

Addressing HIV Misconceptions among Heterosexual Black Men and Communities in Ontario
 ,
,
Abstract
:1. Introduction
2. Methods
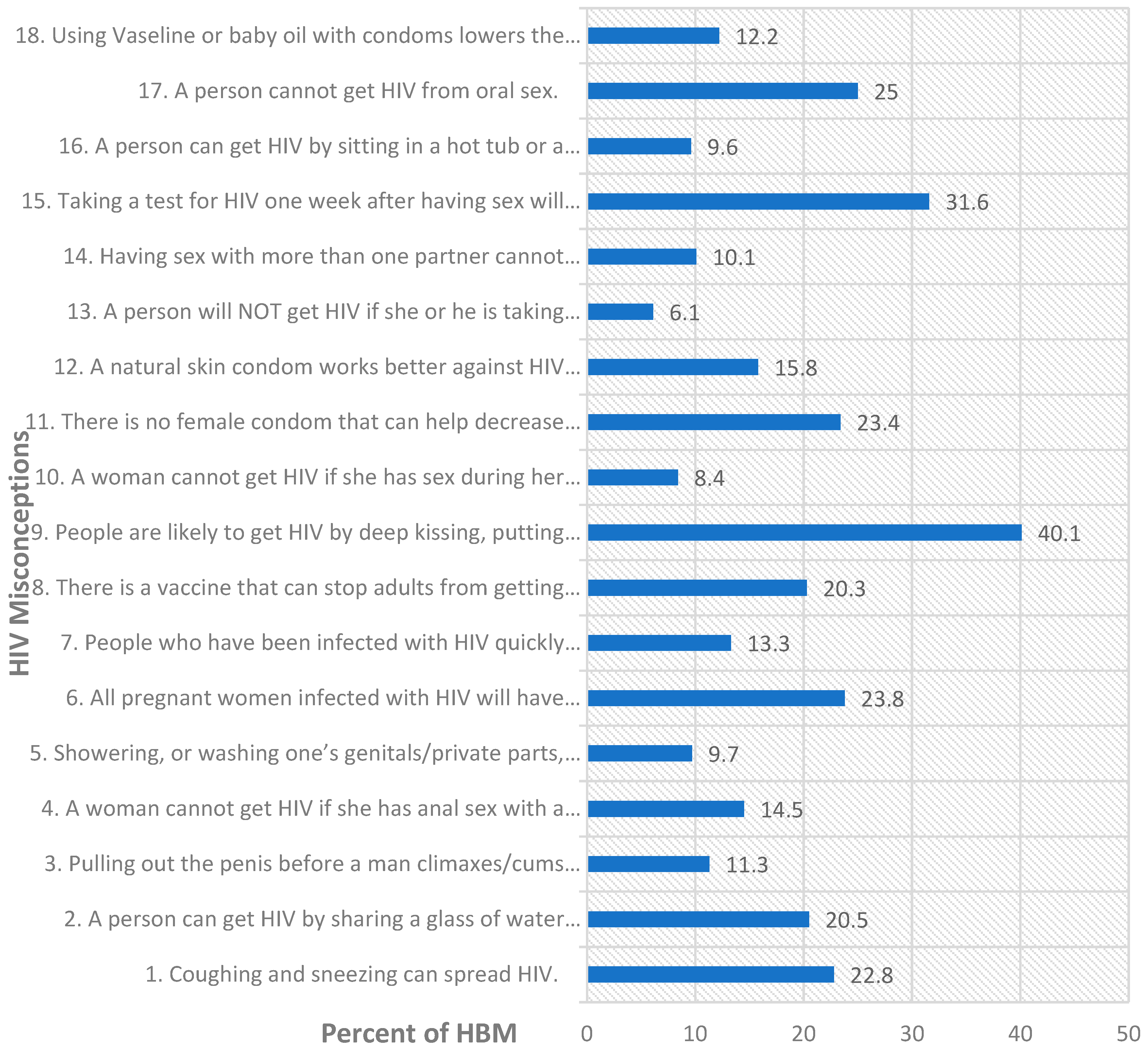
3. Results
4. Discussion
4.1. Risk Factors of HIV Misconceptions
4.2. Protective Factors of HIV Misconceptions
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| S/N | Misconceptions | Correct Knowledge | Explanatory Notes |
|---|---|---|---|
| 1 | Coughing and sneezing can spread HIV. | Coughing and sneezing DO NOT spread HIV. | Because HIV is not airborne, it is not carried by tiny particles from sneezes and coughs [51]. |
| 2 | A person can get HIV by sharing a glass of water with someone who has HIV. | A person CANNOT get HIV by sharing a glass of water with someone who has HIV. | HIV cannot be spread by sharing drinking glasses because science shows that the risk of getting it from saliva is extremely low. |
| 3 | Pulling out the penis before a man climaxes/cums keeps a woman from getting HIV during sex. | Pulling out the penis before a man climaxes/cums MAY NOT keep a woman from getting HIV during sex. | Although semen is one of the most common ways through which HIV is transmitted during sex, pre-ejaculatory fluid may also transmit HIV [52,53]. |
| 4 | A woman cannot get HIV if she has anal sex with a man. | A woman can get HIV if she has anal sex with a man. | Anal sex is the riskiest type of sex for getting or transmitting HIV and being the receptive partner (bottom) makes it riskier than being the insertive partner (top) [54]. |
| 5 | Showering, or washing one’s genitals/private parts, after sex keeps a person from getting HIV. | Showering, or washing one’s genitals/private parts, after sex CANNOT keep a person from getting HIV. | Surprisingly, a study showed that washing the penis immediately after increases the risk of acquiring HIV by uncircumcised men [55]. |
| 6 | All pregnant women infected with HIV will have babies born with AIDS. | NOT ALL pregnant women infected with HIV will have babies born with AIDS. | If the woman is on antiretroviral therapy during pregnancy, she can prevent transmission of HIV to the unborn baby. |
| 7 | People who have been infected with HIV quickly show serious signs of being infected. | People who have been infected with HIV DO NOT quickly show serious signs of being infected. | Most (80%) people infected with HIV experience a short, flu-like illness that occurs 2–6 weeks after infection. After this, HIV may not cause any symptoms for several (10) years [56]. |
| 8 | There is a vaccine that can stop adults from getting HIV. | There is NO VACCINE that can stop adults from getting HIV. | Scientists are still working to develop an HIV vaccine, and Durbin, a professor in international health, says there will not be one by 2030 [57]. |
| 9 | People are likely to get HIV by deep kissing, putting their tongue in their partner’s mouth, if their partner has HIV. | People are NOT LIKELY to get HIV by deep kissing, putting their tongue in their partner’s mouth if their partner has HIV. | You cannot transmit HIV through closed-mouth or “social” kissing with someone who has HIV, except very rarely, when both partners have mouth sores and bleeding gums [54]. |
| 10 | A woman cannot get HIV if she has sex during her period. | A woman CAN get HIV if she has sex during her period. | Studies show that heterosexual transmission of HIV and other STIs happens more easily during menstruation [58]. |
| 11 | There is no female condom that can help decrease a woman’s chance of getting HIV. | There is a female condom that can help decrease a woman’s chance of getting HIV. | There are female condoms, and they are as effective at protecting against HIV as male condoms. Like the male condoms they are available in some drug stores, community health centers, and AIDS service organisations. |
| 12 | A natural skin condom works better against HIV than does a latex condom. | A natural skin condom DOES NOT work better against HIV than does a latex condom. | Latex condoms provide the best protection against HIV. Natural membrane (such as lambskin) condoms have small holes in them and do not block HIV and other STDs [59]. |
| 13 | A person will NOT get HIV if she or he is taking antibiotics. | A person MAY GET HIV Even if she or he is taking antibiotics. | Taking antibiotics does not prevent HIV but they can prevent STIs [60]. More research is needed to estimate the efficacy of antibiotics in preventing HIV transmission [61]. However, PrEP or PEP taken as prescribed by a physician prevents HIV. |
| 14 | Having sex with more than one partner cannot increase a person’s chance of being infected with HIV. | Having sex with more than one partner can increase a person’s chance of being infected with HIV. | Having multiple sex partners who overlap in time increases one’s and one’s regular partner’s risk of getting HIV and STIs [62]. |
| 15 | Taking a test for HIV one week after having sex will tell a person if she or he has HIV. | Taking a test for HIV one week after having sex WILL NOT tell a person if she or he has HIV. | A rapid antigen test carried out with blood from a finger detects HIV 18 to 90 days after exposure. An antigen lab test using blood from a vein detects HIV 18 to 45 days after exposure. A nucleic acid test detects HIV 10 to 33 days after exposure [63]. |
| 16 | A person can get HIV by sitting in a hot tub or a swimming pool with a person who has HIV. | A person CANNOT get HIV by sitting in a hot tub or a swimming pool with a person who has HIV. | HIV does not survive in water or hot tubs, but it survives in some human fluids: blood, semen, pre-seminal fluid, rectum fluids, vaginal fluids, and breast milk [64]. |
| 17 | A person cannot get HIV from oral sex. | A person can get HIV from oral sex. | Putting a mouth on the penis, vagina/vulva, or anus would normally not transmit HIV but ejaculating in a mouth with oral ulcers, bleeding gums, or genital sores and when having STIs increases the risk of getting HIV [62]. |
| 18 | Using Vaseline or baby oil with condoms lowers the chance of getting HIV. | Using Vaseline or baby oil with condoms CANNOT lower the chance of getting HIV. | Using baby oil on a latex condom may cause the condom to break and increase the risk of getting HIV. However, one can use recommended water- or silicone-based lubricants [62]. |
References
- Public Health Agency of Canada. Estimates of HIV Incidence, Prevalence and Canada’s Progress on Meeting the 90-90-90 HIV Targets, 2020. 2022. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/estimates-hiv-incidence-prevalence-canada-meeting-90-90-90-targets-2020.html (accessed on 13 October 2022).
- Mbuagbaw, L.; Tharao, W.; Husbands, W.; Nelson, E.L.; Aden, M.; Arnold, K.; Baidoobonso, S.; Dabone, C.; Dryden, O.; Etowa, E.; et al. A/C study protocol: A cross-sectional study of HIV epidemiology among African, Caribbean and Black people in Ontario. BMJ Open 2020, 10, e036259. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.E.; Tharao, W.; Husbands, W.; Sa, T.; Zhang, N.; Kushwaha, S.; Absalom, D.; Kaul, R. The epidemiology of HIV and other sexually transmitted infections in African, Caribbean and Black men in Toronto, Canada. BMC Infect. Dis. 2019, 19, 294. [Google Scholar] [CrossRef] [PubMed]
- Colyer, S. A Snapshot of HIV Diagnoses and the HIV Care Cascade among African, Caribbean and Black People in Ontario. OHESI. 2022. Available online: https://www.ohesi.ca/a-snapshot-of-hiv-diagnoses-and-the-hiv-care-cascade-among-african-caribbean-and-black-people-in-ontario/ (accessed on 13 October 2022).
- Haddad, N.; Weeks, A.; Robert, A.; Totten, S. HIV in Canada—Surveillance Report. 2019. Available online: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2021-47/issue-1-january-2021/hiv-surveillance-report-2019.html (accessed on 1 January 2023).
- Antabe, R.; Sano, Y.; Anfaara, F.W.; Luginaah, I. Reducing HIV misconceptions among females and males in Malawi: Are we making progress? AIDS Care 2021, 33, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Lilienfeld, S.O. Confronting Psychological Misconceptions in the Classroom. APS Obs. 2010, 23. Available online: https://www.psychologicalscience.org/observer/confronting-psychological-misconceptions-in-the-classroom (accessed on 10 January 2023).
- Murphy, P.K.; Alexander, P.A. Situating Text, Talk, and Transfer in Conceptual Change; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Cognitive Challenges of Effective Teaching. Available online: https://www.apa.org/ed/precollege/psychology-teacher-network/introductory-psychology/challenges-to-teaching (accessed on 1 January 2023).
- Antabe, R.; Konkor, I.; McIntosh, M.; Lawson, E.; Husbands, W.; Wong, J.; Arku, G.; Luginaah, I. “I went in there, had a bit of an issue with those folks”: Everyday challenges of heterosexual African, Caribbean and black (ACB) men in accessing HIV/AIDS services in London, Ontario. BMC Public Health 2021, 21, 315. [Google Scholar] [CrossRef]
- Laprise, C.; Bolster-Foucault, C. Understanding barriers and facilitators to HIV testing in Canada from 2009–2019: A systematic mixed studies review. Can. Commun. Dis. Rep. 2021, 47, 105–125. [Google Scholar] [CrossRef]
- Konkor, I.; Luginaah, I.; Husbands, W.; Omorodion, F.; Antabe, R.; Wong, J.; Kuuire, V.; Mkandawire, P.; Etowa, J. Immigrant generational status and the uptake of HIV screening services among heterosexual men of African descent in Canada: Evidence from the weSpeak study. J. Migr. Health 2022, 6, 100119. [Google Scholar] [CrossRef]
- Knight, R.; Small, W.; Shoveller, J.A. HIV Stigma and the Experiences of Young Men with Voluntary and Routine HIV Testing. Sociol. Health Illn. 2016, 38, 153–167. [Google Scholar] [CrossRef] [Green Version]
- Bogart, L.M.; Wagner, G.; Galvan, F.H.; Banks, D. Conspiracy Beliefs about HIV Are Related to Antiretroviral Treatment Nonadherence among African American Men with HIV. J. Acquir. Immune Defic. Syndr. 2010, 53, 648–655. [Google Scholar] [CrossRef] [Green Version]
- Quinn, K.G.; Reed, S.J.; Dickson-Gomez, J.; Kelly, J.A. An Exploration of Syndemic Factors That Influence Engagement in HIV Care Among Black Men. Qual. Health Res. 2018, 28, 1077–1087. [Google Scholar] [CrossRef]
- Bogart, L.M.; Skinner, D.; Weinhardt, L.S.; Glasman, L.; Sitzler, C.; Toefy, Y.; Kalichman, S.C. HIV/AIDS misconceptions may be associated with condom use among black South Africans: An exploratory analysis. Afr. J. AIDS Res. 2011, 10, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, M.; Eaton, L.A.; Watson, R.J.; Maksut, J.L.; Rucinski, K.B.; Earnshaw, V.A. Perpetuated HIV Microaggressions: A Novel Scale to Measure Subtle Discrimination against People Living with HIV. AIDS Educ. Prev. 2021, 33, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Djiadeu, P.; Smith, M.D.R.; Kushwaha, S.; Odhiambo, A.J.; Absalom, D.; Husbands, W.; Tharao, W.; Regan, R.; Sa, T.; Zhang, N.; et al. Social, Clinical, and Behavioral Determinants of HIV Infection and HIV Testing among Black Men in Toronto, Ontario: A Classification and Regression Tree Analysis. J. Int. Assoc. Provid. AIDS Care 2020, 19, 2325958220934613. [Google Scholar] [CrossRef] [PubMed]
- Omorodion, F.I.; Etowa, E.B.; Kerr, J.; Ghose, B.; Etowa, J. Correlates of Casual Sex Amidst Vulnerability to HIV among ACB Heterosexual Men in Ottawa and Windsor, Ontario Canada. J. Racial Ethn. Health Disparit. 2022, 9, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Husbands, W.; Etowa, J.; Oakes, W.; Omorodion, F.; Luginaah, I.; Etowa, E.; Ghose, B.; Pui-Hing Wong, J. Advancing research for HIV prevention among African, Caribbean and Black men: Protocol for a multisite cross-sectional study in Ontario (weSpeak study). Medicine 2021, 100, e25662. [Google Scholar] [CrossRef]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int. J. Methods Psychiatr. Res. 2003, 12, 65–76. [Google Scholar] [CrossRef]
- Baruth, K.E.; Caroll, J.J. A formal assessment of resilience: The Baruth Protective Factors Inventory. J. Individ. Psychol. 2002, 58, 235–244. [Google Scholar]
- Williams, D.R.; Yu, Y.; Jackson, J.S.; Anderson, N.B. Racial Differences in Physical and Mental Health: Socio-economic Status, Stress and Discrimination. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [Green Version]
- Omorodion, F.I.; Etowa, E.B.; Ker, J.; Ghose, B.; Etowa, J. HIV Exposure through Heterosexual Contacts: Analysis of Demographic, Behavioral and Structural Risk Factors among Black Men in Ottawa and Windsor, Ontario. Eur. J. Med. Health Sci. 2021, 3, 171–179. [Google Scholar] [CrossRef]
- Piper, K.; Enah, C.; Daniel, M. Black southern rural adolescents’ HIV stigma, denial, and misconceptions and implications for HIV prevention. J. Psychosoc. Nurs. Ment. Health Serv. 2014, 52, 50–56. [Google Scholar] [CrossRef]
- Coll, C.G.; Patton, F.; Marks, A.K.; Dimitrova, R.; Yang, R.; Suarez, G.A.; Patrico, A. Understanding the immigrant paradox in youth: Developmental and contextual considerations. In Realizing the Potential of Immigrant Youth; Cambridge University Press: New York, NY, USA, 2012; pp. 159–180. [Google Scholar]
- Earnshaw, V.A.; Bogart, L.M.; Dovidio, J.F.; Williams, D.R. Stigma and racial/ethnic HIV disparities: Moving toward resilience. Am. Psychol. 2013, 68, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Bogart, L.M.; Thorburn, S. Are HIV/AIDS conspiracy beliefs a barrier to HIV prevention among African Americans? J. Acquir. Immune Defic. Syndr. 2005, 38, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Niehaus, I.; Jonsson, G.D. Wouter Basson, Americans, and wild beasts: Men’s conspiracy theories of HIV/AIDS in the South African Lowveld. Med. Anthropol. 2005, 24, 179–208. [Google Scholar] [CrossRef] [PubMed]
- Mufune, P. Myths about condoms and HIV/AIDS in rural northern Namibia. Int. Soc. Sci. J. 2005, 57, 675–686. [Google Scholar] [CrossRef]
- Stewart, K.A. Review of “Witches, Westerners, and HIV: AIDS and Cultures of Blame in Africa” by Alexander Rodlach. AIDS Res. Ther. 2007, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Amoyaw, J.A.; Kuuire, V.Z.; Boateng, G.O.; Asare-Bediako, Y.; Ung, M. Conundrum of Sexual Decision Making in Marital Relationships: Safer-Sex Knowledge, Behavior, and Attitudes of Married Women in Zambia. J. Sex Res. 2015, 52, 868–877. [Google Scholar] [CrossRef]
- Tilahun, M.; Ayele, G. Factors associated with age at first sexual initiation among youths in Gamo Gofa, South West Ethiopia: A cross sectional study. BMC Public Health 2013, 13, 622. [Google Scholar]
- Stevens, G.W.; Walsh, S.D.; Huijts, T.; Maes, M.; Madsen, K.R.; Cavallo, F.; Molcho, M. An Internationally Comparative Study of Immigration and Adolescent Emotional and Behavioral Problems: Effects of Generation and Gender. J. Adolesc. Health 2015, 57, 587–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Geel, M.; Vedder, P. The Role of Family Obligations and School Adjustment in Explaining the Immigrant Paradox. J. Youth Adolesc. 2011, 40, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Sano, Y.; Abada, T. Immigration as a Social Determinant of Oral Health: Does the “Healthy Immigrant Effect” Extend to Self-rated Oral Health in Ontario, Canada? Can. Ethn. Stud. J. 2019, 51, 135–157. [Google Scholar] [CrossRef]
- Turcotte, M. Results from the 2016 Census: Education and Labour Market Integration of Black Youth in Canada. Insights on Canadian Society and Census 2016 Canada. Statistics Canada. 2020, 5-006-X. Available online: https://www150.statcan.gc.ca/n1/en/pub/75-006-x/2020001/article/00002-eng.pdf?st=TaFhcbU2 (accessed on 10 December 2022).
- Raghupathi, V.; Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public Health 2020, 78, 20. [Google Scholar] [CrossRef] [Green Version]
- Hahn, R.A.; Truman, B.I. Education Improves Public Health and Promotes Health Equity. Int. J. Health Serv. 2015, 45, 657–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenkorang, E.Y.; Maticka-Tyndale, E. Individual- and community-level influences on the timing of sexual debut among youth in Nyanza, Kenya. Int. Perspect. Sex. Reprod. Health 2014, 40, 68–78. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association (APA). Building Your Resilience. APA Psychological Topics. 2020. Available online: https://www.apa.org/topics/resilience/building-your-resilience (accessed on 22 October 2022).
- Liu, J.J.W.; Reed, M.; Girard, T.A. Advancing resilience: An integrative, multi-system model of resilience. Personal. Individ. Differ. 2017, 111, 111–118. [Google Scholar] [CrossRef]
- Li, X.; Qiao, S.; Yang, X.; Harrison, S.E.; Tam, C.C.; Shen, Z.; Zhou, Y. A Resilience-Based Intervention to Mitigate the Effect of HIV-Related Stigma: Protocol for a Stepped Wedge Cluster Randomized Trial. Front. Public Health 2022, 10, 857635. [Google Scholar] [CrossRef] [PubMed]
- Woodward, E.N.; Banks, R.J.; Marks, A.K.; Pantalone, D.W. Identifying Resilience Resources for HIV Prevention among Sexual Minority Men: A Systematic Review. AIDS Behav. 2017, 21, 2860–2873. [Google Scholar] [CrossRef]
- Colpitts, E.; Gahagan, J. The utility of resilience as a conceptual framework for understanding and measuring LGBTQ health. Int. J. Equity Health 2016, 15, 60. [Google Scholar] [CrossRef] [Green Version]
- Harrison, S.E.; Li, X.; Vermund, S.H. From surviving to thriving: The role of resilience in meeting global HIV goals. AIDS 2019, 33 (Suppl. S1), S1–S4. [Google Scholar] [CrossRef]
- Dale, S.K.; Safren, S.A. Resilience takes a village: Black women utilize support from their community to foster resilience against multiple adversities. AIDS Care 2018, 30, S18–S26. [Google Scholar] [CrossRef]
- McNair, O.S.; Gipson, J.A.; Denson, D.; Thompson, D.V.; Sutton, M.Y.; Hickson, D.A. The Associations of Resilience and HIV Risk Behaviors among Black Gay, Bisexual, Other Men Who Have Sex with Men (MSM) in the Deep South: The MARI Study. AIDS Behav. 2018, 22, 1679–1687. [Google Scholar] [CrossRef]
- Halkitis, P.N.; Krause, K.D.; Vieira, D.L. Mental Health, Psychosocial Challenges and Resilience in Older Adults Living with HIV. Interdiscip. Top. Gerontol. Geriatr. 2017, 42, 187–203. [Google Scholar]
- Green, D.C.; Wheeler, E.M. A Qualitative Exploration of Facilitators for Health Service Use among Aging Gay Men Living with HIV. J. Int. Assoc. Provid. AIDS Care 2019, 18, 2325958219880569. [Google Scholar] [CrossRef]
- Pebody, R. Impossible Routes of HIV Transmission. AIDsmap: HIV and AIDS-Sharing Knowledge Changing Lives. 2019. Available online: https://www.aidsmap.com/about-hiv/impossible-routes-hiv-transmission (accessed on 12 December 2022).
- Ilaria, G.; Jacobs, J.L.; Polsky, B.; Koll, B.; Baron, P.; MacLow, C.; Armstrong, D.; Schlegel, P.N. Detection of HIV-1 DNA sequences in pre-ejaculatory fluid. Lancet 1992, 340, 1469. [Google Scholar] [CrossRef] [PubMed]
- Pudney, J.; Oneta, M.; Mayer, K.; Seage, G.; Anderson, D. Pre-ejaculatory fluid as potential vector for sexual transmission of HIV-1. Lancet 1992, 340, 1470. [Google Scholar] [CrossRef] [PubMed]
- Centre for Disease Control (CDC). How is HIV Passed from One Person to Another? HIV Basics. 2022. Available online: https://www.cdc.gov/hiv/basics/hiv-transmission/ways-people-get-hiv.html (accessed on 22 December 2022).
- Makumbi, F.E.; Ssempijja, V.; Sekasanvu, J.; Ssekubugu, R.; Kigozi, G.; Watya, S.; Nakigozi, G.; Serwadda, D.; Wawer, M.; Gray, R.H. Postcoital penile washing and the risk of HIV acquisition in uncircumcised men. AIDS 2016, 30, 1669–1673. [Google Scholar] [CrossRef] [PubMed]
- National Health Service (NHS). HIV and AIDS Symptoms. HIV/AIDS. 2021. Available online: https://www.nhs.uk/conditions/hiv-and-aids/symptoms/ (accessed on 24 October 2022).
- Johns Hopkins Bloomberg School of Public Health. Why Don’t We Have an HIV Vaccine? Science Is Still Trying to Catch Up to the World’s Most Cunning Virus. 2022. Available online: https://publichealth.jhu.edu/2022/why-dont-we-have-an-hiv-vaccine (accessed on 12 December 2022).
- Cohen, M.S.; Council, O.D.; Chen, J.S. Sexually transmitted infections and HIV in the era of antiretroviral treatment and prevention: The biologic basis for epidemiologic synergy. J. Int. AIDS Soc. 2019, 22 (Suppl. S6), e25355. [Google Scholar] [CrossRef] [Green Version]
- CDC. What Are Condoms? HIV Basics. 2021. Available online: https://www.cdc.gov/hiv/basics/hiv-prevention/condoms.html (accessed on 12 December 2022).
- O’Halloran, C.; Croxford, S.; Mohammed, H.; Gill, O.N.; Hughes, G.; Fifer, H.; Allen, H.; Owen, G.; Nutland, W.; Delpech, V.; et al. Factors associated with reporting antibiotic use as STI prophylaxis among HIV PrEP users: Findings from a cross-sectional online community survey, May–July 2019, UK. Sex. Transm. Infect. 2020, 97, 429–433. [Google Scholar] [CrossRef]
- Obiero, J.; Ogongo, P.; Mwethera, P.G.; Wiysonge, C.S. Topical microbicides for preventing sexually transmitted infections. Cochrane Database Syst. Rev. 2021, 2021, CD007961. [Google Scholar]
- CDC. HIV Risk Reduction Tools. HIV Risk. 2020. Available online: https://hivrisk.cdc.gov/can-increase-hiv-risk/ (accessed on 20 July 2022).
- CDC. Understanding the HIV Window Period. 2022. Available online: https://www.cdc.gov/hiv/basics/hiv-testing/hiv-window-period.html (accessed on 12 December 2022).
- Seladi-Schulman, J.; Lillis, C. Can HIV Live and Spread Outside the Body? Medical News Today. 2020. Available online: https://www.medicalnewstoday.com/articles/324052 (accessed on 10 January 2023).

| Variables | Toronto n (%) | Ottawa n (%) | London n (%) | Windsor n (%) | β (Unadjusted Model) |
|---|---|---|---|---|---|
| City of residence | 343 (39.6) | 210 (24.3) | 157 (18.1) | 156 (18.0) | −0.05 |
| Country of birth | |||||
| Born in Canada | 98 (29.62) | 60 (28.85) | 37 (24.0) | 64 (41.6) | 0.11 |
| Born abroad | 238 (70.8) | 148 (71.15 | 117 (76.0) | 90 (58.4) | ref |
| Total valid responses | 336 (100) | 108 (100) | 154 (100) | 154 (100) | |
| Age categories (in years) | |||||
| 15–19 | 27 (7.9) | 42 (20.00) | 22 (14.0) | 11 (7.05) | 3.78 * |
| 20–29 | 94 (27.4) | 66 (31.43) | 47 (29.9) | 57 (36.54) | 1.14 |
| 30–39 | 100 (29.1) | 50 (23.81) | 42 (26.8) | 32 (20.51) | 0.65 |
| 40–49 | 60 (17.5) | 38 (18.1) | 25 (15.9) | 15 (9.61) | 1.18 |
| 50–59 | 27 (7.9) | 4 (1.9) | 17 (10.8) | 29 (18.59) | 0.65 |
| 60–64 | 19 (5.5) | 6 (2.86) | 3 (1.91) | 6 (3.85) | 1.63 |
| 65 and older | 16 (4.7) | 4 (1.9) | 1 (0.6) | 6 (3.85) | ref |
| Total valid responses | 343 (100) | 210 (100) | 157 (100) | 156 (100) | |
| Marital status | |||||
| Single | 151 (53.0) | 115 (54.8) | 81 (60.5) | 80 (51.28) | −0.13 |
| Married | 115 (40.3) | 60 (28.6) | 46 (34.3) | 44 (28.21) | −0.93 * |
| Others | 19 (6.7) | 35 (16.6) | 7 (5.2) | 32 (20.51) | ref |
| Total valid responses | 285 (100) | 210 (100) | 134 (100) | 156 (100) | |
| Education | |||||
| High school or lower education | 118 (34.8) | 64 (31.7) | 44 (28.8) | 36 (24.0) | 3.22 ** |
| College or university undergraduate | 178 (52.5) | 110 (54.4) | 77 (50.3) | 91 (60.7) | 0.65 |
| University graduate or professional degree | 43 (12.7) | 28 (13.9) | 32 (20.9) | 23 (15.3) | ref |
| Total valid responses | 339 (100) | 202 (100) | 153 (100) | 150 (100) | |
| Religious affiliation | |||||
| Muslim | 39 (12) | 32 (16.6) | 14 (9.5) | 9 (6) | −0.13 |
| Christian | 235 (71.9) | 132 (68.4) | 116 (78.9) | 124 (83.3) | −1.28 * |
| African traditional | 5 (1.5) | 5 (2.6) | 1 (0.7) | 0 (0) | −1.13 |
| Others | 5 (1.5) | 4 (2) | 2 (1.4) | 3 (2) | −0.46 |
| None | 43 (13.1) | 20 (10.4) | 14 (9.5) | 13 (8.7) | Ref |
| Total valid responses | 327 (100) | 193 (100) | 147 (100) | 149 (100) | |
| Employment status | |||||
| Employed (full time) | 177 (54.3) | 120 (60.6) | 59 (39.9) | 92 (60.9) | −1.1 ** |
| Employed (part time) | 45 (13.8) | 28 (14.1) | 26 (17.5) | 27 (17.9) | −0.71 |
| Unemployed | 104 (31.9) | 50 (25.3) | 63 (42.6) | 32 (21.2) | Ref |
| Total valid responses | 324 (100) | 198 (100) | 148 (100) | 151 (100) | |
| Pro-Black community attitudes score (m ± SD) | 15.7 ± 3.8 | 16.3 ± 4.0 | 15.9 ± 3.2 | 16.1 ± 3.2 | −0.07 |
| Resilience (m ± SD) | 58.6 ± 9.5 | 57.4 ± 8.4 | 58.9 ± 8.0 | 56.8 ± 8.8 | −0.07 *** |
| Everyday discrimination score (m ± SD) | 20.4 ± 6.4 | 20.4 ± 6.1 | 20.3 ± 6.3 | 17.9 ± 7.9 | −0.02 |
| Negative condom attitudes (score) | 25.4 ± 6.2 | 26.2 ± 5.8 | 24.6 ± 6.2 | 27.2 ± 6.0 | 0.08 ** |
| Age at sexual debut (m ± SD) | 17.1 ± 3.9 | 17.8 ± 6.3 | 19 ± 7 | 23.5 ± 15.4 | 0.03 |
| Score Categories | Toronto (n = 343) | Ottawa (n = 210) | London (n = 157) | Windsor (n = 156) | All Sites (N = 866) |
|---|---|---|---|---|---|
| None (0) | 3.5 (11.7) | 3.3 (11.9) | 3.8 (10.8) | 2.6 (13.5) | 3.3 (11.9) |
| (1–5) | 22.2 (6.1) | 22.9 (7.1) | 22.3 (4.5) | 26.3 (10.3) | 23.1(6.8) |
| (6–10) | 2.6 (17.2) | 3.3 (22.9) | 5.7 (16.6) | 1.9 (15.4) | 3.2 (18.1) |
| (>10) | 0.6 (65.0) | 2.4 (58.1) | 0.6 (68.2) | 0.0 (60.9) | 0.9 (63.2) |
| Misconception (%) | 25.4 | 28.6 | 28.6 | 28.2 | 27.2 |
| Outcome: HIV Misconceptions (Score) | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Predictors: | β | 95% CI | β | 95% CI |
| Country of birth dummy (Canada = 1, other countries = 0) | −1.06 * | −1.9, −0.22 | −0.96 * | −1.8, −0.12 |
| Employment status (employed full time = 1, others = 0) | 0.46 | −0.27, 1.19 | 0.46 | −0.24, 1.16 |
| Religion (non-religious = 1, otherwise = 0) | 0.39 | −0.83, 1.61 | 0.78 | −0.42, 1.98 |
| Education (more than high school = 1, high school or lower = 0) | −0.35 *** | −0.51, −0.19 | −0.37 * | −0.52, −0.21 |
| Resilience (score) | −0.04 * | −0.08, −0.01 | ||
| Discrimination (score) | 0.23 * | 0.01, 0.46 | ||
| Negative condom attitudes (score) | 0.07 * | 0.01, 0.12 | ||
| Positive pro-Black community attitudes (score) | 0.05 | −0.05, 0.14 | ||
| Age at sexual debut (years) | 0.06 * | 0.01, 0.1 | ||
| Model summary | ||||
| R2 change | 0.14 *** | 0.1 ** | ||
| Adjusted R2 | 0.12 *** | 0.2 *** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etowa, E.B.; Wong, J.P.-H.; Omorodion, F.; Etowa, J.; Luginaah, I. Addressing HIV Misconceptions among Heterosexual Black Men and Communities in Ontario. Healthcare 2023, 11, 997. https://doi.org/10.3390/healthcare11070997
Etowa EB, Wong JP-H, Omorodion F, Etowa J, Luginaah I. Addressing HIV Misconceptions among Heterosexual Black Men and Communities in Ontario. Healthcare. 2023; 11(7):997. https://doi.org/10.3390/healthcare11070997
Chicago/Turabian StyleEtowa, Egbe B., Josephine Pui-Hing Wong, Francisca Omorodion, Josephine Etowa, and Isaac Luginaah. 2023. "Addressing HIV Misconceptions among Heterosexual Black Men and Communities in Ontario" Healthcare 11, no. 7: 997. https://doi.org/10.3390/healthcare11070997