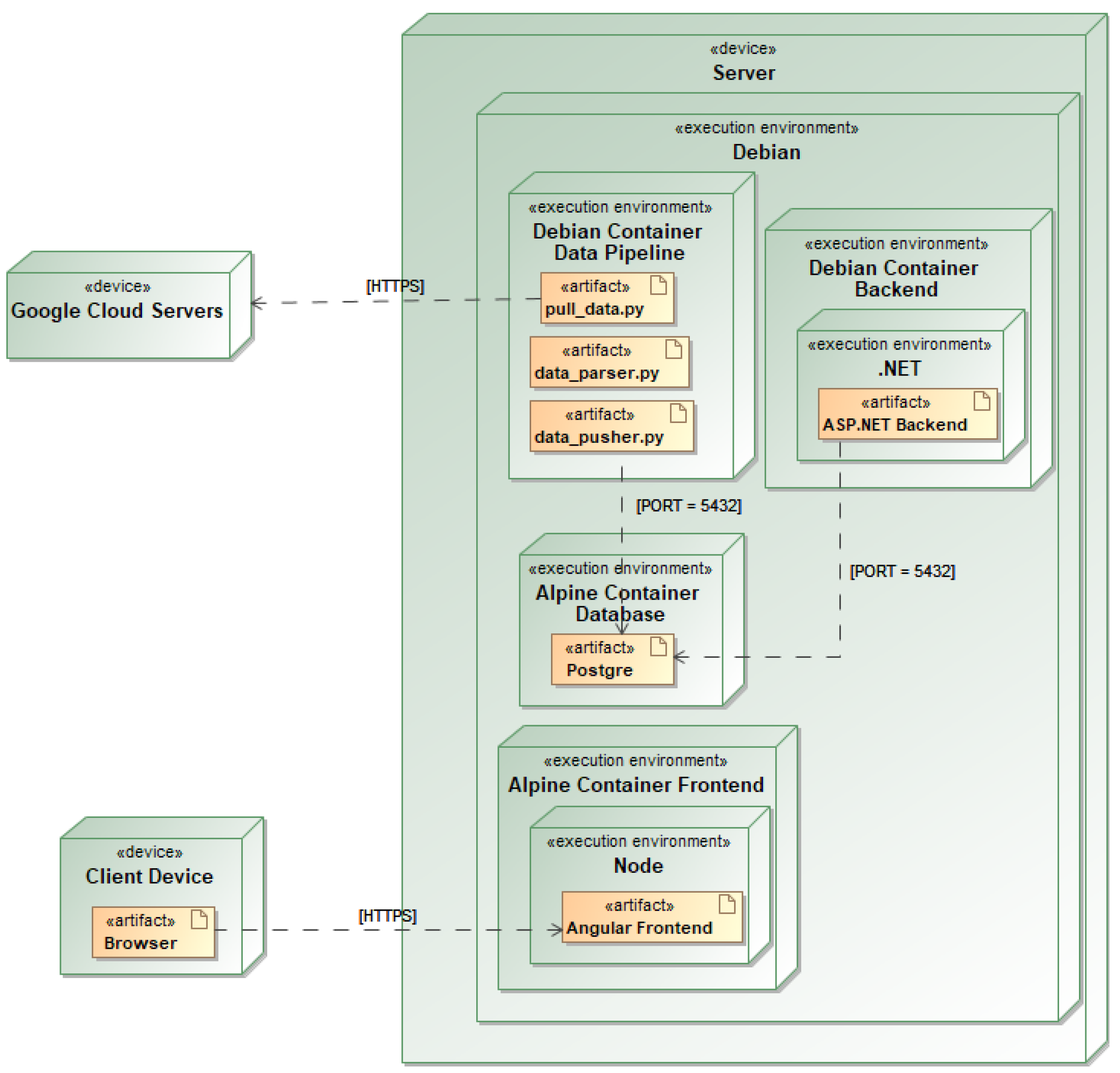
4.1. Implementation of the Geriatric Care System
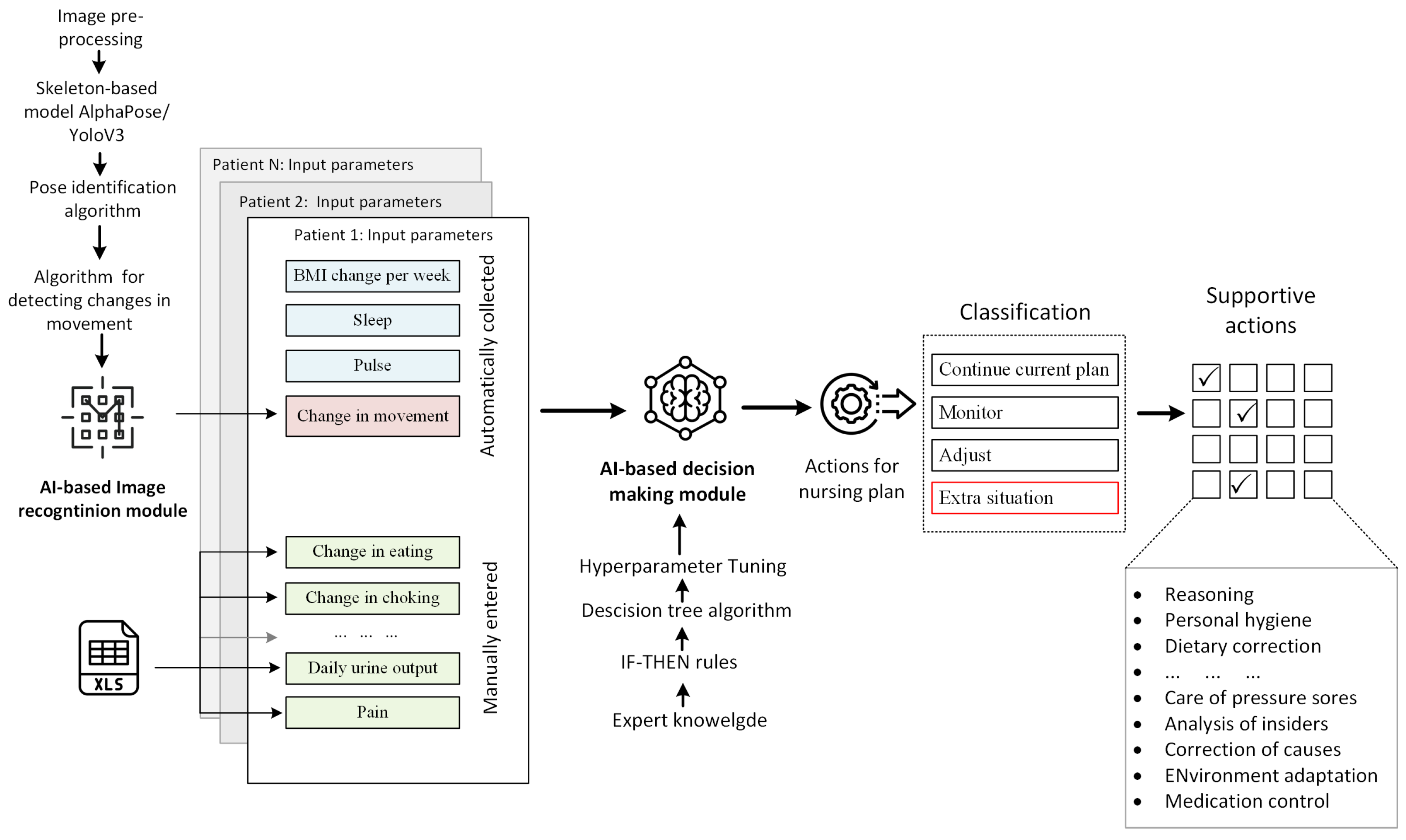
4.2. AI-Based Data Analytics and Decision Making
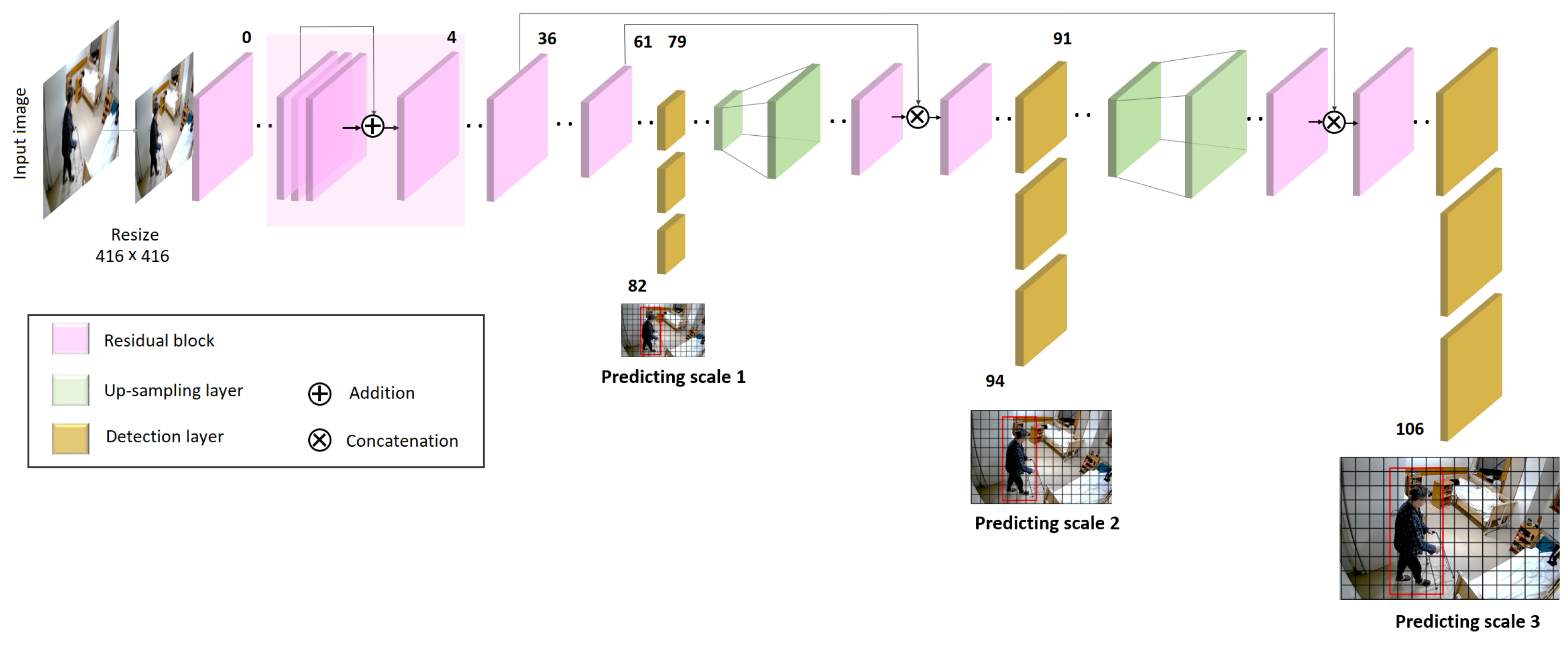
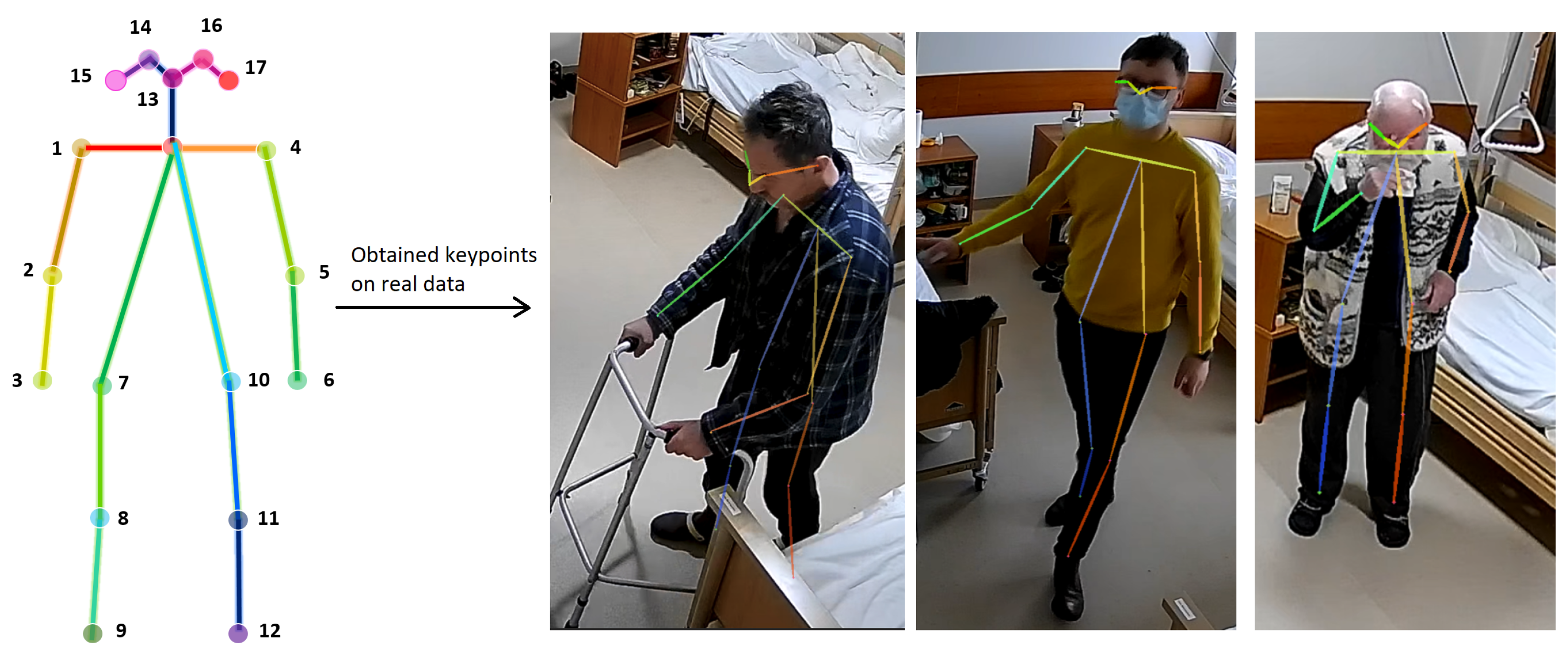
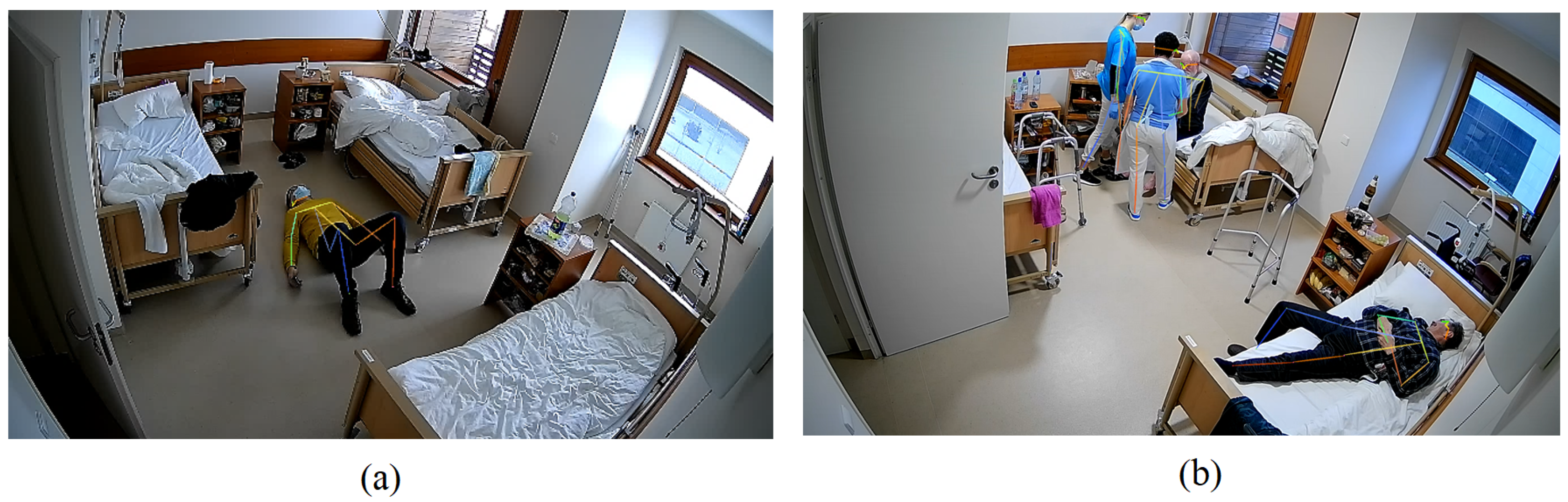
Image Recognition Solution
- Brightening: to increase the overall luminosity of the image, improve visibility, and increase the clarity of the image during low light conditions;
- Cropping: to keep only regions of interest in the image;
- Denoising: to remove noise from the image, typically by applying a low-pass filter. It also improved the quality and clarity of the image by removing noise, which could be especially useful if the image was taken under poor conditions or with a low-quality camera.
- Edge detection: to identify edges in the image by finding points of a rapid intensity change. It can also be used to identify and extract features or objects in the image, such as lines, shapes, or boundaries.
| Algorithm 1 Evaluation of changes in movement habits |
|
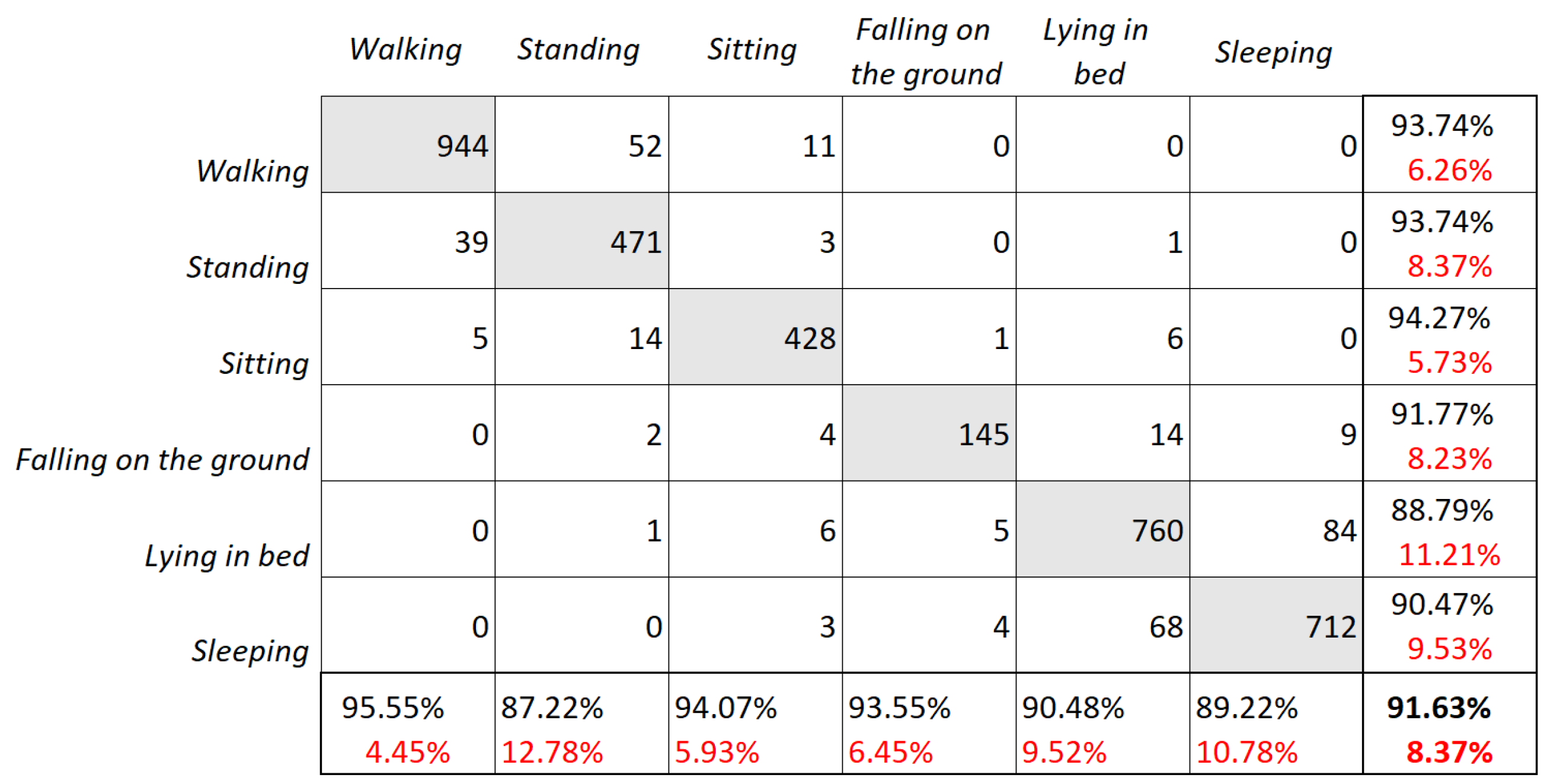
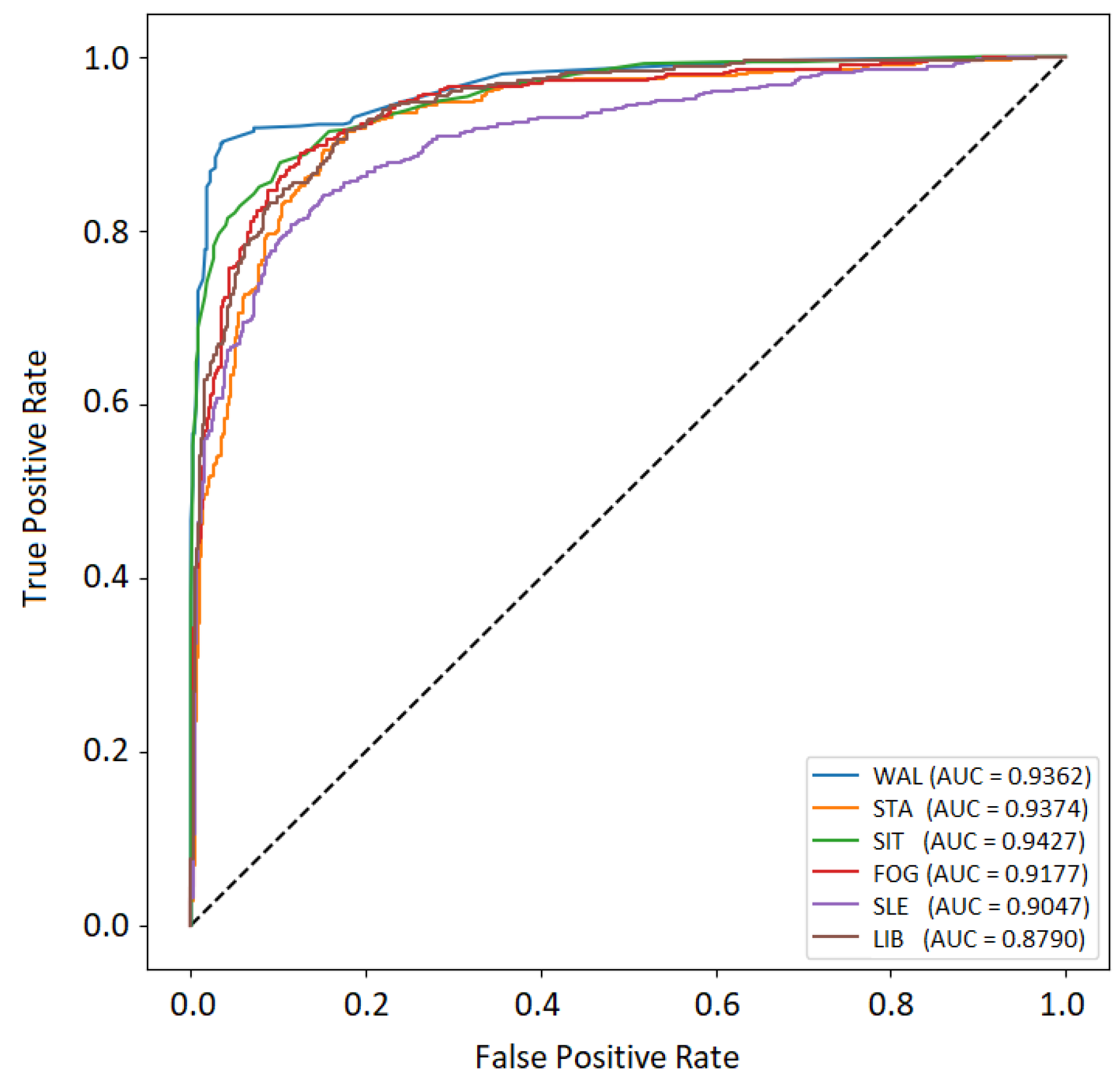
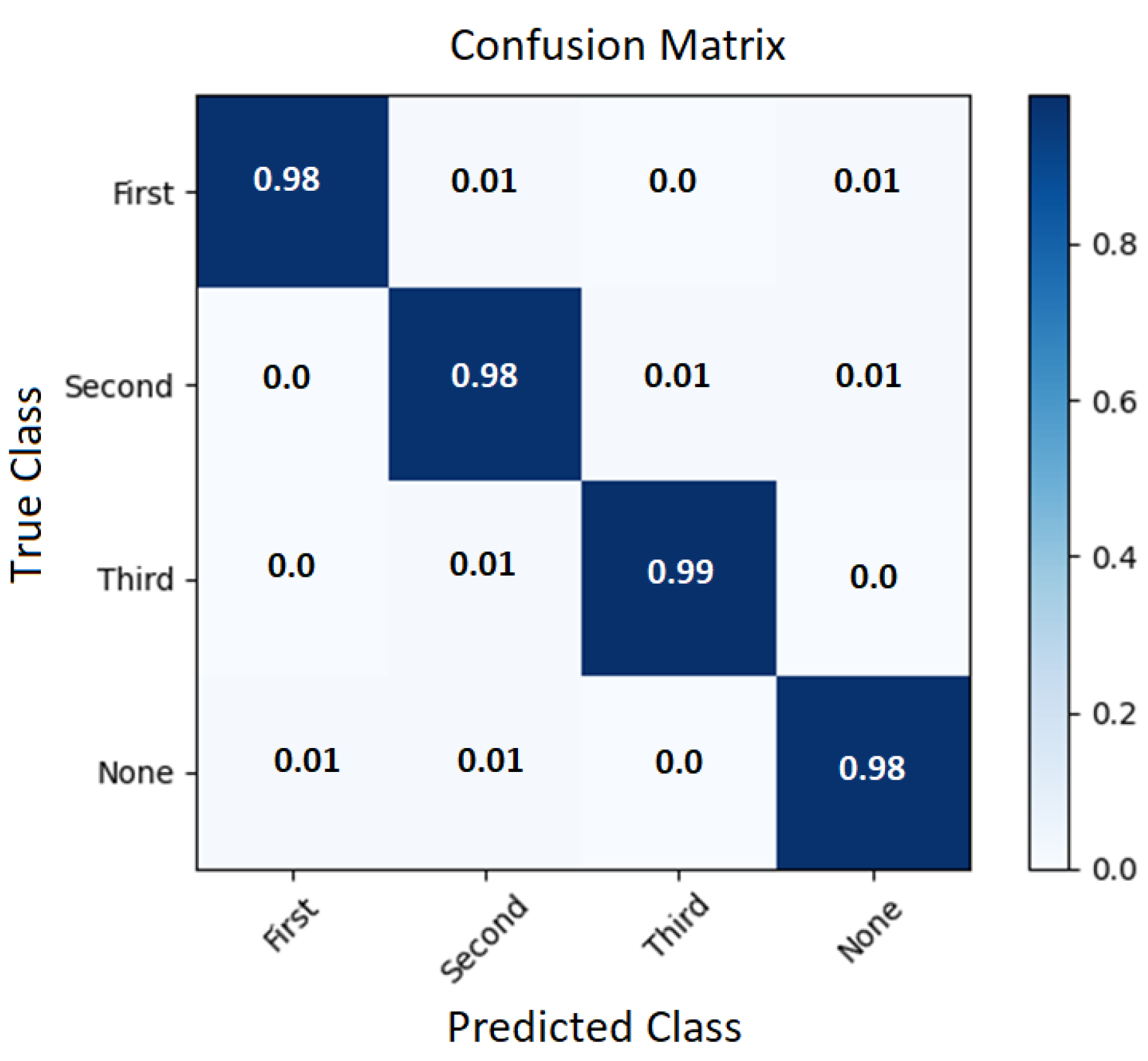
4.3. Experimental Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellis, G.; Sevdalis, N. Understanding and improving multidisciplinary team working in geriatric medicine. Age Ageing 2019, 48, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.N.; Beckett, M.K.; Cohea, C.; Lehrman, W.G.; Russ, C.; Cleary, P.D.; Giordano, L.A.; Goldstein, E.; Saliba, D. The hospital care experiences of older patients compared to younger patients. J. Am. Geriatr. Soc. 2022, 70, 3570–3577. [Google Scholar] [CrossRef] [PubMed]
- Reber, K.C.; Lindlbauer, I.; Schulz, C.; Rapp, K.; König, H.H. Impact of morbidity on care need increase and mortality in nursing homes: A retrospective longitudinal study using administrative claims data. BMC Geriatr. 2020, 20, 439. [Google Scholar] [CrossRef] [PubMed]
- Dall’Ora, C.; Griffiths, P.; Hope, J.; Briggs, J.; Jeremy, J.; Gerry, S.; Redfern, O. How long do nursing staff take to measure and record patients’ vital signs observations in hospital? A time-and-motion study. Int. J. Nurs. Stud. 2021, 118, 103921. [Google Scholar] [CrossRef] [PubMed]
- Tang, V.; Choy, K.; Ho, G.; Lam, H.; Tsang, Y.P. An IoMT-based geriatric care management system for achieving smart health in nursing homes. Ind. Manag. Data Syst. 2019; ahead-of-print. [Google Scholar] [CrossRef]
- Flores-Martin, D.; Rojo, J.; Moguel, E.; Berrocal, J.; Murillo, J.M.; Cai, Z. Smart Nursing Homes: Self-Management Architecture Based on IoT and Machine Learning for Rural Areas. Wirel. Commun. Mob. Comput. 2021, 2021. [Google Scholar] [CrossRef]
- Lu, Z.X.; Qian, P.; Bi, D.; Ye, Z.W.; He, X.; Zhao, Y.H.; Su, L.; Li, S.L.; Zhu, Z.L. Application of AI and IoT in Clinical Medicine: Summary and Challenges. Curr. Med Sci. 2021, 41, 1134–1150. [Google Scholar] [CrossRef] [PubMed]
- Mbunge, E.; Muchemwa, B.; Jiyane, S.; Batani, J. Sensors and healthcare 5.0: Transformative shift in virtual care through emerging digital health technologies. Glob. Health J. 2021, 5, 169–177. [Google Scholar] [CrossRef]
- Khan, M.F.; Ghazal, T.M.; Said, R.A.; Fatima, A.; Abbas, S.; Khan, M.A.; Issa, G.F.; Ahmad, M.; Khan, M.A. An IoMT-Enabled Smart Healthcare Model to Monitor Elderly People Using Machine Learning Technique. Comput. Intell. Neurosci. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Alshamrani, M. IoT and artificial intelligence implementations for remote healthcare monitoring systems: A survey. J. King Saud Univ.—Comput. Inf. Sci. 2022, 34, 4687–4701. [Google Scholar] [CrossRef]
- Ienca, M.; Schneble, C.; Kressig, R.W.; Wangmo, T. Digital health interventions for healthy ageing: A qualitative user evaluation and ethical assessment. BMC Geriatr. 2021, 21, 412. [Google Scholar] [CrossRef]
- Andreoni, G.; Mambrettii, C. Privacy and Security Concerns in IoT-Based Healthcare Systems. In Digital Health Technology for Better Aging; Springer: Cham, Switzerland, 2021; p. 365. [Google Scholar] [CrossRef]
- Kekade, S.; Hseieh, C.H.; Islam, M.M.; Atique, S.; Mohammed Khalfan, A.; Li, Y.C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Programs Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef]
- Chandrasekaran, R.; Katthula, V.; Moustakas, E. Too old for technology? Use of wearable healthcare devices by older adults and their willingness to share health data with providers. Health Inform. J. 2021, 27, 14604582211058073. [Google Scholar] [CrossRef]
- Prieto-Avalos, G.; Cruz-Ramos, N.A.; Alor-Hernández, G.; Sánchez-Cervantes, J.L.; Rodríguez-Mazahua, L.; Guarneros-Nolasco, L.R. Wearable Devices for Physical Monitoring of Heart: A Review. Biosensors 2022, 12, 292. [Google Scholar] [CrossRef]
- Lu, L.; Zhang, J.; Xie, Y.; Gao, F.; Xu, S.; Wu, X.; Ye, Z. Wearable health devices in health care: Narrative systematic review. JMIR mHealth uHealth 2020, 8, e18907. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A.; Cowie, M.R. The Role of Wearables in Heart Failure. Curr. Heart Fail. Rep. 2020, 17, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, M.; Straiton, N.; Gallagher, R. Harnessing the Potential of Wearable Activity Trackers for Heart Failure Self-Care. Curr. Heart Fail. Rep. 2017, 14, 23–29. [Google Scholar] [CrossRef]
- Gresham, G.; Schrack, J.; Gresham, L.M.; Shinde, A.M.; Hendifar, A.E.; Tuli, R.; Rimel, B.; Figlin, R.; Meinert, C.L.; Piantadosi, S. Wearable activity monitors in oncology trials: Current use of an emerging technology. Contemp. Clin. Trials 2018, 64, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Saito, H.; Koike, E.; Nitta, K. A Preliminary Test of Measurement of Joint Angles and Stride Length with Wireless Inertial Sensors for Wearable Gait Evaluation System. Comput. Intell. Neurosci. 2011, 2011, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ryvlin, P.; Ciumas, C.; Wisniewski, I.; Beniczky, S. Wearable devices for sudden unexpected death in epilepsy prevention. Epilepsia 2018, 59 (Suppl. 1), 61–66. [Google Scholar] [CrossRef]
- Takei, K.; Honda, W.; Harada, S.; Arie, T.; Akita, S. Toward flexible and wearable human-interactive health-monitoring devices. Adv. Healthc. Mater. 2015, 4, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Kamei, T.; Kanamori, T.; Yamamoto, Y.; Edirippulige, S. The use of wearable devices in chronic disease management to enhance adherence and improve telehealth outcomes: A systematic review and meta-analysis. J. Telemed. Telecare 2022, 28, 342–359. [Google Scholar] [CrossRef]
- Yu, S.; Chen, Z.; Wu, X. The Impact of Wearable Devices on Physical Activity for Chronic Disease Patients: Findings from the 2019 Health Information National Trends Survey. Int. J. Environ. Res. Public Health 2023, 20, 887. [Google Scholar] [CrossRef] [PubMed]
- Kulurkar, P.; kumar Dixit, C.; Bharathi, V.; Monikavishnuvarthini, A.; Dhakne, A.; Preethi, P. AI based elderly fall prediction system using wearable sensors: A smart home-care technology with IOT. Meas. Sensors 2023, 25, 100614. [Google Scholar] [CrossRef]
- Cudejko, T.; Button, K.; Al-Amri, M. Validity and reliability of accelerations and orientations measured using wearable sensors during functional activities. Sci. Rep. 2022, 12, 14619. [Google Scholar] [CrossRef] [PubMed]
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Heerden, D.V.; Luan, H.; Cullen, K.; et al. Reliability and Validity of Commercially Available Wearable Devices for Measuring Steps, Energy Expenditure, and Heart Rate: Systematic Review. JMIR mHealth uHealth 2020, 8, e18694. [Google Scholar] [CrossRef]
- Patel, V.; Orchanian-Cheff, A.; Wu, R. Evaluating the Validity and Utility of Wearable Technology for Continuously Monitoring Patients in a Hospital Setting: Systematic Review. JMIR mHealth uHealth 2021, 9, e17411. [Google Scholar] [CrossRef]
- Chan, A.; Chan, D.; Lee, H.; Ng, C.C.; Yeo, A.H.L. Reporting adherence, validity and physical activity measures of wearable activity trackers in medical research: A systematic review. Int. J. Med Inform. 2022, 160, 104696. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, E.; Fonseca, H.; Diniz-Sousa, F.; Veras, L.; Boppre, G.; Oliveira, J.; Pinto, D.; Alves, A.J.; Barbosa, A.; Mendes, R.; et al. Wearable Devices for Physical Activity and Healthcare Monitoring in Elderly People: A Critical Review. Geriatrics 2021, 6, 38. [Google Scholar] [CrossRef]
- Moore, K.; O’Shea, E.; Kenny, L.; Barton, J.; Tedesco, S.; Sica, M.; Crowe, C.; Alamaki, A.; Condell, J.; Nordstrom, A.; et al. Older Adults’ Experiences With Using Wearable Devices: Qualitative Systematic Review and Meta-synthesis. JMIR mHealth uHealth 2021, 9, e23832. [Google Scholar] [CrossRef]
- Koerber, D.; Khan, S.; Shamsheri, T.; Kirubarajan, A.; Mehta, S. Accuracy of Heart Rate Measurement with Wrist-Worn Wearable Devices in Various Skin Tones: A Systematic Review. J. Racial Ethn. Health Disparities 2022. [Google Scholar] [CrossRef]
- Ferguson, C.; Hickman, L.D.; Turkmani, S.; Breen, P.; Gargiulo, G.; Inglis, S.C. “Wearables only work on patients that wear them”: Barriers and facilitators to the adoption of wearable cardiac monitoring technologies. Cardiovasc. Digit. Health J. 2021, 2, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersson, A.; Lindén, M. Wearable Sensors for Monitoring and Preventing Noncommunicable Diseases: A Systematic Review. Information 2020, 11, 521. [Google Scholar] [CrossRef]
- Rohmetra, H.; Raghunath, N.; Narang, P.; Chamola, V.; Guizani, M.; Lakkaniga, R. AI-enabled remote monitoring of vital signs for COVID-19: Methods, Prospects and Challenges. Computing 2021, 105, 783–809. [Google Scholar] [CrossRef]
- Guo, K.; Zhai, T.; Purushothama, M.H.; Dobre, A.; Meah, S.; Pashollari, E.; Vaish, A.; DeWilde, C.; Islam, M.N. Contactless Vital Sign Monitoring System for In-Vehicle Driver Monitoring Using a Near-Infrared Time-of-Flight Camera. Appl. Sci. 2022, 12, 4416. [Google Scholar] [CrossRef]
- Guo, K.; Zhai, T.; Pashollari, E.; Varlamos, C.J.; Ahmed, A.; Islam, M.N. Contactless Vital Sign Monitoring System for Heart and Respiratory Rate Measurements with Motion Compensation Using a Near-Infrared Time-of-Flight Camera. Appl. Sci. 2021, 11, 10913. [Google Scholar] [CrossRef]
- Jelinčić, V.; Diest, I.V.; Torta, D.M.; von Leupoldt, A. The breathing brain: The potential of neural oscillations for the understanding of respiratory perception in health and disease. Psychophysiology 2022, 59, e13844. [Google Scholar] [CrossRef] [PubMed]
- Andrea, N.; Carlo, M.; Emiliano, S.; Massimo, S. The Importance of Respiratory Rate Monitoring: From Healthcare to Sport and Exercise. Sensors 2020, 20, 6396. [Google Scholar] [CrossRef]
- Baumert, M.; Linz, D.; Stone, K.; McEvoy, R.D.; Cummings, S.; Redline, S.; Mehra, R.; Immanuel, S. Mean nocturnal respiratory rate predicts cardiovascular and all-cause mortality in community-dwelling older men and women. Eur. Respir. J. 2019, 54, 1802175. [Google Scholar] [CrossRef]
- Fox, H.; Rudolph, V.; Munt, O.; Malouf, G.; Graml, A.; Bitter, T.; Oldenburg, O. Early identification of heart failure deterioration through respiratory monitoring with adaptive servo-ventilation. J. Sleep Res. 2023, 32, e13749. [Google Scholar] [CrossRef]
- Scebba, G.; Da Poian, G.; Karlen, W. Multispectral Video Fusion for Non-Contact Monitoring of Respiratory Rate and Apnea. IEEE Trans. Biomed. Eng. 2021, 68, 350–359. [Google Scholar] [CrossRef]
- Nakagawa, K.; Sankai, Y. Noncontact Vital Sign Monitoring System with Dual Infrared Imaging for Discriminating Respiration Mode. Adv. Biomed. Eng. 2021, 10, 80–89. [Google Scholar] [CrossRef]
- Yacchirema, D.C.; de Puga, J.S.; Palau, C.E.; Esteve, M. Fall detection system for elderly people using IoT and ensemble machine learning algorithm. Pers. Ubiquitous Comput. 2019, 23, 801–817. [Google Scholar] [CrossRef]
- Esmaeili, B.; AkhavanPour, A.; Bosaghzadeh, A. An Ensemble Model For Human Posture Recognition. In Proceedings of the 2020 International Conference on Machine Vision and Image Processing (MVIP), Teheren, Iran, 18–20 February 2020; pp. 1–7. [Google Scholar] [CrossRef]
- Artacho, B.; Savakis, A.E. UniPose: Unified Human Pose Estimation in Single Images and Videos. CoRR 2020, abs/2001.08095. [Google Scholar]
- Insafutdinov, E.; Pishchulin, L.; Andres, B.; Andriluka, M.; Schiele, B. DeeperCut: A Deeper, Stronger, and Faster Multi-Person Pose Estimation Model. CoRR 2016, abs/1605.03170. [Google Scholar]
- Li, J.; Wang, C.; Zhu, H.; Mao, Y.; Fang, H.; Lu, C. CrowdPose: Efficient Crowded Scenes Pose Estimation and a New Benchmark. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, CVPR 2019, Long Beach, CA, USA, 16–20 June 2019; pp. 10863–10872. [Google Scholar] [CrossRef]
- Ouyang, W.; Chu, X.; Wang, X. Multi-source Deep Learning for Human Pose Estimation. In Proceedings of the 2014 IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 2337–2344. [Google Scholar] [CrossRef]
- Moon, G.; Chang, J.; Lee, K.M. PoseFix: Model-Agnostic General Human Pose Refinement Network. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 7765–7773. [Google Scholar] [CrossRef]
- Nie, X.; Feng, J.; Xing, J.; Xiao, S.; Yan, S. Hierarchical Contextual Refinement Networks for Human Pose Estimation. IEEE Trans. Image Process. 2019, 28, 924–936. [Google Scholar] [CrossRef]
- Newell, A.; Yang, K.; Deng, J. Stacked Hourglass Networks for Human Pose Estimation. In Proceedings of the Computer Vision–ECCV 2016, Amsterdam, The Netherlands, 11–14 October 2016; pp. 483–499. [Google Scholar]
- Núñez-Marcos, A.; Azkune, G.; Arganda-Carreras, I. Vision-Based Fall Detection with Convolutional Neural Networks. Wirel. Commun. Mob. Comput. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Xu, C.; Xu, Y.; Xu, Z.; Guo, B.; Zhang, C.; Huang, J.; Deng, X. Fall Detection in Elevator Cages Based on XGBoost and LSTM. In Proceedings of the 2021 26th International Conference on Automation and Computing (ICAC), Portsmouth, UK, 2–4 September 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Ren, X.; Zhang, Y.; Yang, Y. Human Fall Detection Model with Lightweight Network and Tracking in Video. In Proceedings of the 2021 5th International Conference on Computer Science and Artificial Intelligence, CSAI 2021, Beijing, China, 4–6 December 2021; pp. 1–7. [Google Scholar] [CrossRef]
- De Miguel, K.; Brunete, A.; Hernando, M.; Gambao, E. Home Camera-Based Fall Detection System for the Elderly. Sensors 2017, 17, 2864. [Google Scholar] [CrossRef]
- Sadreazami, H.; Bolic, M.; Rajan, S. Contactless Fall Detection Using Time-Frequency Analysis and Convolutional Neural Networks. IEEE Trans. Ind. Informatics 2021, 17, 6842–6851. [Google Scholar] [CrossRef]
- Butt, F.S.; La Blunda, L.; Wagner, M.F.; Schafer, J.; Medina-Bulo, I.; Gomez-Ullate, D. Fall Detection from Electrocardiogram (ECG) Signals and Classification by Deep Transfer Learning. Information 2021, 12, 63. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Vaughan, R. Deep Learning Radar Design for Breathing and Fall Detection. IEEE Sensors J. 2020, 20, 5072–5085. [Google Scholar] [CrossRef]
- Martinez-Martin, N.; Luo, Z.; Kaushal, A.; Adeli, E.; Haque, A.; Kelly, S.S.; Wieten, S.; Cho, M.K.; Magnus, D.; Fei-Fei, L.; et al. Ethical issues in using ambient intelligence in health-care settings. Lancet Digit. Health 2021, 3, e115–e123. [Google Scholar] [CrossRef]
- Esteva, A.; Chou, K.; Yeung, S.; Naik, N.; Madani, A.; Mottaghi, A.; Liu, Y.; Topol, E.; Dean, J.; Socher, R. Deep learning-enabled medical computer vision. NPJ Digit. Med. 2021, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Babar, M.; Rahman, A.; Arif, F.; Jeon, G. Energy-harvesting based on internet of things and big data analytics for smart health monitoring. Sustain. Comput. Inform. Syst. 2018, 20, 155–164. [Google Scholar] [CrossRef]
- Syed, L.; Jabeen, S.; Manimala, S.; Elsayed, H.A. Data Science Algorithms and Techniques for Smart Healthcare Using IoT and Big Data Analytics. In Smart Techniques for a Smarter Planet: Towards Smarter Algorithms; Springer International Publishing: Cham, Switzerland, 2019; pp. 211–241. [Google Scholar] [CrossRef]
- Tawalbeh, L.; Muheidat, F.; Tawalbeh, M.; Quwaider, M. IoT Privacy and Security: Challenges and Solutions. Appl. Sci. 2020, 10, 4102. [Google Scholar] [CrossRef]
- Awotunde, J.B.; Jimoh, R.G.; Folorunso, S.O.; Adeniyi, E.A.; Abiodun, K.M.; Banjo, O.O. Privacy and Security Concerns in IoT-Based Healthcare Systems. In The Fusion of Internet of Things, Artificial Intelligence, and Cloud Computing in Health Care; Springer International Publishing: Cham, Switzerland, 2021; pp. 105–134. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. YOLOv3: An Incremental Improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.S.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Pan, C.; Cao, H.; Zhang, W.; Song, X.; Li, M. Driver activity recognition using spatial-temporal graph convolutional LSTM networks with attention mechanism. IET Intell. Transp. Syst. 2020, 15, 297–307. [Google Scholar] [CrossRef]
- Vasconez, J.; Admoni, H.; Cheein, F.A. A methodology for semantic action recognition based on pose and human-object interaction in avocado harvesting processes. Comput. Electron. Agric. 2021, 184, 106057. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, X. Bed-Leaving Action Recognition Based on YOLOv3 and AlphaPose. In Proceedings of the 2022 the 5th International Conference on Image and Graphics Processing (ICIGP), ICIGP 2022, Beijing, China, 7–9 January 2022; pp. 117–123. [Google Scholar] [CrossRef]
- Zhao, X.; Hou, F.; Su, J.; Davis, L. An Alphapose-Based Pedestrian Fall Detection Algorithm. In Proceedings of the Artificial Intelligence and Security, Qinghai, China, 15–20 July 2022; pp. 650–660. [Google Scholar]
- Cortés, X.; Conte, D.; Cardot, H. A new bag of visual words encoding method for human action recognition. In Proceedings of the 2018 24th International Conference on Pattern Recognition (ICPR), Beijing, China, 20–24 August 2018; pp. 2480–2485. [Google Scholar] [CrossRef]
- Aslan, M.; Durdu, A.; Sabanci, K. Human action recognition with bag of visual words using different machine learning methods and hyperparameter optimization. Neural Comput. Appl. 2020, 32, 8585–8597. [Google Scholar] [CrossRef]
- Nazir, S.; Yousaf, M.H.; Velastin, S.A. Evaluating a bag-of-visual features approach using spatio-temporal features for action recognition. Comput. Electr. Eng. 2018, 72, 660–669. [Google Scholar] [CrossRef]
- Fang, H.S.; Li, J.; Tang, H.; Xu, C.; Zhu, H.; Xiu, Y.; Li, Y.L.; Lu, C. AlphaPose: Whole-Body Regional Multi-Person Pose Estimation and Tracking in Real-Time. arXiv 2022, arXiv:2211.03375. [Google Scholar] [CrossRef]
- Fang, H.S.; Xie, S.; Tai, Y.W.; Lu, C. RMPE: Regional Multi-person Pose Estimation. arXiv 2016, arXiv:1612.00137. [Google Scholar] [CrossRef]
- Wan, C.; Wang, L.; Phoha, V.V. A Survey on Gait Recognition. ACM Comput. Surv. 2018, 51, 1–35. [Google Scholar] [CrossRef]
- Semwal, V.B.; Mazumdar, A.; Jha, A.; Gaud, N.; Bijalwan, V. Speed, Cloth and Pose Invariant Gait Recognition-Based Person Identification. In Machine Learning: Theoretical Foundations and Practical Applications; Springer Singapore: Singapore, 2021; pp. 39–56. [Google Scholar] [CrossRef]
- Elharrouss, O.; Almaadeed, N.; Al-ma’adeed, S.; Bouridane, A. Gait recognition for person re-identification. J. Supercomput. 2021, 77, 3653–3672. [Google Scholar] [CrossRef]
- Sun, F.; Zang, W.; Gravina, R.; Fortino, G.; Li, Y. Gait-based identification for elderly users in wearable healthcare systems. Inf. Fusion 2020, 53, 134–144. [Google Scholar] [CrossRef]
- Liu, X.; Zhao, C.; Zheng, B.; Guo, Q.; Duan, X.; Wulamu, A.; Zhang, D. Wearable Devices for Gait Analysis in Intelligent Healthcare. Front. Comput. Sci. 2021, 3, 661676. [Google Scholar] [CrossRef]
- Zhao, A.; Li, J.; Dong, J.; Qi, L.; Zhang, Q.; Li, N.; Wang, X.; Zhou, H. Multimodal Gait Recognition for Neurodegenerative Diseases. IEEE Trans. Cybern. 2022, 52, 9439–9453. [Google Scholar] [CrossRef]
- Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.; Warmerdam, E.; Sünkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D.; et al. Gait analysis with wearables predicts conversion to Parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Rucco, R.; Agosti, V.; Jacini, F.; Sorrentino, P.; Varriale, P.; De Stefano, M.; Milan, G.; Montella, P.; Sorrentino, G. Spatio-temporal and kinematic gait analysis in patients with Frontotemporal dementia and Alzheimer’s disease through 3D motion capture. Gait Posture 2017, 52, 312–317. [Google Scholar] [CrossRef]
- de Oliveira Silva, F.; Ferreira, J.V.; Plácido, J.; Chagas, D.; Praxedes, J.; Guimarães, C.; Batista, L.A.; Laks, J.; Deslandes, A.C. Gait analysis with videogrammetry can differentiate healthy elderly, mild cognitive impairment, and Alzheimer’s disease: A cross-sectional study. Exp. Gerontol. 2020, 131, 110816. [Google Scholar] [CrossRef]
- Yamada, H.; Ahn, J.; Mozos, O.; Iwashita, Y.; Kurazume, R. Gait-based person identification using 3D LiDAR and long short-term memory deep networks. Adv. Robot. 2020, 34, 1201–1211. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IoT Device Type | Device Name |
|---|---|
| Camera | EZVIZ CS-C3TN 1920 × 1080 |
| Wrist band | Fitbit Charge 5 |
| Blood Pressure | Withings BPM Connect |
| Scales | Withings Body+ |
| No | Variable | Definition | Instances of Possible Values/Range |
|---|---|---|---|
| 1 | FN | First name | - |
| 2 | LN | Last name | - |
| 3 | BD | Birth date | yyyy/mm/dd |
| 4 | HE | Height | 1.20 m–2.20 m |
| Input data | |||
| 1 | MoveC | Movement capabilities | Lying; sitting in a wheelchair; with assistive devices; etc. |
| 2 | RiskC | Risk of collapse | None; low; medium; high |
| 3 | Bedsores | Bedsores | Yes; no |
| 4 | Diseases | All patient’s diseases | Heart failure; Alzheimer; dementia; Cancer; etc. |
| 5 | Med | Taken medications | Antibiotics; antihypertensives; antidepressants; etc. |
| 6 | BMI | BMI unit change per week | <0.5 plus; <0.5 minus; 0.5–1 plus; etc. |
| 7 | MoveH | Movement habits | Unchanged; slowed down; increased; falling on the ground |
| 8 | EatH | Eating habits | Parenteral nutrition; fed by another person; independent eating; etc. |
| 9 | EatC | Eating capabilities | Swallows solid food; swallows only mashed food; swallows only liquids; etc. |
| 10 | Bowel | Bowel habits | Regular bowel movements; diarrhoea; constipation; faecal incontinence |
| 11 | Sleep | Sleeping | <4 h; 4–6 h; 6–8 h; >8 h; apnoea |
| 12 | Breath | Breathing | Increased; slowing down; with apnoeas |
| 13 | PL | Pulse | Normal; bradycardia; tachycardia |
| 14 | BP | Blood Pressure | Normotension; hypotension; hypertension mild; hypertension moderate; hypertension severe; etc. |
| 15 | Temp | Temperature | <36.0 °C; 36.0–37.4 °C; etc. |
| 16 | Sat | Saturation | ≥94%; <94% |
| 17 | Urine | Daily urine output | Concentrated urine; very frequent; etc. |
| 18 | Fluid | Fluid tracking | <500 mL; ≥500 mL |
| 19 | Gly | Glycaemia | <2.5 mmol/l; ≥2.5 mmol/l |
| 20 | Con | Consciousness | Unchanged; changed; unconscious |
| 21 | Pain | Perceived level of pain | None; mild; moderate; severe; unbearable |
| Output data | |||
| 1 | Plan | Nursing plan | Continue current plan; monitor; adjust; extra situation |
| Class | Precision | Recall | F1 Score |
|---|---|---|---|
| Walking (WAL) | 0.9554 | 0.9374 | 0.9463 |
| Standing (STA) | 0.8722 | 0.9163 | 0.8937 |
| Sitting (SIT) | 0.9406 | 0.9427 | 0.9416 |
| Fallen on the ground (FOG) | 0.9354 | 0.8333 | 0.8814 |
| Lying in bed (LIB) | 0.8951 | 0.8878 | 0.8914 |
| Sleeping (SLE) | 0.8844 | 0.9047 | 0.8944 |
| Macro F1 score | 0.9082 | ||
| Weighted F1 score | 0.9125 | ||
| No. | Actual Pose | Predicted Pose | Ambient Lighting | Confidence |
|---|---|---|---|---|
| 1 | Walking | Walking | Day time (well-lit) | 98.0% |
| 2 | Sitting | Sitting | Day time (well-lit) | 97.5% |
| 3 | Sitting | Sitting | Day time (well-lit) | 98.2% |
| 4 | Lying in bed | Sleeping | Night time (poorly lit) | 89.3% |
| 5 | Standing | Standing | Day time (perfect) | 99.7% |
| 6 | Lying in bed | Lying in bed | Evening time (semi-lit) | 87.9% |
| 7 | Sleeping | Lying in bed | Evening time (semi-lit) | 88.6% |
| 8 | Standing | Standing | Day time (perfect) | 99.1% |
| 9 | Sleeping | Sleeping | Night time (poorly lit) | 85.4% |
| 10 | Walking | Walking | Day time (perfect) | 93.6% |
| 11 | Lying in bed | Lying in bed | Day time (perfect) | 94.2% |
| 12 | Standing | Standing | Day time (perfect) | 99.3% |
| 13 | Walking | Walking | Night time (poorly lit) | 96.0% |
| 14 | Sitting | Sitting | Day time (perfect) | 98.5% |
| 15 | Sleeping | Sleeping | Day time (perfect) | 91.0% |
| 16 | Fallen on the ground | Fallen on the ground | Day time (perfect) | 99.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulauskaite-Taraseviciene, A.; Siaulys, J.; Sutiene, K.; Petravicius, T.; Navickas, S.; Oliandra, M.; Rapalis, A.; Balciunas, J. Geriatric Care Management System Powered by the IoT and Computer Vision Techniques. Healthcare 2023, 11, 1152. https://doi.org/10.3390/healthcare11081152
Paulauskaite-Taraseviciene A, Siaulys J, Sutiene K, Petravicius T, Navickas S, Oliandra M, Rapalis A, Balciunas J. Geriatric Care Management System Powered by the IoT and Computer Vision Techniques. Healthcare. 2023; 11(8):1152. https://doi.org/10.3390/healthcare11081152
Chicago/Turabian StylePaulauskaite-Taraseviciene, Agne, Julius Siaulys, Kristina Sutiene, Titas Petravicius, Skirmantas Navickas, Marius Oliandra, Andrius Rapalis, and Justinas Balciunas. 2023. "Geriatric Care Management System Powered by the IoT and Computer Vision Techniques" Healthcare 11, no. 8: 1152. https://doi.org/10.3390/healthcare11081152