
The Relationship of Nurse and Physician Staffing in Intensive Care Units with Patient Outcomes in Postoperative Patients on Ventilators: An Analysis Using Korean National Health Insurance Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Data
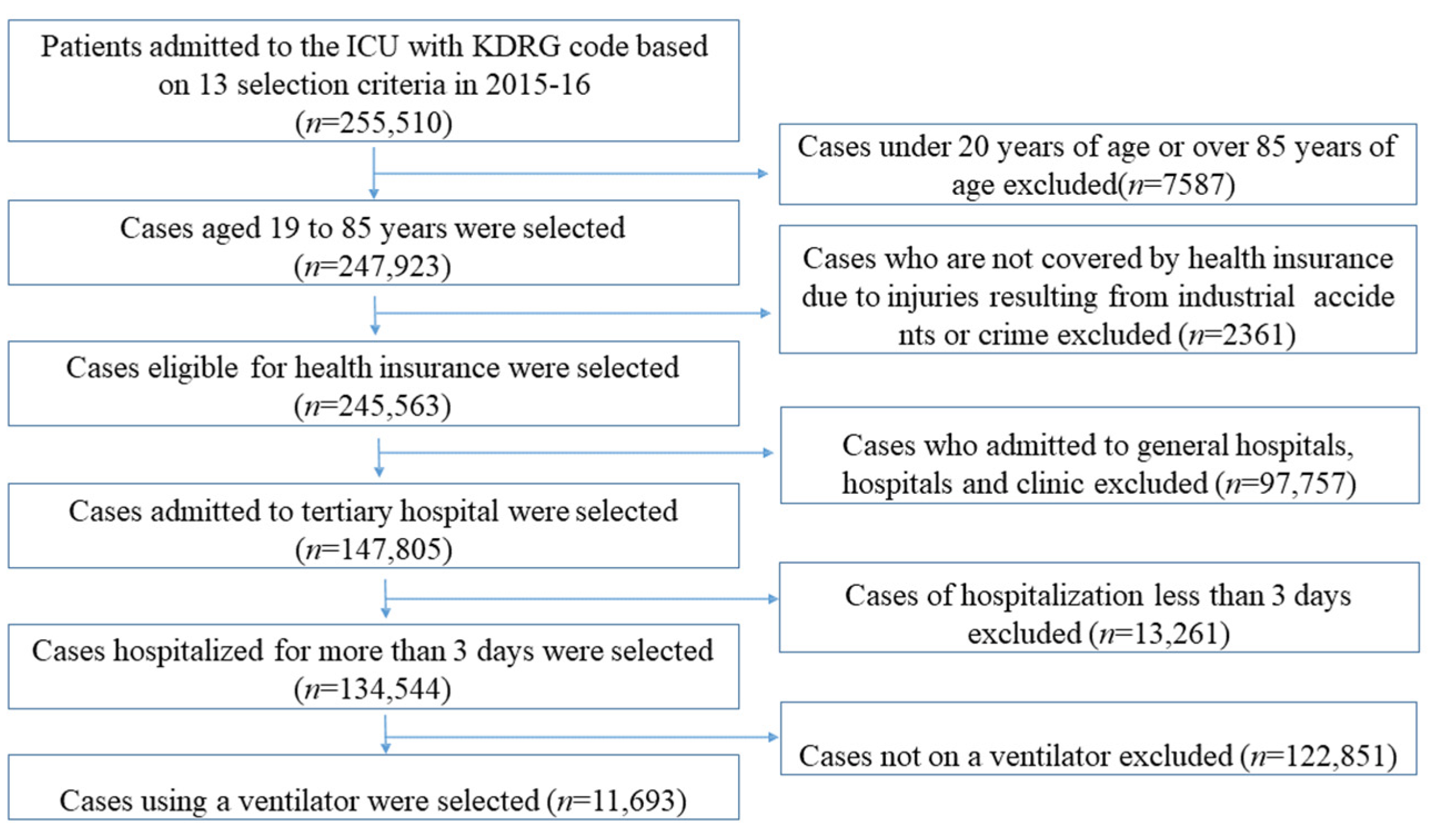
2.2. Study Participants
2.3. Measurement
2.3.1. Hospital Characteristics
2.3.2. Patient Characteristics
2.4. Data Analysis
2.5. Ethics Statement
3. Results
3.1. Patient and Hospital Characteristics
3.2. Univariate Analysis of HAP and In-Hospital Mortality According to Hospital Characteristics
3.3. Univariate Analysis of HAP and In-Hospital Mortality According to Patient Characteristics
3.4. Relationships of Nurse and Physician Staffing with HAP and In-Hospital Mortality after Adjusting for Patient and Hospital Characteristics
4. Discussion
Limitations and Suggestions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pileggi, C.; Mascaro, V.; Bianco, A.; Nobile, C.G.; Pavia, M. Ventilator bundle and its effects on mortality among ICU patients: A meta-analysis. Crit. Care Med. 2018, 46, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Jeon, K.; Chung, C.R.; Yang, J.H.; Cho, Y.H.; Cho, J.; Suh, G.Y. A nationwide analysis of intensive care unit admissions, 2009–2014–The Korean ICU National Data (KIND) study. J. Crit. Care 2018, 44, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Esper, A.M.; Arabi, Y.M.; Cecconi, M.; Du, B.; Giamarellos-Bourboulis, E.J.; Juffermans, N.; Martin, G.S. Systematized and efficient: Organization of critical care in the future. Crit. Care 2022, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.M.; Kwak, S.H.; Suh, G.Y.; Koh, Y. Critical care in Korea: Present and future. J. Korean Med. Sci. 2015, 30, 1540–1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, E.; Barron, D.N.; Harrison, D.; Rafferty, A.M.; Rowan, K.; Sanderson, C. Nurse staffing, medical staffing and mortality in intensive care: An observational study. Int. J. Nurs. Stud. 2014, 51, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Na, J.I. A Report on the Calculation of the Appropriate Hospital Admission Charges in the Intensive Care Unit; Korean Institute of Hospital Management: Seoul, Republic of Korea, 2014; pp. 1–106. [Google Scholar]
- Numata, Y.; Schulzer, M.; van der Wal, R.; Globerman, J.; Semeniuk, P.; Balka, E.; Fitzgerald, J.M. Nurse staffing levels and hospital mortality in critical care settings: Literature review and meta-analysis. J. Adv. Nurs. 2006, 55, 435–448. [Google Scholar] [CrossRef]
- West, E.; Mays, N.; Rafferty, A.M.; Rowan, K.; Sanderson, C. Nursing resources and patient outcomes in intensive care: A systematic review of the literature. Int. J. Nurs. Stud. 2009, 46, 993–1011. [Google Scholar] [CrossRef]
- Penoyer, D.A. Nurse staffing and patient outcomes in critical care: A concise review. Crit. Care Med. 2010, 38, 1521–1528. [Google Scholar] [CrossRef]
- Cho, S.H.; Hwang, J.H.; Kim, J. Nurse staffing and patient mortality in intensive care units. Nurs. Res. 2008, 57, 322–330. [Google Scholar] [CrossRef]
- Rae, P.J.; Pearce, S.; Greaves, P.J.; Dall’Ora, C.; Griffiths, P.; Endacott, R. Outcomes sensitive to critical care nurse staffing levels: A systematic review. Intensive Crit. Care Nurs. 2021, 67, 103110. [Google Scholar] [CrossRef]
- Jansson, M.M.; Syrjälä, H.P.; Ala-Kokko, T.I. Association of nurse staffing and nursing workload with ventilator-associated pneumonia and mortality: A prospective, single-center cohort study. J. Hosp. Infect. 2019, 101, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.H.; Kim, Y.S.; Park, E.C.; Lee, S.H.; Hong, J.H.; Kim, D.W. A Report on Analysis of Factors Related to the Status of Hospitalized Patients in the Intensive Care Unit, Medical Use, Survival Rate, and Prognosis Using National Health Insurance Data; National Health Insurance Service Ilsan Hospital: Goyang, Republic of Korea, 2017; pp. 1–56. [Google Scholar]
- Kim, E.J.; Kwak, Y.G.; Kim, T.H.; Lee, M.S.; Lee, S.O.; Kim, S.R.; Kim, M.N. Korean National Healthcare-associated Infections Surveillance System, intensive care unit module report: Summary of data from July 2017 through June 2018. Korean J. Healthc. Assoc. Infect. Control. Prev. 2019, 24, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Saied, W.I.; Mourvillier, B.; Cohen, Y.; Ruckly, S.; Reignier, J.; Marcotte, G.; OUTCOMEREA Study Group. A comparison of the mortality risk associated with ventilator-acquired bacterial pneumonia and nonventilator ICU-acquired bacterial pneumonia. Crit. Care Med. 2019, 47, 345–352. [Google Scholar] [CrossRef]
- Chastre, J.; Fagon, J.Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Safdar, N.; Dezfulian, C.; Collard, H.R.; Saint, S. Clinical and economic consequences of ventilator-associated pneumonia: A systematic review. Crit. Care Med. 2005, 33, 2184–2193. [Google Scholar] [CrossRef] [PubMed]
- Muscedere, J.G.; Day, A.; Heyland1, D.K. Mortality, attributable mortality, and clinical events as end points for clinical trials of ventilator-associated pneumonia and hospital-acquired pneumonia. Clin. Infect. Dis. 2010, 51 (Suppl. 1), S120–S125. [Google Scholar] [CrossRef]
- Kwak, S.H.; Jeong, C.W.; Lee, S.H.; Lee, H.J.; Koh, Y. Current status of intensive care units registered as critical care subspecialty training hospitals in Korea. J. Korean Med. Sci. 2014, 29, 431–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, K.; Wren, I.; Baldwin, A.; St Ledger, U.; Gibson, V.; Goodman, S.; Walsh, D. Standards for nurse staffing in critical care units determined by: The British Association of Critical Care Nurses, The Critical Care Networks National Nurse Leads, Royal College of Nursing Critical Care and In-flight Forum. Nurs. Crit. Care 2010, 15, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Serratt, T. California’s Nurse-to-Patient Ratios, Part 1. J. Nurs. Adm. 2013, 43, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Australian Nursing, Midwifery Federation Vitoria Branch. Nurse/Midwife Patient Ratios. It’s a Matter of Saving Lives. 2016. Available online: https://www.anmfvic.asn.au/~/media/f06f12244fbb4522af619e1d5304d71d (accessed on 3 March 2023).
- Ministry of Health and Welfare Notice, No. 2015-145. 2015. Available online: http://www.hira.or.kr/bbsDummy.do?brdBltNo=5756&brdScnBltNo=4&pgmid=HIRAA020002000100 (accessed on 3 March 2023).
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.H.; Lee, J.Y.; June, K.J.; Hong, K.J.; Kim, Y. Nurse staffing levels and proportion of hospitals and clinics meeting the legal standard for nurse staffing for 1996~2013. J. Korean Acad. Nurs. Adm. 2016, 22, 209–219. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.H. Comorbidity adjustment in health insurance claim database. Health Policy Manag. 2016, 26, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Ma, X.; Gao, S.; Li, Q.; Luo, H.; Sun, J.; Liu, D. Association between hospital and ICU structural factors and patient outcomes in China: A secondary analysis of the National Clinical Improvement System Data in 2019. Crit. Care 2022, 26, 24. [Google Scholar] [CrossRef] [PubMed]
- The Korean Society of Critical Care Medicine. 2020 Domestic ICU Status Survey Report; The Korean Society of Critical Care Medicine: Seoul, Republic of Korean, 2020; Available online: https://www.ksccm.org/html/?pmode=BBBS0006700008&page=1&smode=view&seq=2225&searchValue=&searchTitle=strTitle (accessed on 3 March 2023).
- Law, A.C.; Stevens, J.P.; Hohmann, S.; Walkey, A.J. Patient outcomes after the introduction of statewide intensive care unit nurse staffing regulations. Crit. Care Med. 2018, 46, 1563–1569. [Google Scholar] [CrossRef]
- Young, M.P.; Birkmeyer, J.D. Potential reduction in mortality rates using an intensivist model to manage intensive care units. Eff. Clin. Pract. 2000, 3, 284–289. [Google Scholar]
- Faculty of Intensive Care Medicine, Intensive Care Society. Guidelines for the Provision of Intensive Care Services. 2019. Available online: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/gpics-v2.pdf (accessed on 3 March 2023).


{kind=link}
| ICU Nurse Staffing Grade | Nurse Staffing Level (Nurse-to-Bed Ratio) | Nurse-to-Patient Ratio † | Estimated Number of Patients per Shift Working Nurse ‡ | ICU Nursing Management Fee Criteria (2015) |
|---|---|---|---|---|
| 1 | <0.5:1 | <0.47 | <2.64 | 1.45 times the standard |
| 2 | <0.63:1 | <0.59 | <3.02 | 1.3 times the standard |
| 3 | <0.77:1 | <0.73 | <3.70 | 1.15 times the standard |
| 4 | <0.88:1 | <0.83 | <4.22 | Standard fee |
| 5 | ≥0.88:1 | ≥0.83 | ≥4.22 | 0.85 times the standard |
| Variable | Category | Hospital (n = 43) | Patient (n = 11,693) |
|---|---|---|---|
| n (%) | n (%) | ||
| Hospital ownership | Public | 10 (23.3) | 3708 (31.7) |
| Educational foundation | 29 (67.4) | 5492 (47.0) | |
| Medical corporation | 4 (9.3) | 2493 (21.3) | |
| Location | Seoul | 14 (32.6) | 6209 (53.1) |
| Metropolitan cities | 15 (34.9) | 2452 (21.0) | |
| Other regions | 14 (32.6) | 3032 (25.9) | |
| Number of adult ICU beds | <50 | 14 (32.6) | 1862 (15.9) |
| 50–69 | 18 (41.9) | 2399 (20.5) | |
| 70–119 | 8 (18.6) | 3975 (34.0) | |
| ≥120 | 3 (7.0) | 3457 (29.6) | |
| Dedicated resident in ICU | No | 24 (55.8) | 6580 (56.3) |
| Yes | 19 (44.2) | 5113 (43.7) | |
| Dedicated specialist in ICU | No | 24 (55.8) | 7385 (63.2) |
| Yes | 19 (44.2) | 4309 (36.9) | |
| Nurse staffing level in ICU | Grade 1 | 10 (23.3) | 6896 (59.0) |
| Grade 2 | 27 (62.8) | 4052 (34.7) | |
| Grade 3 and higher | 6 (14.0) | 745 (6.4) |
| Variable | Category | n (%) |
|---|---|---|
| Age | 20–49 | 2138 (18.3) |
| 50–59 | 2832 (24.2) | |
| 60–69 | 3074 (26.3) | |
| 70–85 | 3649 (31.2) | |
| Sex | Male | 6990 (59.8) |
| Female | 4703 (40.2) | |
| Korean Diagnosis-Related Group | Major craniotomy (excluding trauma) | 3353 (28.7) |
| Other type of craniotomy (excluding trauma) | 550 (4.7) | |
| Craniotomy for trauma | 627 (5.4) | |
| Cardiac valve surgery using cardiac catheterization | 588 (5.0) | |
| Cardiac valve surgery without cardiac catheterization | 1305 (11.2) | |
| Coronary artery bypass graft | 1799 (15.4) | |
| Major vascular repair surgery | 480 (4.1) | |
| Percutaneous angioplasty | 1272 (10.9) | |
| Esophageal surgery | 505 (4.3) | |
| Rectal surgery | 98 (0.8) | |
| Major small and large intestine surgery | 644 (5.5) | |
| Gastric and duodenal surgery | 273 (2.3) | |
| Pancreas and liver surgery | 199 (1.7) | |
| Charlson comorbidity index | 0 | 1833 (15.7) |
| 1–5 | 7836 (67.0) | |
| ≥6 | 2024 (17.3) | |
| Admission route | Outpatient visit | 9156 (78.3) |
| Emergency room | 2537 (21.7) | |
| History of respiratory disease | No | 7756 (66.3) |
| Yes | 3937 (33.7) | |
| Ventilator application time | <1 day | 8662 (74.1) |
| 1 day to 3 days | 2180 (18.6) | |
| 4 days and more | 851 (7.3) |
| Variable | Category | Incidence of Pneumonia | X2 (p) | In-Hospital Mortality | X2 (p) |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Hospital ownership | Public | 54 (1.5) | 77.28 | 227 (6.1) | 400.47 |
| Educational foundation | 220 (4.0) | (<0.001) | 937 (17.1) | (<0.001) | |
| Medical corporation | 33 (1.3) | 116 (4.7) | |||
| Location | Seoul | 66 (1.1) | 193.59 | 391 (6.3) | 345.09 |
| Metropolitan cities | 156 (6.4) | (<0.001) | 480 (19.6) | (<0.001) | |
| Other regions | 85 (2.8) | 409 (13.5) | |||
| Number of adult ICU beds | <50 | 79 (4.2) | 249.03 | 416 (22.3) | 810.38 |
| 50–69 | 157 (6.5) | (<0.001) | 499 (20.8) | (<0.001) | |
| 70–119 | 53 (1.3) | 286 (7.2) | |||
| ≥120 | 18 (0.5) | 79 (2.3) | |||
| Dedicated resident in ICU | No | 171 (2.6) | 0.04 | 738 (11.2) | 1.12 |
| Yes | 136 (2.7) | (0.838) | 542 (10.6) | (0.290) | |
| Dedicated specialist in ICU | No | 202 (2.7) | 0.95 | 842 (11.4) | 4.28 |
| Yes | 105 (2.4) | (0.330) | 438 (10.2) | (0.039) | |
| Nurse staffing level in ICU | Grade 1 | 41 (0.6) | 278.31 | 263 (3.8) | 952.81 |
| Grade 2 | 214 (5.3) | (<0.001) | 791 (19.5) | (<0.001) | |
| Grade 3 and higher | 52 (7.0) | 226 (30.3) |
| Variable | Category | Incidence of Pneumonia | X2 (p) | In-Hospital Mortality | X2 (p) |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age | 20–49 | 31 (1.5) | 34.9 | 175 (8.2) | 139.91 |
| 50–59 | 65 (2.3) | (<0.001) | 253 (8.9) | (<0.001) | |
| 60–69 | 71 (2.3) | 268 (8.7) | |||
| 70–85 | 140 (3.8) | 584 (16.0) | |||
| Sex | Male | 201 (2.9) | 4.25 | 769 (11.0) | 0.05 (0.817) |
| Female | 106 (2.2) | (0.039) | 511 (10.9) | ||
| Korean Diagnosis-Related Group | Major craniotomy (excluding trauma) | 69 (2.1) | 364.56 | 298 (8.9) | 1604.28 |
| Other type of craniotomy (excluding trauma) | 32 (5.8) | (<0.001) | 232 (42.2) | (<0.001) | |
| Craniotomy for trauma | 38 (6.1) | 210 (33.5) | |||
| Cardiac valve surgery using cardiac catheterization | 1 (0.2) | 2 (0.3) | |||
| Cardiac valve surgery without cardiac catheterization | 5 (0.4) | 5 (0.4) | |||
| Coronary artery bypass graft | 4 (0.2) | 5 (0.3) | |||
| Major vascular repair surgery | 1 (0.2) | 29 (6.0) | |||
| Percutaneous angioplasty | 114 (9.0) | 273 (21.5) | |||
| Esophageal surgery | 4 (0.8) | 5 (1.0) | |||
| Rectal surgery | 2 (2.0) | 12 (12.2) | |||
| Major small and large intestine surgery | 22 (3.4) | 133 (20.7) | |||
| Gastric and duodenal surgery | 14 (5.1) | 49 (18.0) | |||
| Pancreas and liver surgery | 1 (0.5) | 27 (13.6) | |||
| Charlson comorbidity index | 0 | 28 (1.5) | 16.27 | 190 (10.4) | 34.97 |
| 1–5 | 206 (2.6) | (<0.001) | 793 (10.1) | (<0.001) | |
| ≥6 | 73 (3.6) | 297 (14.7) | |||
| Admission route | Outpatient visit | 181 (2.0) | 69.45 | 744 (8.1) | 344.47 |
| Emergency room | 126 (5.0) | (<0.001) | 536 (21.1) | (<0.001) | |
| History of respiratory disease | No | 115 (1.5) | 117.67 | 794 (10.2) | 11.89 |
| Yes | 192 (4.9) | (<0.001) | 486 (12.3) | (0.001) | |
| Ventilator application time | <1 day | 168 (1.9) | 118.92 | 579 (6.7) | 1349.13 |
| 1 day to 3 days | 70 (3.2) | (<0.001) | 296 (13.6) | (<0.001) | |
| 4 days and more | 69 (8.1) | 405 (47.6) |
| Incidence of Pneumonia | In-Hospital Mortality | |||||
|---|---|---|---|---|---|---|
| Variable | Category | OR | (95% CI) | OR | (95% CI) | |
| Patient factors | Age | 1.01 | (1.00–1.03) | 1.02 | (1.01–1.03) | |
| Sex | Male | 1.30 | (1.04–1.62) | 1.03 | (0.88–1.21) | |
| Female | 1 | 1 | ||||
| Charlson comorbidity index | 0 | 0.58 | (0.33–1.01) | 0.84 | (0.62–1.14) | |
| 1–5 | 0.84 | (0.62–1.13) | 0.82 | (0.66–1.01) | ||
| ≥6 | 1 | 1 | ||||
| History of respiratory disease | Yes | 3.86 | (2.85–5.23) | 1.06 | (0.87–1.28) | |
| No | 1 | |||||
| Admission route | Outpatient visit | 0.53 | (0.40–0.71) | 1.32 | (1.07–1.63) | |
| Emergency room | 1 | 1 | ||||
| Ventilator application days | 1–3 | 1.07 | (1.04–1.11) | 1.73 | (1.29–2.31) | |
| ≥4 | 1.46 | (1.03–2.08) | 6.13 | (4.21–8.92) | ||
| <1 | 1 | 1 | ||||
| Hospital factors | Hospital ownership | Public | 0.61 | (0.39–0.95) | 0.60 | (0.30–1.20) |
| Educational foundation | 0.96 | (0.60–1.55) | 0.96 | (0.56–1.64) | ||
| Medical corporation | 1 | 1 | ||||
| Location | Seoul | 0.78 | (0.34–1.77) | 0.97 | (0.60–1.58) | |
| Metropolitan cities | 1.61 | (0.71–3.66) | 1.16 | (0.80–1.69) | ||
| Other regions | 1 | 1 | ||||
| Number of adult ICU beds | 1 | (0.99–1.01) | 0.99 | (0.99–1.00) | ||
| Dedicated resident in ICU | Yes | 0.93 | (0.50–1.72) | 0.82 | (0.58–1.17) | |
| No | 1 | 1 | ||||
| Dedicated specialist in ICU | Yes | 0.92 | (0.53–1.59) | 0.54 | (0.38–0.77) | |
| No | 1 | 1 | ||||
| Nurse staffing level in ICU | Grade 1 | 0.27 | (0.09–0.86) | 0.41 | (0.18–0.95) | |
| Grade 2 | 0.90 | (0.36–2.23) | 0.79 | (0.51–1.22) | ||
| Grade 3 and higher | 1 | 1 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, S.-H. The Relationship of Nurse and Physician Staffing in Intensive Care Units with Patient Outcomes in Postoperative Patients on Ventilators: An Analysis Using Korean National Health Insurance Data. Healthcare 2023, 11, 1124. https://doi.org/10.3390/healthcare11081124
Kim Y, Kim S-H. The Relationship of Nurse and Physician Staffing in Intensive Care Units with Patient Outcomes in Postoperative Patients on Ventilators: An Analysis Using Korean National Health Insurance Data. Healthcare. 2023; 11(8):1124. https://doi.org/10.3390/healthcare11081124
Chicago/Turabian StyleKim, Yunmi, and Seon-Ha Kim. 2023. "The Relationship of Nurse and Physician Staffing in Intensive Care Units with Patient Outcomes in Postoperative Patients on Ventilators: An Analysis Using Korean National Health Insurance Data" Healthcare 11, no. 8: 1124. https://doi.org/10.3390/healthcare11081124