
Psychosocial Work Stress and Occupational Stressors in Emergency Medical Services

Abstract
:1. Introduction
2. Materials and Methods
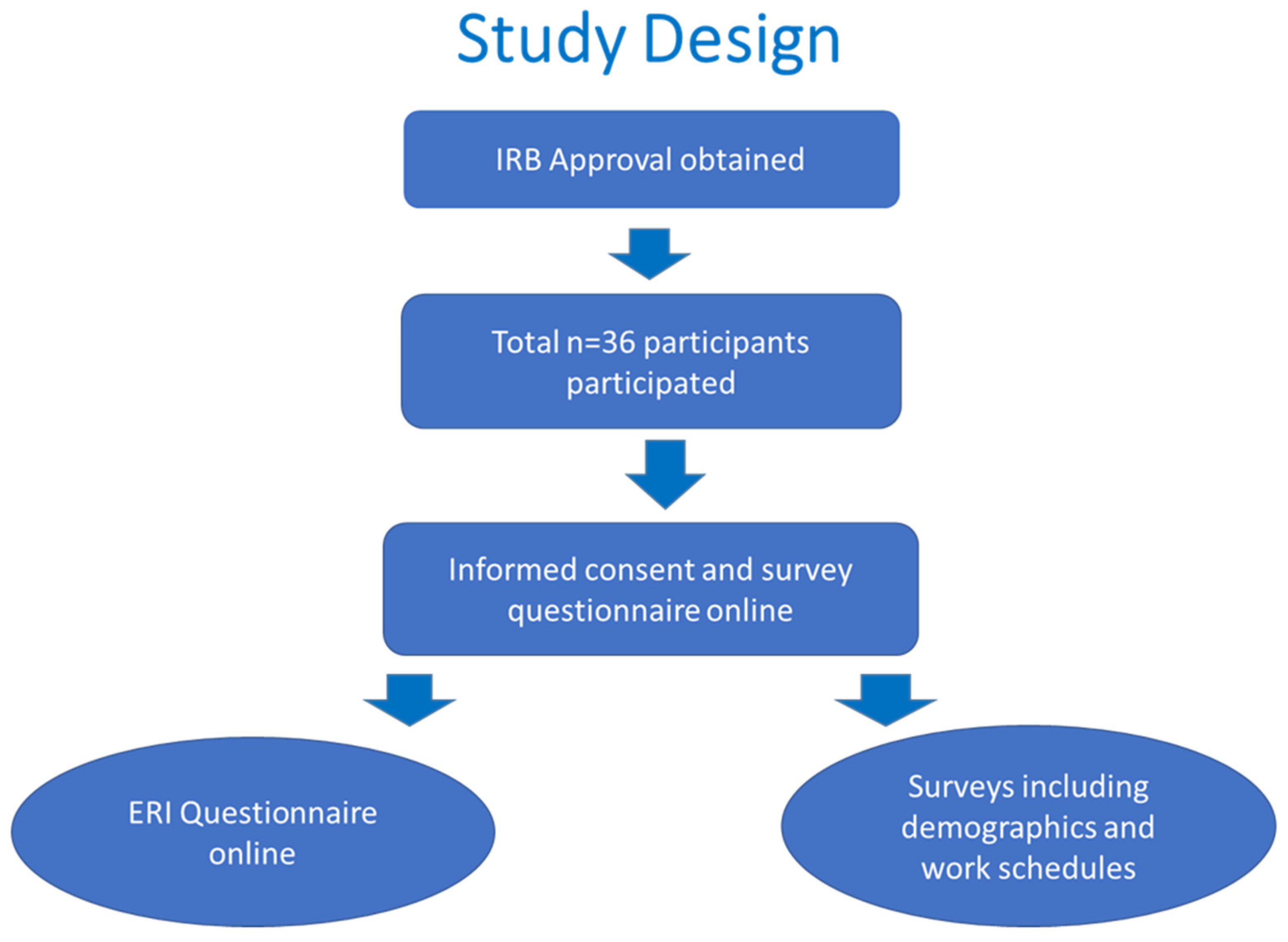
2.1. Study Design
2.2. Evaluation of Job Stress Using the Effort–Reward Imbalance Model
2.3. Statistical Analysis
3. Results
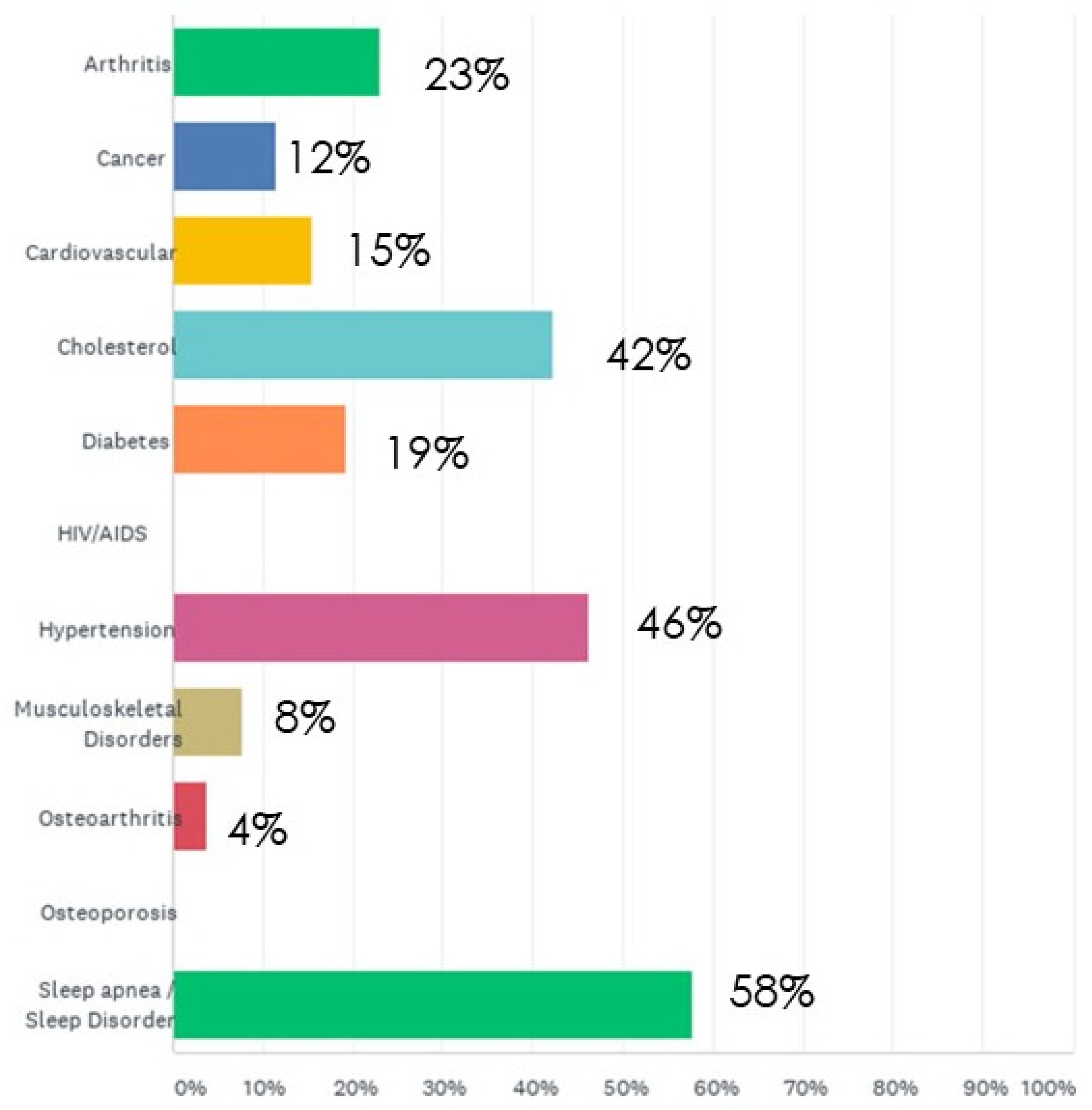
3.1. Participant Characteristics
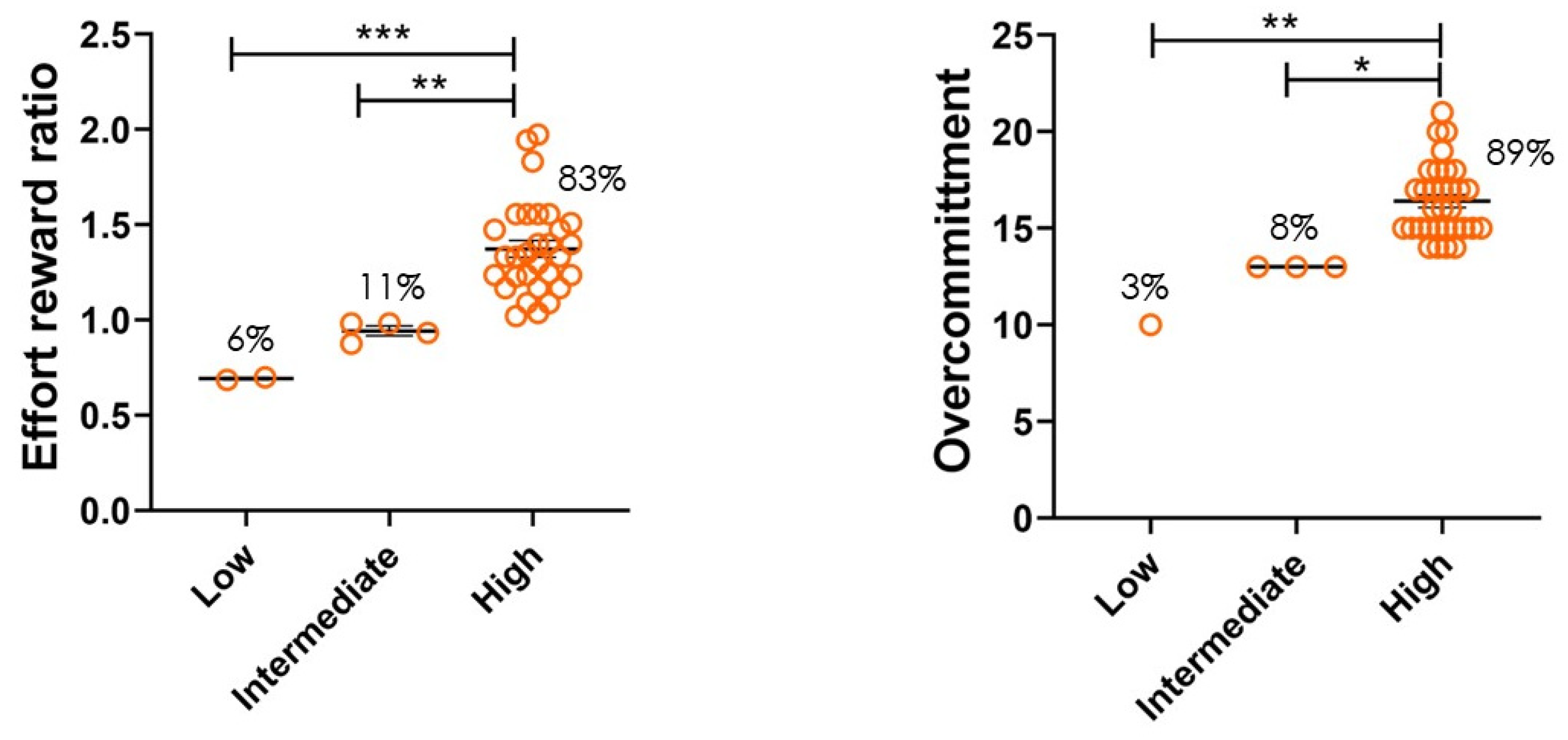
3.2. Job Stress Indicators
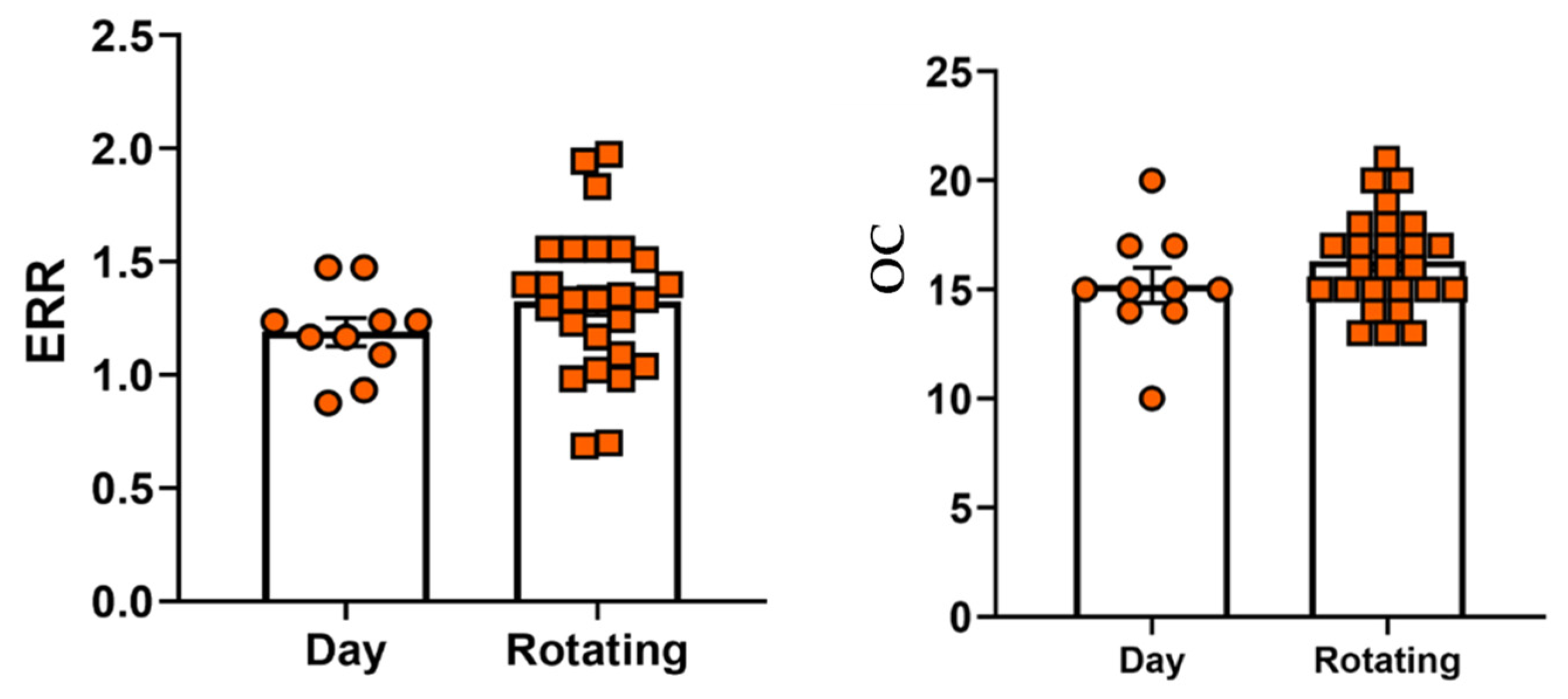
3.3. Sleep Apnea, Shiftwork, and Job Stress Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neale, A.V. Work stress in emergency medical technicians. J. Occup. Med. 1991, 33, 991–997. [Google Scholar] [PubMed]
- Afshari, A.; Borzou, S.R.; Shamsaei, F.; Mohammadi, E.; Tapak, L. Perceived occupational stressors among emergency medical service providers: A qualitative study. BMC Emerg. Med. 2021, 21, 35. [Google Scholar] [CrossRef] [PubMed]
- Tunaligil, V.; Dokucu, A.I.; Erdogan, M.S. Determinants of General Health, Work-Related Strain, and Burnout in Public Versus Private Emergency Medical Technicians in Istanbul. Workplace Health Saf. 2016, 64, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boland, L.L.; Kinzy, T.G.; Myers, R.N.; Fernstrom, K.M.; Kamrud, J.W.; Mink, P.J.; Stevens, A.C. Burnout and Exposure to Critical Incidents in a Cohort of Emergency Medical Services Workers from Minnesota. West J. Emerg. Med. 2018, 19, 987–995. [Google Scholar] [CrossRef]
- Amro, T.M.; Arcos Gonzalez, P.; Montero Vinuales, E.; Castro Delgado, R. Impact of COVID-19 Pandemic on Stress and Burnout Levels amongst Emergency Medical Technicians: A Cross-Sectional Study in Spain. Ann. Med. 2022, 54, 3007–3016. [Google Scholar] [CrossRef] [PubMed]
- Chavez, S.; Crowe, R.; Huebinger, R.; Chan, H.K.; Gill, J.; Villa, N.; Pancyzk, M.; Jarvis, J.; Bobrow, B. Perspective of emergency medical services (EMS) professionals on changes in resources, cardiac arrest care and burnout in Texas during the COVID-19 pandemic. Am. J. Emerg. Med. 2022, 62, 118–122. [Google Scholar] [CrossRef]
- Di Giuseppe, M.; Nepa, G.; Prout, T.A.; Albertini, F.; Marcelli, S.; Orru, G.; Conversano, C. Stress, Burnout, and Resilience among Healthcare Workers during the COVID-19 Emergency: The Role of Defense Mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef]
- Lau, B. Effort-reward imbalance and overcommitment in employees in a Norwegian municipality: A cross sectional study. J. Occup. Med. Toxicol. 2008, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Parvaresh-Masoud, M.; Imanipour, M.; Cheraghi, M.A. Emergency Medical Technicians’ Experiences of the Challenges of Prehospital Care Delivery During the COVID-19 Pandemic: A Qualitative Study. Ethiop. J. Health Sci. 2021, 31, 1115–1124. [Google Scholar] [CrossRef]
- Mohammadi, F.; Tehranineshat, B.; Bijani, M.; Khaleghi, A.A. Management of COVID-19-related challenges faced by EMS personnel: A qualitative study. BMC Emerg. Med. 2021, 21, 95. [Google Scholar] [CrossRef]
- Bailey, I. COVID-19 Stress Pushing More Paramedics to Seek Mental-Health Support in B.C. Phillip Crawley, Publisher and CEO. The Globe and Mail Centre 351 King Street East Suite 1600 Toronto, Ontario M5A 0N1. In The Globe and Mail. 2020. Available online: https://www.theglobeandmail.com/canada/british-columbia/article-covid-19-stress-pushing-more-paramedics-to-seek-mental-health-support/ (accessed on 1 February 2023).
- CDC. Optimizing Supply of PPE and Other Equipment during Shortages; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Hu, N.C.; Chen, J.D.; Cheng, T.J. The Associations Between Long Working Hours, Physical Inactivity, and Burnout. J. Occup. Environ. Med. 2016, 58, 514–518. [Google Scholar] [CrossRef]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Chu, H.; Chen, R.; Liu, D.; Banda, K.J.; O’Brien, A.P.; Jen, H.J.; Chiang, K.J.; Chiou, J.F.; Chou, K.R. Prevalence of depression, anxiety, and stress among first responders for medical emergencies during COVID-19 pandemic: A meta-analysis. J. Glob. Health 2022, 12, 05028. [Google Scholar] [CrossRef]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Bude, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.J.; Huang, K.C.; Wu, C.H. Determination of sample size in using central limit theorem for weibull distribution. Int. J. Inf. Manag. Sci. 2006, 17, 153–174. [Google Scholar]
- Siegrist, J. Effort-reward imbalance at work and cardiovascular diseases. Int. J. Occup. Med. Environ. Health 2010, 23, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Siegrist, J.; Wege, N.; Puhlhofer, F.; Wahrendorf, M. A short generic measure of work stress in the era of globalization: Effort-reward imbalance. Int. Arch. Occup. Environ. Health 2009, 82, 1005–1013. [Google Scholar] [CrossRef]
- Stanhope, J. Effort–Reward Imbalance Questionnaire. Occup. Med. 2017, 67, 314–315. [Google Scholar] [CrossRef] [Green Version]
- CDC/NIOSH. The Challenge of Underreporting; The National Institute for Occupational Safety and Health (NIOSH), Ed.; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Bureau of Labor Statistics. EMTs and Paramedics; US Department of Labor, Ed.; Occupational Outlook Handbook: Washington, DC, USA, 2023. Available online: https://www.bls.gov/ooh/healthcare/emts-and-paramedics.htm (accessed on 18 January 2023).
- Bridgeman, P.J.; Bridgeman, M.B.; Barone, J. Burnout syndrome among healthcare professionals. Am. J. Health Syst. Pharm. 2018, 75, 147–152. [Google Scholar] [CrossRef]
- Nishimura, Y.; Miyoshi, T.; Sato, A.; Hasegawa, K.; Hagiya, H.; Kosaki, Y.; Otsuka, F. Burnout of Healthcare Workers Amid the COVID-19 Pandemic: A Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 1581. [Google Scholar] [CrossRef]
- Tan, B.Y.Q.; Kanneganti, A.; Lim, L.J.H.; Tan, M.; Chua, Y.X.; Tan, L.; Sia, C.H.; Denning, M.; Goh, E.T.; Purkayastha, S.; et al. Burnout and Associated Factors Among Health Care Workers in Singapore During the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 1751–1758.e1755. [Google Scholar] [CrossRef]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations. Arch. Acad. Emerg. Med. 2021, 9, e7. [Google Scholar] [CrossRef] [PubMed]
- Dimitriu, M.C.T.; Pantea-Stoian, A.; Smaranda, A.C.; Nica, A.A.; Carap, A.C.; Constantin, V.D.; Davitoiu, A.M.; Cirstoveanu, C.; Bacalbasa, N.; Bratu, O.G.; et al. Burnout syndrome in Romanian medical residents in time of the COVID-19 pandemic. Med. Hypotheses 2020, 144, 109972. [Google Scholar] [CrossRef] [PubMed]
- Raudenska, J.; Steinerova, V.; Javurkova, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef]
- Sultana, A.; Sharma, R.; Hossain, M.M.; Bhattacharya, S.; Purohit, N. Burnout among healthcare providers during COVID-19: Challenges and evidence-based interventions. Indian J. Med. Ethics 2020, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- De Simone, S.; Vargas, M.; Servillo, G. Organizational strategies to reduce physician burnout: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Markaki, A.; Baird, J.; Murray, P.; Edwards, R. Addressing Healthcare Professional Burnout: A Quality Improvement Intervention. Worldviews Evid. Based Nurs. 2020, 17, 213–220. [Google Scholar] [CrossRef]
- Awais, S.B.; Martins, R.S.; Khan, M.S. Paramedics in pandemics: Protecting the mental wellness of those behind enemy lines. Br. J. Psychiatry 2021, 218, 75–76. [Google Scholar] [CrossRef]
- Dopelt, K.; Wacht, O.; Strugo, R.; Miller, R.; Kushnir, T. Factors that affect Israeli paramedics’ decision to quit the profession: A mixed methods study. Isr. J. Health Policy Res. 2019, 8, 78. [Google Scholar] [CrossRef] [Green Version]
- Hruska, B.; Barduhn, M.S. Dynamic psychosocial risk and protective factors associated with mental health in Emergency Medical Service (EMS) personnel. J. Affect Disord. 2021, 282, 9–17. [Google Scholar] [CrossRef]
- Ventura, C.A.I.; Denton, E.E.; David, J.A.; Schoenfelder, B.J.; Mela, L.; Lumia, R.P.; Rudi, R.B.; Haldar, B. Emergency Medical Services Prehospital Response to the COVID-19 Pandemic in the US: A Brief Literature Review. Open Access Emerg. Med. 2022, 14, 249–272. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Ong, M.E.; Cho, J.; Ma, M.H.; Tanaka, H.; Nishiuchi, T.; Al Sakaf, O.; Abdul Karim, S.; Khunkhlai, N.; Atilla, R.; Lin, C.H.; et al. Comparison of emergency medical services systems in the pan-Asian resuscitation outcomes study countries: Report from a literature review and survey. Emerg. Med. Australas 2013, 25, 55–63. [Google Scholar] [CrossRef]
- Carlson, J.N.; Karns, C.; Mann, N.C.; Karen, E.J.; Dai, M.; Colleran, C.; Wang, H.E. Procedures Performed by Emergency Medical Services in the United States. Prehosp. Emerg. Care 2016, 20, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Tomasz, I.; Małgorzata, R.; Ćwiertnia, M.; Mikulska, M.; Waksmańska, W.; Krakowiak, A.; Bobiński, R.; Kawecki, M. Predictors of stress among emergency medical personnel during the COVID-19 pandemic. Int. J. Occup. Med. Environ. Health 2021, 34, 139–149. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Sun, J.T.; Chang, H.P.; Chen, Y.L.; Pei, D.; Liang, Y.J. Investigation of Psychological Stress and Sleep Quality of Emergency Medical Technicians in Taiwan Fire Department during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 20, 137. [Google Scholar] [CrossRef]
- McHugh, M.; French, D.D.; Kwasny, M.M.; Maechling, C.R.; Holl, J.L. The Impact of Shift Work and Long Work Hours on Employers’ Health Care Costs. J. Occup. Environ. Med. 2020, 62, 1006–1010. [Google Scholar] [CrossRef]
- Rivera, A.S.; Akanbi, M.; O’Dwyer, L.C.; McHugh, M. Shift work and long work hours and their association with chronic health conditions: A systematic review of systematic reviews with meta-analyses. PLoS ONE 2020, 15, e0231037. [Google Scholar] [CrossRef] [PubMed]
- Bardinelli, J.A.; Roarty, J.; Goldstein, S. EMS Disordered Sleep And Work Schedule; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand J. Work Environ. Health 2018, 44, 229–238. [Google Scholar] [CrossRef] [Green Version]
- Khan, W.A.A.; Conduit, R.; Kennedy, G.A.; Jackson, M.L. The relationship between shift-work, sleep, and mental health among paramedics in Australia. Sleep Health 2020, 6, 330–337. [Google Scholar] [CrossRef]
- Laudencka, A.; Klawe, J.J.; Tafil-Klawe, M.; Złomańczuk, P. Does night-shift work induce apnea events in obstructive sleep apnea patients? J. Physiol. Pharmacol. 2007, 58, 345–347. [Google Scholar]
- Lies, J.; Mellor, A.; Jobson, L.; Drummond, S.P.A. Prevalence of sleep disturbance and its relationships with mental health and psychosocial issues in refugees and asylum seekers attending psychological services in Australia. Sleep Health 2019, 5, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Luken, M.; Sammons, A. Systematic Review of Mindfulness Practice for Reducing Job Burnout. Am. J. Occup. Ther. 2016, 70, 7002250020p1–7002250020p10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, A.A.; Kinchen, E.V. The Effects of Mindfulness Meditation on Stress and Burnout in Nurses. J. Holist. Nurs. 2021, 39, 356–368. [Google Scholar] [CrossRef]
- Burton, A.; Burgess, C.; Dean, S.; Koutsopoulou, G.Z.; Hugh-Jones, S. How Effective are Mindfulness-Based Interventions for Reducing Stress among Healthcare Professionals? A Systematic Review and Meta-Analysis. Stress Health 2017, 33, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, A.A. The Psychological Challenges of Emergency Medical Service Providers During Disasters: A Mini-Review. Front. Psychiatry 2022, 13, 773100. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 36) n% or Mean (SD) * | Median (Range) |
|---|---|---|
| Age (years) * | 39.028 (10.722) | 39 (20–65) |
| Sex | ||
| Female | 10 (28) | |
| Male | 26 (72) | |
| BMI * | 31.633 (7.863) | 30.2 (18–56.1) |
| Marital Status | ||
| Married | 23 (64) | |
| Single | 13 (36) | |
| Shiftwork | ||
| Dayshift | 10 (28) | |
| Rotating shift | 26 (72) | |
| Weekend Work | ||
| Yes | 31 (86) | |
| No | 5 (14) | |
| Continuous Work hours/week | ||
| ≤12 | 15 (42) | |
| ≥24 | 21 (58) | |
| ERR * | 1.287 (0.298) | 1.270 (0.686–1.97) |
| OC * | 15.944 (2.254) | 15.5 (10–21) |
| Characteristics | OR (95% CI) | p Value |
|---|---|---|
| Age (years) | ||
| ≤40 | 1.00 (Reference) | |
| >40 | 3.002 (0.265–33.970) | 0.374 |
| Sex | ||
| Female | 0.355 (0.012–10.370) | 0.547 |
| Male | 1.00 (Reference) | |
| Marital Status | ||
| Married | 0.000 (0.000) | 0.998 |
| Single | 1.00 (Reference) | |
| Weekend Work | ||
| Yes | 0.000 (0.000) | 0.999 |
| No | 1.00 (Reference) | |
| Continuous Work hours/week | ||
| ≤12 | 1.00 (Reference) | |
| ≥24 | 12.565 (0.223–709.28) | 0.219 |
| BMI | ||
| Obese (≥30) | 0.000 (0.000) | 0.999 |
| Overweight (25.0–29.9) | 0.000 (0.000) | 0.999 |
| Normal (<25) | 1.00 (Reference) |
| Characteristics | OR (95% CI) | p Value |
|---|---|---|
| Age (years) | ||
| ≤40 | 1.00 (Reference) | |
| >40 | 0.305 (0.015–6.232) | 0.440 |
| Sex | ||
| Female | 1.317 (0.068–25.629) | 0.856 |
| Male | 1.00 (Reference) | |
| Marital Status | ||
| Married | 1.835 (0.114–29.589) | 0.669 |
| Single | 1.00 (Reference) | |
| Weekend Work | ||
| Yes | 0.000 (0.000) | 0.999 |
| No | 1.00 (Reference) | |
| Continuous Work hours/week | ||
| ≤12 | 1.00 (Reference) | |
| ≥24 | 2.296 (0.161–32.804) | 0.540 |
| BMI | ||
| Obese (≥30) | 8.221 (0.210–321.406) | 0.260 |
| Overweight (25.0–29.9) | 4.723 (0.129–172.821) | 0.398 |
| Normal (<25) | 1.00 (Reference) |
| Variables | Pearson r | 95% CI | R Squared | p (Two Tailed) |
|---|---|---|---|---|
| ERR vs. Sleep Apnea | 0.3949 | 0.07623–0.6403 | 0.1559 | 0.0172 * |
| OC vs. Sleep Apnea | 0.5534 | 0.2748–0.7463 | 0.3063 | 0.0005 * |
| ERR vs. Sleep Apnea in Rotating Shift Employees | 0.5731 | 0.2387–0.7860 | 0.3284 | 0.0022 * |
| OC vs. Sleep Apnea in Rotating Shift Employees | 0.5623 | 0.2236–0.7798 | 0.3161 | 0.0028 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardhan, R.; Byrd, T. Psychosocial Work Stress and Occupational Stressors in Emergency Medical Services. Healthcare 2023, 11, 976. https://doi.org/10.3390/healthcare11070976
Bardhan R, Byrd T. Psychosocial Work Stress and Occupational Stressors in Emergency Medical Services. Healthcare. 2023; 11(7):976. https://doi.org/10.3390/healthcare11070976
Chicago/Turabian StyleBardhan, Rupkatha, and Traci Byrd. 2023. "Psychosocial Work Stress and Occupational Stressors in Emergency Medical Services" Healthcare 11, no. 7: 976. https://doi.org/10.3390/healthcare11070976