
Effectiveness of the Patient’s Severity Classification Competency Promotion Virtual Reality Program of Nursing Students during the COVID-19 Pandemic Period

Abstract
:1. Introduction
2. Materials and Methods
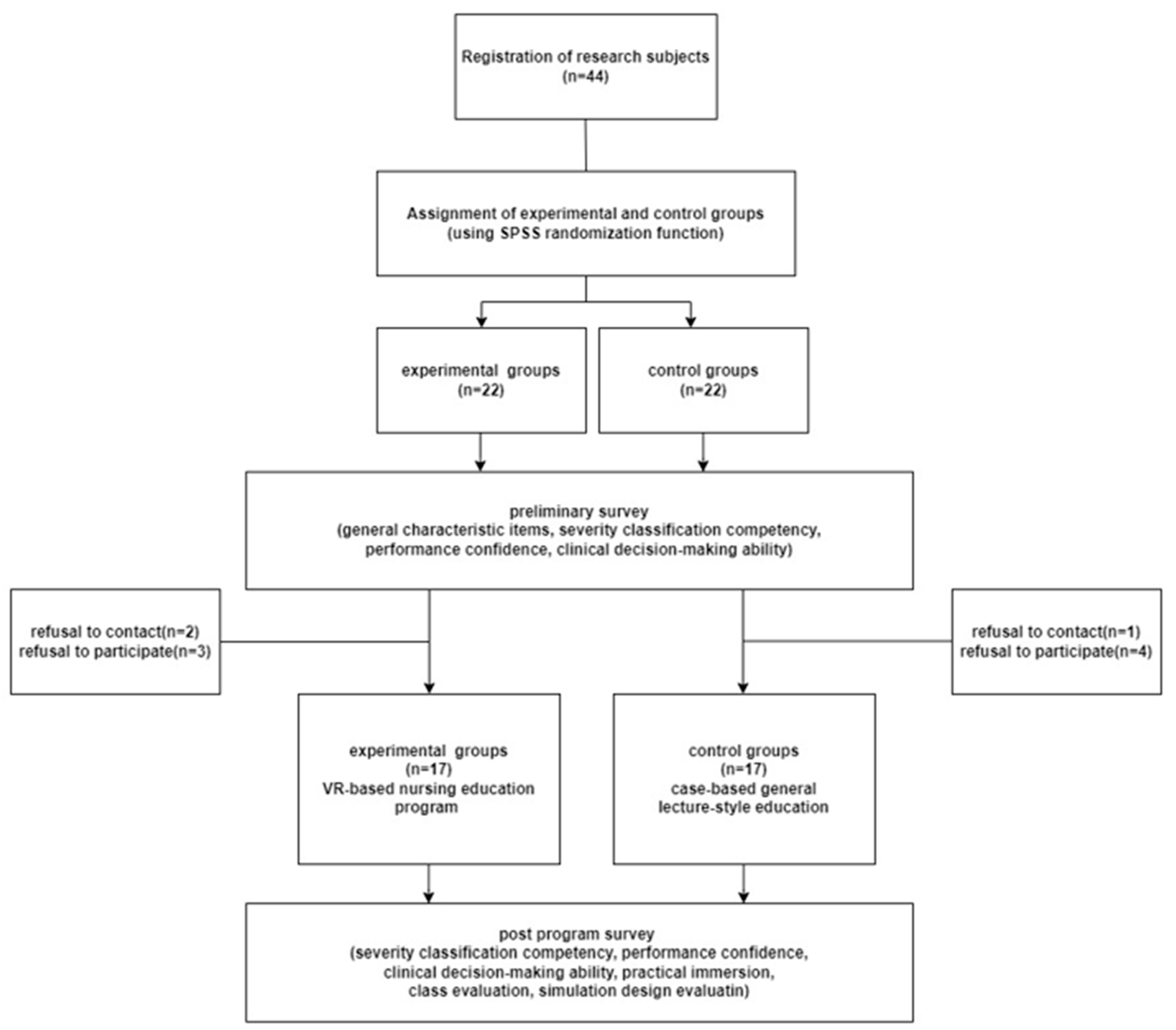
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Severity Classification Competency
2.3.2. Confidence in Performance
2.3.3. Clinical Decision-Making Ability
2.3.4. Class Evaluation
2.3.5. Simulation Design Evaluation
2.3.6. Practice Flow
2.4. Data Collection
2.5. Development of a Nursing Education Program to Improve the Severity Classification Competency of Nursing Students Using Virtual Reality
2.6. Application of Nursing Education Program to Improve Severity Classification Competency of Nursing Students Using Virtual Reality
2.6.1. Preliminary Survey
2.6.2. Application of Nursing Education Program to Improve Severity Classification Competency
2.6.3. Post Program Survey
2.7. Data Analysis
3. Results
3.1. General Characteristics and Homogeneity Test of Participants
3.2. Difference between the Experimental Group and the Control Group’s Severity Classification Competency, Performance Confidence, and Clinical Decision-Making Ability before and after the Program
3.3. Differences in Class Evaluation, Simulation Design Evaluation, and Practice Immersion between the Groups Post Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gómez-Angelats, E.; Miró, Ò. Triage level assignment and nurse characteristics and experience. Emergencias 2018, 30, 163–168. [Google Scholar]
- Gottlieb, M.; Farcy, D.A.; Moreno, L.A.; Vilke, G.M.; Guittard, J.A. Triage nurse-ordered testing in the emergency department setting: A review of the literature for the clinician. J. Emerg. Med. 2021, 60, 570–575. [Google Scholar] [CrossRef]
- Choi, Y.H. Hospital infection control practice in the COVID-19 era: An experience of university affiliated hospital. Kor. J. Med. 2020, 95, 308–314. [Google Scholar] [CrossRef]
- Liu, Y.; Lee, J.M.; Lee, C. The challenges and opportunities of a global health crisis: The management and business implications of COVID-19 from an Asian perspective. Asian Bus. Manag. 2020, 19, 277–297. [Google Scholar] [CrossRef]
- Lucchini, A.; Giani, M.; Elli, S.; Villa, S.; Rona, R.; Foti, G. Nursing activities score is increased in COVID-19 patients. Intensive Crit. Care Nurs. 2020, 59, 102876. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, A.; Iozzo, P.; Bambi, S. Nursing workload in the COVID-19 era. Intensive Crit. Care Nurs. 2020, 61, 102929. [Google Scholar] [CrossRef]
- Kim, H.J.; Kang, H.Y. Effects of a web-based Korean Triage and Acuity Scale learning program on triage self-efficacy and triage performance ability for nurses in emergency department. J. Kor. Acad. Nurs. 2019, 49, 171–180. [Google Scholar] [CrossRef]
- Wolf, L.A.; Delao, A.M.; Perhats, C.; Moon, M.D.; Zavotsky, K.E. Triaging the emergency department, not the patient: United States emergency nurses’ experience of the triage process. J. Emerg. Nurs. 2018, 44, 258–266. [Google Scholar] [CrossRef]
- Lee, H.J.; Cho, K.J. Comparison of knowledge level of triage in 119 EMTs. Kor. J. Emerg. Med. Ser. 2014, 18, 43–54. [Google Scholar] [CrossRef] [Green Version]
- Chun, K.H.; Lee, H.J. The evaluation of responses and abilities of 119 EMTs to perform pediatric triage. Fire Sci. Eng. 2021, 35, 66–73. [Google Scholar] [CrossRef]
- Park, J.Y.; Choi, S.M. A study on the triage performance of military nurses and its related factors using a mass casualty scenario, paper exercise. Kor. J. Mil. Nurs. Res. 2012, 30, 128–142. [Google Scholar]
- Hur, J.; Park, H.J. Nursing students’ perception, competency of disaster nursing and ego resilience. J. Learn. Cent. Curr. Instr. 2015, 15, 121–138. [Google Scholar]
- Kim, H.J. A study on disaster preparedness, core competencies and educational needs on disaster nursing of nursing students. J. Korea Acad. Industr. Coop. Soc. 2015, 16, 7447–7455. [Google Scholar] [CrossRef] [Green Version]
- Park, A.S. The effect of disaster awareness, attitude, preparedness on the basic competencies of disaster nursing among nursing students. J. Kor. Data Anal. Soc. 2017, 19, 1625–1636. [Google Scholar] [CrossRef]
- Choi, M.J.; Kim, K.J. Effects of simulation program using immersive virtual reality: Meta-analysis. J. Korea Converg. Soc. 2021, 12, 381–388. [Google Scholar] [CrossRef]
- Butt, A.L.; Kardong-Edgren, S.; Ellertson, A. Using game-based virtual reality with haptics for skill acquisition. Clin. Simul. Nurs. 2018, 16, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Kahn, C.A.; Schultz, C.H.; Miller, K.T.; Anderson, C.L. Does START triage work? An outcomes assessment after a disaster. Ann. Emerg. Med. 2009, 54, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Kim, S.H.; Lee, W.S. Effects of a virtual reality simulation and a blended simulation of care for pediatric patient with asthma. Child Health Nurs. Res. 2019, 25, 496. [Google Scholar] [CrossRef]
- Frick, K.D.; Swoboda, S.M.; Mansukhani, K.; Jeffries, P.R. An economic model for clinical simulation in prelicensure nursing programs. J. Nurs. Regul. 2014, 5, 9–13. [Google Scholar] [CrossRef]
- Killion, C.; Reilly, J.; Gallagher-Lepak, S. Becoming an onliner: Students perceptions of moving from traditional to virtual learning. J. Nurs. Inform. 2011, 15, 139. [Google Scholar]
- Cant, R.P.; Cooper, S.J. Simulation in the Internet age: The place of web-based simulation in nursing education. An integrative review. Nurse Educ. Today 2014, 34, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- You, H.E.; Yang, B.S. The effects of virtual reality simulation scenario application on clinical competency, problem solving ability and nursing performance confidence. J. Korea Acad. Industr. Coop. Soc. 2021, 22, 116–126. [Google Scholar] [CrossRef]
- Lim, J.H. The effect of virtual reality simulation education on nursing process competency. J. Digit. Converg. 2021, 19, 401–409. [Google Scholar] [CrossRef]
- Aebersold, M. Simulation-based learning: No longer a novelty in undergraduate education. J. Issues Nurs. 2018, 23, 1. [Google Scholar] [CrossRef]
- Lim, S.H. Content analysis on online non-face-to-face adult nursing practice experienced by graduating nursing students in the ontact era. J. Korea Acad. Industr. Coop. Soc. 2021, 22, 195–205. [Google Scholar] [CrossRef]
- Smith, S.J.; Farra, S.L.; Ulrich, D.L.; Hodgson, E.; Nicely, S.; Mickle, A. Effectiveness of two varying levels of virtual reality simulation. Nurs. Educ. Perspect. 2018, 39, E10–E15. [Google Scholar] [CrossRef]
- Padilha, J.M.; Machado, P.P.; Ribeiro, A.; Ramos, J.; Costa, P. Clinical virtual simulation in nursing education: Randomized controlled trial. J. Med. Int. Res. 2019, 21, e11529. [Google Scholar] [CrossRef]
- Lee, E.J.; Ryu, M.J. Development and effects of a nursing education program using virtual reality for enhancing clinical decision-making ability in respiratory disease nursing care. J. Kor. Acad. Fundam. Nurs. 2021, 28, 458–469. [Google Scholar] [CrossRef]
- Lim, S.M.; Yeom, Y.R. The effect of education integrating virtual reality simulation training and outside school clinical practice for nursing students. J. Converg. Inf. Technol. 2020, 10, 100–108. [Google Scholar] [CrossRef]
- Cobbett, S.; Snelgrove-Clarke, E. Virtual versus face-to-face clinical simulation in relation to student knowledge, anxiety, and self-confidence in maternal-newborn nursing: A randomized controlled trial. Nurse Educ. Today 2016, 45, 179–184. [Google Scholar] [CrossRef]
- Verkuyl, M.; Hughes, M. Virtual gaming simulation in nursing education: A mixed-methods study. Clin. Simul. Nurs. 2019, 29, 9–14. [Google Scholar] [CrossRef]
- Kim, S.K.; Eom, M.R.; Park, M.H. Effects of nursing education using virtual reality: A systematic review. J. Korea Contents Assoc. 2019, 19, 661–670. [Google Scholar] [CrossRef]
- Gates, M.G.; Parr, M.B.; Hughen, J.E. Enhancing nursing knowledge using high-fidelity simulation. J. Nurs. Educ. 2012, 51, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.; Cole, P.G. An aptitude-treatment interaction in a mastery learning model of instruction. J. Exp. Educ. 1987, 55, 189–200. [Google Scholar] [CrossRef]
- Koles, P.G.; Stolfi, A.; Borges, N.J.; Nelson, S.; Parmelee, D.X. The impact of team-based learning on medical students’ academic performance. Acad. Med. 2010, 85, 1739–1745. [Google Scholar] [CrossRef]
- Moon, S.H. Development of the Triage Competency Scale for Emergency Nurses. Ph.D. Thesis, Seoul National University, Seoul, Republic of Korea, 2017. [Google Scholar]
- Kim, H.K. Application Effect of Simulation Education for Clinical Decision Making Enhancement of Nursing Students. Ph.D. Thesis, Chonnam National University, Gwangju, Republic of Korea, 2015. [Google Scholar]
- Jenkins, H.M. Improving clinical decision making in nursing. J. Nurs. Educ. 1985, 24, 242–243. [Google Scholar] [CrossRef]
- Baek, M.K. Relationship between Level of Autonomy and Clinical Decision-Making in Nursing Scale of E.T Nurse. Master’s Thesis, Yonsei University, Seoul, Republic of Korea, 2005. [Google Scholar]
- Ko, E.M.; Lee, H.K.; Han, E.O. A study for development of the course evaluation tool for college lecture types. J. Humanit. 2013, 31, 365–394. [Google Scholar]
- Yoo, J.H. Factors Influencing Nursing Student’s Flow Experience and Clinical Competency in Simulation-Base Education-Based on Jeffries’s Simulation Model. Master’s Thesis, Sungshin University, Seoul, Republic of Korea, 2016. [Google Scholar]
- Engeser, S.; Rheinberg, F. Flow, performance and moderators of challenge-skill balance. Motiv. Emot. 2008, 32, 158–172. [Google Scholar] [CrossRef]
- Jeffries, P.R. A framework for designing, implementing and evaluating simulation used as teaching strategies in nursing. Nurs. Educ. Perspect. 2005, 26, 96–103. [Google Scholar]
- Plotzky, C.; Lindwedel, U.; Sorber, M.; Loessl, B.; König, P.; Kunze, C.; Meng, M. Virtual reality simulations in nurse education: A systematic mapping review. Nurse Educ. Today 2021, 101, 104868. [Google Scholar] [CrossRef]
- Leem, E.S. The Present and application methods of virtual/augmented reality technology in nursing and medical education. J. Kor. Acad. Soc. Nurs. Educ. 2019, 2019, 19–39. [Google Scholar]
- Choi, S.H.; Won, J.S. The nature of flow in virtual reality education: Based on a grounded theory approach. J. Korea Contents Assoc. 2017, 17, 446–460. [Google Scholar] [CrossRef]
- Duran, L.B.; Duran, E. The 5E instructional model: A learning cycle approach for inquiry-based science teaching. Sci. Educ. Rev. 2004, 3, 49–58. [Google Scholar]
- Tseng, T.J.; Guo, S.E.; Hsieh, H.W.; Lo, K.W. The effect of a multidimensional teaching strategy on the self-efficacy and critical thinking dispositions of nursing students: A quasi-experimental study. Nurse Educ. Today 2022, 119, 105531. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.O.; Kwon, S.J.; Kim, J.; Song, J.H. Effects of nursing skills practice using VR (virtual reality) on competency and confidence in nursing skills, learning self-efficacy, and satisfaction of nursing students. J. Ind. Converg. 2022, 20, 47–55. [Google Scholar] [CrossRef]
- Bryant, R.; Miller, C.L.; Henderson, D. Virtual clinical simulations in an online advanced health appraisal course. Clin. Simul. Nurs. 2015, 11, 437–444. [Google Scholar] [CrossRef]
- Cakir, N.K. Effect of 5E learning model on academic achievement, attitude and science process skills: Meta-analysis study. J. Educ. Train. 2017, 5, 157–170. [Google Scholar] [CrossRef] [Green Version]
- Rosdianto, H.; Teeka, C. The Improvement of students’ problem-solving skills through 5E learning model. J. Pendidik. Indones. 2019, 8, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.Y.; Choi, J.Y. A comparative study on learning outcomes according to the Integration sequences of S-PBL in nursing students: Randomized crossover design. J. Kor. Acad. Nurs. 2019, 49, 92–103. [Google Scholar] [CrossRef]
- Chen, F.Q.; Leng, Y.F.; Ge, J.F.; Wang, D.W.; Li, C.; Chen, B.; Sun, Z.L. Effectiveness of virtual reality in nursing education: Meta-analysis. J. Med. Int. Res. 2020, 22, e18290. [Google Scholar] [CrossRef]
- Forsberg, E.; Ziegert, K.; Hult, H.; Fors, U. Assessing progression of clinical reasoning through virtual patients: An exploratory study. Nurse Educ Pract. 2016, 16, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Rourke, S. How does virtual reality simulation compare to simulated practice in the acquisition of clinical psychomotor skills for pre-registration student nurses? A systematic review. Int. J. Nurs. Stud. 2020, 102, 103466. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.Y.; Gu, M.K.; Sok, S.H. A concept analysis of nurses’ clinical decision making: Implications for Korea. J. Environ. Res. Public Health 2022, 19, 3596. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Categories | Exp.(n = 17) | Cont.(n = 17) | x2 or F | p |
|---|---|---|---|---|---|
| n (%) or M ± SD | n (%) or M ± SD | ||||
| Age (year) | 21.65 ± 0.61 | 21.59 ± 0.87 | 3.04 | 0.091 | |
| Preferred education | Lecture | 11(64.7) | 11(64.7) | 0.58 | 0.452 |
| Discussion | 1(5.9) | 1(5.9) | |||
| Q and A | 2(11.8) | 0(0) | |||
| Performance | 3(17.6) | 5(29.4) | |||
| Last semester grade | <2.5 | 1(5.9) | 1(5.9) | 2.04 | 0.163 |
| 2.5–3.0 | 2(11.8) | 1(5.9) | |||
| 3.0–3.5 | 10(58.8) | 5(29.4) | |||
| 3.5–4.0 | 3(17.6) | 6(35.3) | |||
| 4.0–4.5 | 1(5.9) | 4(23.5) |
| Variables | Exp.(n = 17) | Cont.(n = 17) | t | p |
|---|---|---|---|---|
| M ± SD | M ± SD | |||
| Severity classification competency | 2.71 ± 0.53 | 2.95 ± 0.39 | 1.45 | 0.157 |
| Confidence in performance | 3.43 ± 0.46 | 3.81 ± 0.39 | −0.80 | 0.427 |
| Clinical decision-making ability | 3.28 ± 0.18 | 3.66 ± 0.66 | 4.59 | <0.001 |
| Search for alternatives or options | 3.27 ± 0.28 | 3.77 ± 0.51 | 3.59 | <0.001 |
| Evaluation and reevaluation of consequences | 3.44 ± 0.31 | 4.05 ± 0.38 | 5.09 | <0.001 |
| Canvassing of objectives and values | 3.28 ± 0.41 | 3.25 ± 0.41 | −0.30 | 0.760 |
| Search for information and unbiased assimilation of new information | 3.15 ± 0.29 | 3.55 ± 0.43 | 3.17 | <0.001 |
| Characteristics | Exp.(n = 17) | Cont.(n = 17) | Source | x2 or F | p |
|---|---|---|---|---|---|
| M ± SD | M ± SD | ||||
| Confidence in performance | |||||
| Pretest | 3.43 ± 0.46 | 3.81 ± 0.39 | Group | 1.07 | 0.309 |
| Posttest | 4.18 ± 0.29 | 4.06 ± 0.56 | Time | 34.92 | <0.001 |
| Group/time | 8.631 | 0.006 | |||
| Severity classification competency | |||||
| Pretest | 2.71 ± 0.53 | 2.95 ± 0.36 | Group | 0.01 | 0.957 |
| Posttest | 4.12 ± 0.26 | 3.88 ± 0.48 | Time | 134.99 | <0.001 |
| Group/time | 5.73 | 0.023 | |||
| Clinical decision-making ability_Canvassing of objectives and values | |||||
| Pretest | 3.28 ± 0.25 | 3.25 ± 0.40 | Group | 3.31 | <0.001 |
| Posttest | 3.95 ± 0.40 | 3.57 ± 0.45 | Time | 56.27 | <0.001 |
| Group/time | 7.17 | <0.001 | |||
| Variables | Exp.(n = 17) | Cont.(n = 17) | t | p |
|---|---|---|---|---|
| M ± SD | M ± SD | |||
| Class evaluation | ||||
| Learning management | 4.79 ± 0.36 | 4.82 ± 0.39 | −0.29 | 0.821 |
| Instructional methods, materials | 4.85 ± 0.24 | 4.84 ± 0.37 | 0.11 | 0.913 |
| Objectivity of assessment | 4.57 ± 0.65 | 4.78 ± 0.44 | −1.12 | 0.269 |
| Learning satisfaction | 4.91 ± 0.26 | 4.82 ± 0.39 | 0.76 | 0.449 |
| Total | 4.78 ± 0.29 | 4.82 ± 0.39 | −0.33 | 0.741 |
| Simulation design evaluation | ||||
| Learning goals and education | 4.56 ± 0.47 | 4.55 ± 0.68 | 0.049 | 0.961 |
| Support | 4.87 ± 0.22 | 4.71 ± 0.56 | 1.10 | 0.280 |
| Problem solving | 4.72 ± 0.28 | 4.73 ± 0.52 | −0.81 | 0.936 |
| Feedback | 4.56 ± 0.55 | 4.79 ± 0.52 | −1.27 | 0.210 |
| Realism | 4.74 ± 0.53 | 4.71 ± 0.59 | 0.153 | 0.880 |
| Total | 4.67 ± 0.32 | 4.69 ± 0.55 | −0.07 | 0.942 |
| Practice flow | 4.31 ± 0.48 | 4.46 ± 0.66 | −0.77 | 0.456 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Baek, G.; Hwang, Y. Effectiveness of the Patient’s Severity Classification Competency Promotion Virtual Reality Program of Nursing Students during the COVID-19 Pandemic Period. Healthcare 2023, 11, 1122. https://doi.org/10.3390/healthcare11081122
Lee E, Baek G, Hwang Y. Effectiveness of the Patient’s Severity Classification Competency Promotion Virtual Reality Program of Nursing Students during the COVID-19 Pandemic Period. Healthcare. 2023; 11(8):1122. https://doi.org/10.3390/healthcare11081122
Chicago/Turabian StyleLee, Eunju, Gyuli Baek, and Yeonhui Hwang. 2023. "Effectiveness of the Patient’s Severity Classification Competency Promotion Virtual Reality Program of Nursing Students during the COVID-19 Pandemic Period" Healthcare 11, no. 8: 1122. https://doi.org/10.3390/healthcare11081122