3.2. Participants’ Awareness of CAMs
A total of 63.0% (
n = 226) of participants had tried CAM approaches, and the most preferred method was phytotherapy with 50% (
n = 113), followed by aromatherapy with 44.2% (
n = 100), and apitherapy with 37.6% (
n = 85). While 38.7% (
n = 139) of the participants thought that CAM is helpful, 4.5% (16) believed that it is not at all useful. When the respondents were asked where they had learned and tried CAM methods, 27.9% said they were advised by a doctor; 22.8% said they received advice from family, friends, or neighbors; 22.6% were advised by a pharmacist; 21.2% had seen information on the Internet or television and tried it; and 4.7% said they tried it because they had seen information in a newspaper or magazine. When respondents were asked about the number of places providing complementary and alternative treatment services and the adequacy of the educational status of the practitioners providing CAM treatment services, 53.8% (
n = 193) stated that the number of places was insufficient. In contrast, 30.4% of the same participants thought that the knowledge of CAM providers is insufficient. When the respondents were asked why they used CAM, 40.7% (
n = 146) used it as an immune booster, followed by 22% (
n = 79) for sleeping disorders stress, 20.9% (
n = 79) for burnout syndrome, and 20.6% (
n = 74) for lumbar hernia, rheumatism, musculoskeletal disorders, etc., as listed in
Table 2.
3.3. Use of and Public Attitudes towards HPs
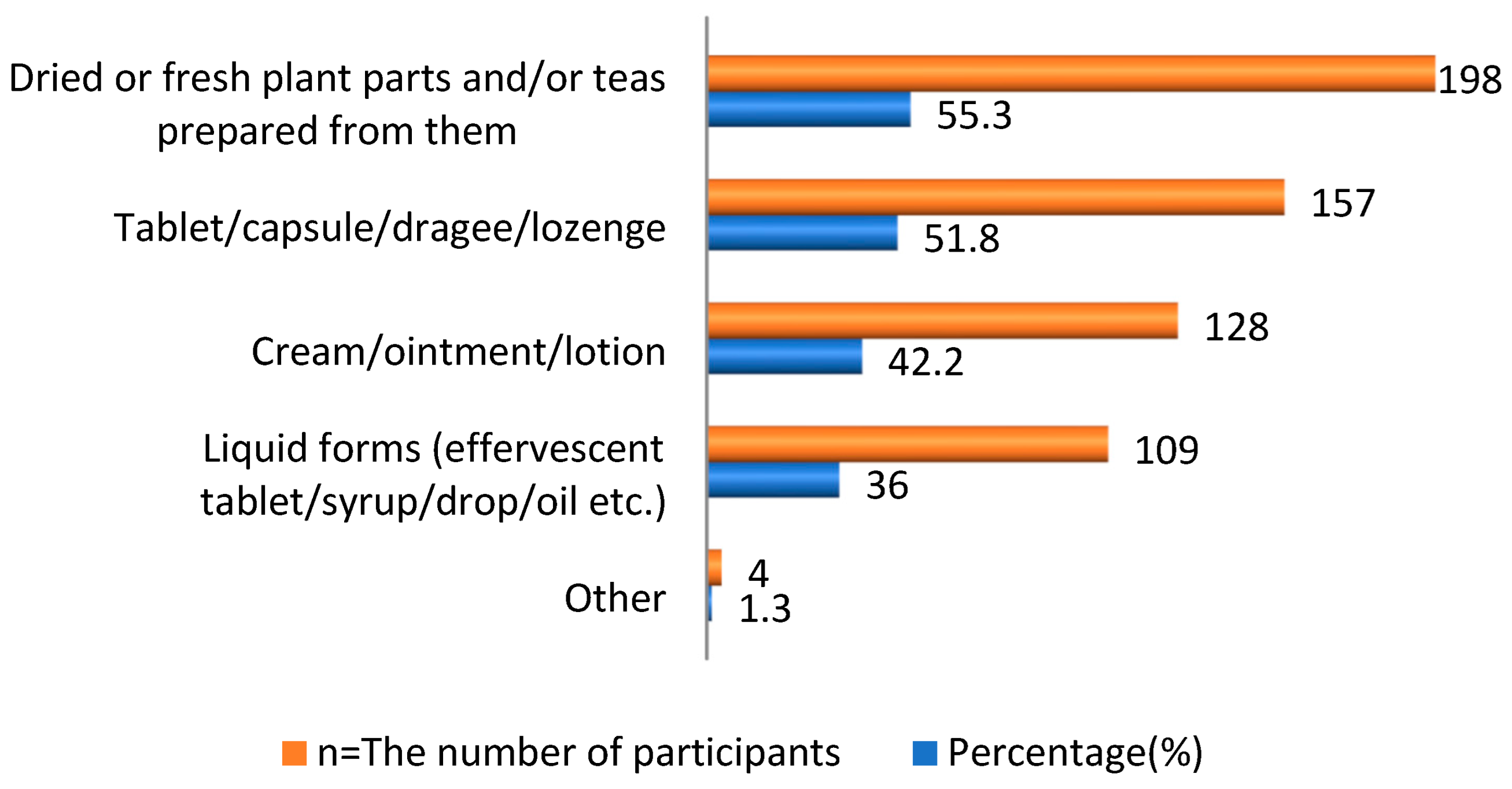
Considering the use of HPs, 303 participants (84.40%) had used at least one herbal product. As for the preferred format of the HPs, 157 (51.8%) participants preferred solid forms, such as tablets, capsules, dragees, or lozenges, and 198 (55.3%) participants preferred dried or fresh plant parts and/or tea prepared from them as shown in
Figure 1. The most preferred HPs were fennel (
n = 208, 57.9%), ginger (
n = 181, 50.4%), and echinacea (
n = 146, 40.7%), as indicated in
Table 3.
It was observed that the participants’ main purpose when using HPs was to prevent sickness and protect health (
n = 251, 69.9%). While the number of participants who used HPs to cure an existing disease was 125 (34.8%), the number of those who used HPs to prevent the symptoms of their disease was 132 (36.8%). The majority of the respondents thought that HPs are natural, harmless, and chemical-free (
n = 187, 52.1%) or that the risks of side effects, drug interactions, and allergies are very low (
n = 95, 26.5%), as shown in
Table 4.
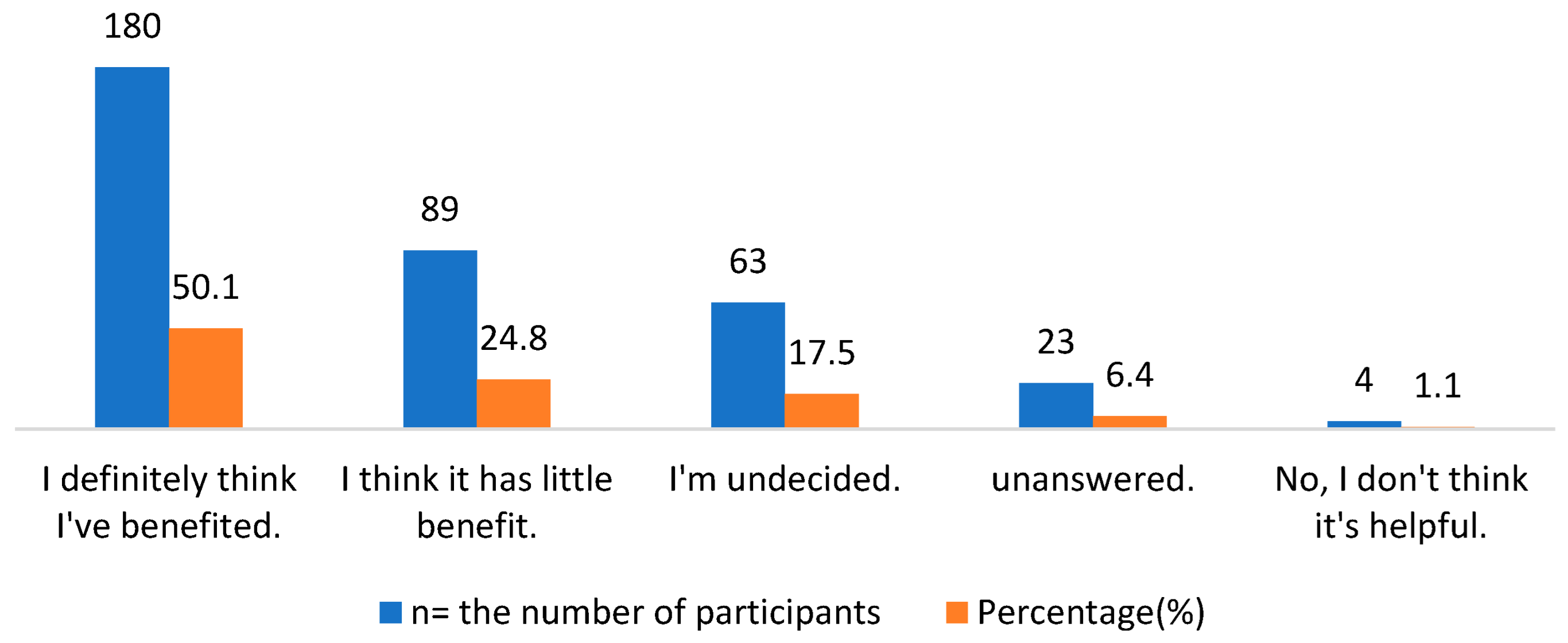
Among the respondents, 180 participants (50.1%) thought that the HPs they use are beneficial according to their intended use, while 89 (24.8%) thought they provide minimal benefit, as illustrated in
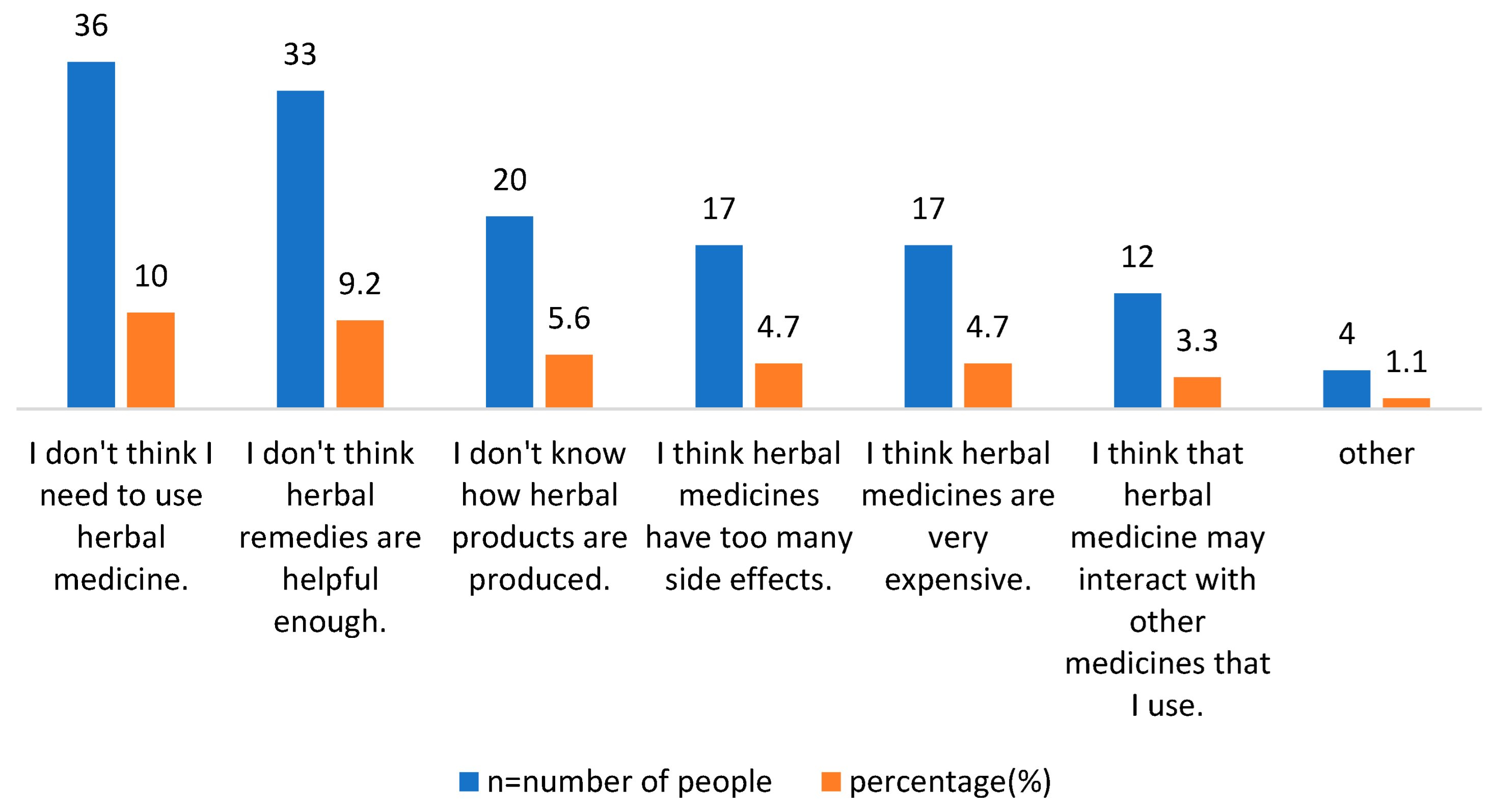
Figure 2. Moreover, the authors asked the respondents about their reasons for not using herbal products. As shown in
Figure 3, 10% of the participants thought that they do not need to use herbal products, 9.2% thought that herbal products are not useful enough, and 5.6% expressed reluctance to take such supplements because they do not know the production conditions of herbal products. Some 4.7% of respondents thought that products are very expensive, and 4.7% of them said they do not use such products because of the possible side effects of herbal products. Finally, it was observed that 3.3% of the participants did not use such products because they thought that the herbal products might interact with the conventional drugs they were currently using.
The number of participants with chronic diseases among the survey participants was 107 (29.8%). When asked if they would inform their doctor/pharmacist about the HPs they use, of the 67 participants who used conventional medicine as well as HPs for their chronic disease, the majority (
n = 43, 64.2%) said they would do so (
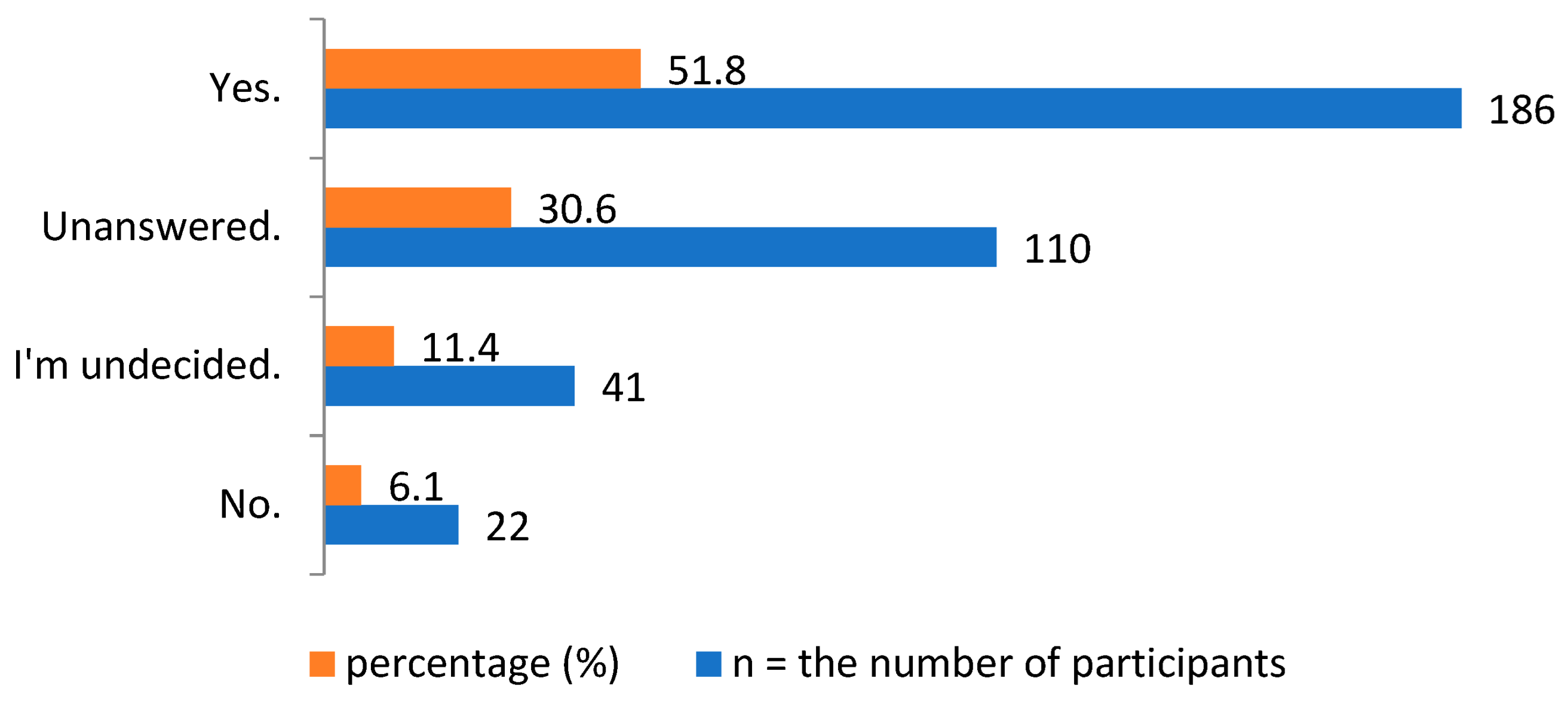
Table 5). The respondents were asked if they would use HPs in addition to conventional medicine if recommended by their doctor or pharmacist to. While 186 participants (51.8%) said yes, 22 participants (6.1%) stated that they would not use them, as shown in
Figure 4.
Furthermore, when the respondents were asked whether herbal medicines/products are as effective as the conventional medicines currently on the market in the treatment of certain diseases, 55.2% (
n = 198) of the respondents said they were partially effective, while 25.1% (
n = 90) said they were effective, and 1.9% (
n = 7) stated that they are not effective at all. It was observed that the respondents mostly preferred to use HPs in cases, such as cold, flu, cough, etc. (
n = 278, 77.4%), and to strengthen the immune system (
n = 234, 65.2%), as indicated in
Table 6.
When asked about the most effective factors in the use of HPs, 61.6% of the participants said that a doctor’s advice (n = 221) and 56.5% cited a pharmacist’s advice (n = 203) as the most important factors, while the Internet (n = 139, 38.7%) and neighbor/friend/family recommendations (n = 113, 31.5%) were also found to be other effective factors.
After deciding to use the product, 71% (n = 255) of the participants said that they would consult their pharmacist about the product when asked about the methods they would use to collect information, while 53.8% (n = 193) said they would consult their doctor, and 52.9% (n =190) stated they would gather information from the Internet. The proportion of those who said they would ask their neighbors and/or friends who had used the product about their experience was 22.3% (n = 80), while the rate of those who said they would use it without conducting any research was 1.9% (n = 7).
When asked which factors were important when buying HPs, 71% (
n = 255) cited their pharmacist’s suggestions, 65.5% (
n = 235) said their doctor’s suggestions, 47.6% (
n = 171) looked at the manufacturer brand HPs, 20.9% (
n = 75) said the price, and 8.1% (
n = 29) said advertisements on the Internet and television. Considering the distribution of HP use according to age, gender, education level, and income level, people with a master’s degree or higher education level preferred fewer HPs than those whose with less education, 78.5% to 88.16%, respectively. Individuals between the ages of 36and 45 were the most likely to use herbal products (88.8%). However, when the effect of age, education level, gender, and income status on the use of HPs was examined, no statistically significant difference was found (
Table 7).
In addition, Chi-square tests were performed for the comparisons made in
Table 7. Significant associations (
p-value < 0.05) were found between education level and HP use status. Additionally, there was no significant difference between age and HP use (χ
2 = 2.665,
p = 0.264 > 0.05) as patients used HPs regardless of age. As a result of the Chi-square test, no significant difference was found between the gender variable and HP use status (χ
2 = 0.272,
p = 0.602 > 0.05) as patients used HPs regardless of gender. There was no significant difference between the income variable and HP use status (χ
2 = 5.515,
p = 0.238 > 0.05). In other words, patients used HP regardless of their income level.
Moreover,
Table 8 presents responses regarding the average monthly budget for the herbal products used. It was found that women spent more money than men, and the difference was statistically significant (χ
2 = 6.575 a,
p = 0.037 > 0.05). As for the effect of education, 44.7% of individuals with graduate and higher education levels spent TL 150 or more on herbal products, while this rate was 30.2% for individuals with university degrees, and only 23.7% for those with a high school education. The difference was found to be statistically significant (χ
2 = 14.125 a,
p = 0.007 > 0.05).
3.5. Qualitative Findings of the Study-Interview Analysis
In this section, the findings were interpreted by obtaining study participants’ on herbal products and complementary and alternative medicines from a qualitative point of view.
The interview content analysis identified three main themes: (a) familiarity and understanding of CAM; (b) attitudes and perceived benefits; and (c) disclosure to the physician. Each topic with illustrative excerpts from patients’ texts is described below.
Theme 1: Familiarity and understanding of complementary and alternative medicine.
Patients were asked about their use of any alternative therapies to the approved standard of care.
“I took my treatment as my doctor said, but I prefer to use some herbal and vitamins with it because they make me feel better and they are good… I also tried some dietary supplements to improve my health in general”.
“Yes, sometimes I drink herbs and lemon juice when I feel that my pressure is high. Also, I do use CAM from time to time and I feel better after doing it”.
Only a small number of patients claimed that they adhere to the therapy advised by the doctor and have never attempted any alternative method; nevertheless, they said they follow a diet restriction program.
“No, I’ve never attempted anything other than the doctor-prescribed therapy... Because they have not been evaluated and I am unsure of the potential consequences of using them, I do not trust products like herbs or CAM therapies. I altered my diet and took the required medications.”
Some patients explained why they were seeking such therapies. The majority cited affordability, safety, religious difficulties, and advice from friends.
“My friend advised me to use one of the CAMs to treat hypertension, and when I tried it, I felt good without the need to use medicines”.
“Natural products are not manufactured by a human; they have been found in nature for our benefit since the beginning of life. They are like our food, they are also cheap and not like manufactured drugs which are very expensive and may result in harm to the patients”.
The interviews revealed that respondents in this study were unfamiliar with the term CAMs; instead, they knew this sort of therapy as herbal medicine.
“No, I’ve never heard of this name before, but I know this therapy is known as herbal medicine. No, I was unaware of this before... But, I have heard about alternative medications on television and believe they are the same as herbal remedies”.
Theme 2: Attitudes and perceived benefits of complementary and alternative medicine.
The majority of individuals utilized a range of CAM products for hypertension. Among the most frequently suggested items were garlic, lemon, vitamins, and nutritional supplements. However, the data do not indicate the initial product used by each participant, as the majority of them had utilized many types of CAM at the same time and since their diagnosis.
“I have used different things since I found out I have hypertension… I drink lemon; also, I take some food supplements with garlic, ginger, and vitamins…”.
Pharmacists and friends were the main sources of information regarding CAM. Furthermore, the respondents said that they could easily obtain such products from the markets, herbalists, and community pharmacies at reasonable prices.
“I got them from the pharmacy… I prefer to ask the pharmacist about them because he knows more about the medicines and herbs”.
“Herbal medicine has been known since ancient times and when I need to use it or need any advice, I ask older people or the pharmacist sometimes”.
Patients perceived that CAM therapy is effective in lowering high blood pressure based on regular use. Another noted perception was that CAM is a safe practice and free from any side effects.
“Yes, it is an effective treatment and gives good results, but you have to take it continuously… If you leave it for a long time, maybe you will not get any benefit from it. It needs time to lower the blood pressure”.
“I think they are safe, without any harmful effects… Our religion encourages us to do it. Reflexology is also good and safe as I have tried it before without any bad results”.
Theme 3: Communication with the physicians and other medical staff.
The last theme suggested that respondents did not disclose CAM practices to their doctors. In most cases, the respondents said they tend to use CAM despite their standard prescribed treatment. Reasons for nondisclosure were short counseling time, fear of the doctors’ anger, and lack of CAM recognition.
In this study, CAM users said they preferred to consult their pharmacist about CAM-related information. “I buy the herbs from the pharmacy and ask the pharmacist about the preparation and use. I think the pharmacist is the best person to obtain information about the treatment and herbal medicines because drugs were originally made from herbs”.
“Concerning CAM, I learned about it from TV shows and from reading about it on the Internet. I sometimes contact the elderly since they have experience dealing with it”.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}