
Challenges, Concerns, and Experiences of Community-Dwelling Older Women with Chronic Low Back Pain—A Qualitative Study in Hong Kong, China
 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Interviews
2.3. Data Analysis
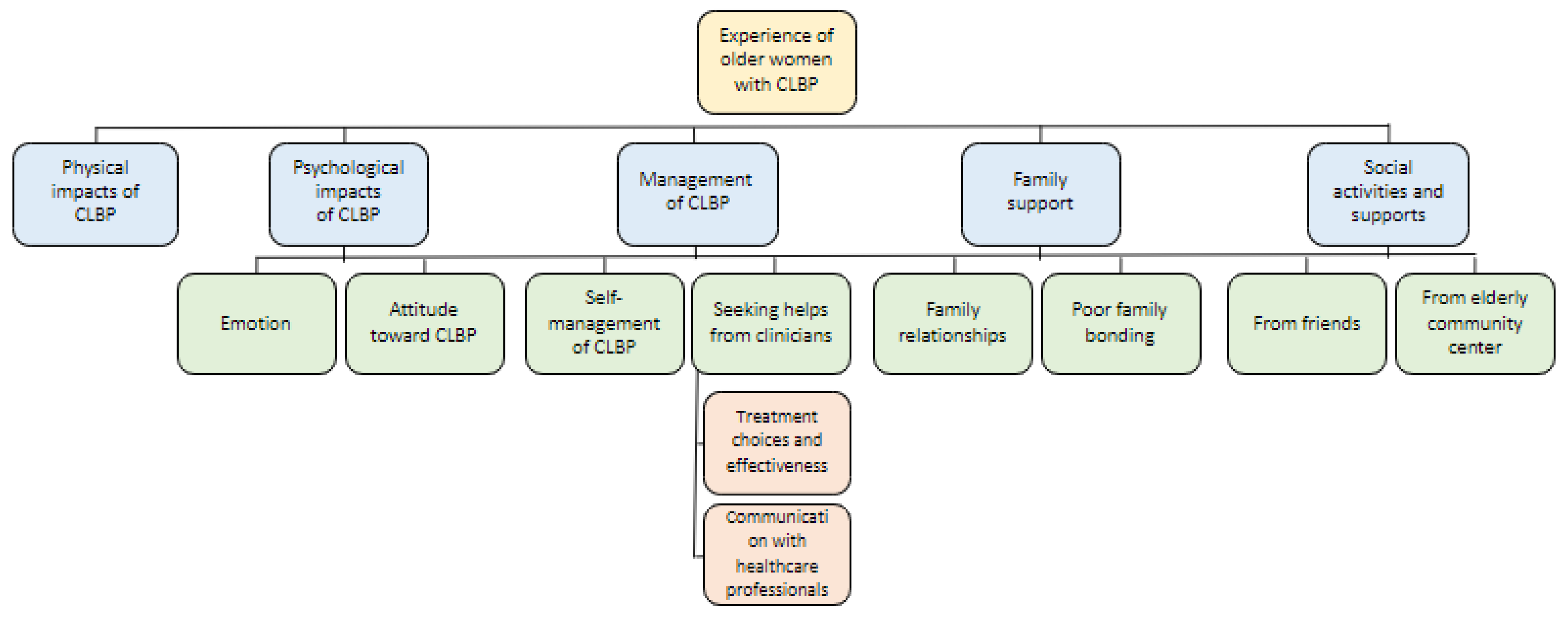
3. Results
3.1. Theme 1—Physical Impact on Daily Life
“I used to be fine because I did regular exercises, such as swimming… After I have LBP, I hate swimming and try to avoid it… my back was like hit by water from a waterfall. It was too painful for me to continue swimming.”(H5)
“When I sleep, my back will be in pain. …Sometimes I suffer from insomnia. …I can’t sleep at night, so I sleep in the morning. My days and nights are reversed…”(A4)
“I couldn’t sleep well, and my back was in pain.”(A6)
“I couldn’t sleep for two whole nights in a month. I feel painful when I have slept for a while, so I don’t want to sleep.”(H2)
3.2. Theme 2—Psychological Impacts of CLBP
3.2.1. Subtheme—Emotion
“I feel…sometimes desperate because of the incurable condition”(A6)
“It’s exhausting and lonely to suffer from the back pain.”(H3)
“I am worried that I may not be able to walk anymore.”(C2)
“I am not depressed now; it has been there for many years, and I have accepted it.”(A5)
3.2.2. Subtheme—Attitudes toward CLBP
“… I feel like this…injury will stay with me for the rest of my life.”(A3)
“I don’t want to increase their [referring to her family] burden. Besides, there’s nothing they can do to help me.”(C1)
“... They thought that it was something simple. … Nobody helped me, I did everything by myself.”(C3)
3.3. Theme 3—Management of CLBP
3.3.1. Subtheme—Self-Management of CLBP
“I may forget the pain after exercising. …I tend to do more exercise. … I keep on doing it as I hope my back won’t deteriorate quickly.”(A1)
“I have been doing exercise, but the pain has not been relieved.”(C3)
3.3.2. Subtheme—Seeking Help from Clinicians
Nested Subtheme—Treatment Choices and Effectiveness
“I have visited different doctors…but my back hasn’t got any better. …”(A2)
“Although I have visited a doctor, I didn’t receive any specific treatment. I only received some heat therapies, but they were useless.”(H2)
“… I hate taking medicine, but I tend to accept Chinese medicine instead of western medicine. I think Chinese medicine helps me regulate my body. … sometimes after I took the western medicine, my mouth would be dry and uncomfortable. …”(A5)
“I spent around HK$200 to HK$300 [approximately US$25 to US$38] to receive acupuncture each time. However, it’s not effective.”(H3)
“I received acupuncture from my son-in-law, I feel much relieved.”(A6)
“After receiving physiotherapy, I realized that there were some movements that I could do. These could be very useful. I think physiotherapy was quite effective… They [GPs] said, the number of times to receive physiotherapy was limited.”(A3)
Nested Subtheme—Communication with Healthcare Professionals
“… they [the medical doctors who met A3] were helpful. They taught me some movements and … explained how these movements would be useful to me.”(A3)
“My GP (…) gave me some painkillers and ointments. He didn’t give me enough time to talk. There was no examination either. (…) My Chinese medicine practitioner took my pulse. He would check if there were problems associated with ‘blood deficiency’ or old age. Then he prescribed Chinese medicine to regulate my body. (…) I don’t think the GP cared about me (…) I think the Chinese medicine practitioner is better.”(C1)
3.4. Theme 4—Family Relationships
3.4.1. Subtheme—Support from Family Members
“My children were worried and brought me to visit two to three doctors (…) My children treat me very well and they give me sufficient care (…) My children paid for the medical expenses (…) My children hired a part-time domestic helper. (…) My children arranged my treatment.”(H1)
“We [participant and her children] go to Chinese restaurants together when they have holidays.”(C4)
“They even gave me acupuncture. (…) They like to give me physiotherapy.”(A6)
3.4.2. Subtheme—Poor Family Bonding
“My children seldom visit me because they are busy. (…) I seldom discuss my things with others. I don’t want to increase their burden. Besides, there’s nothing they can do to help me. (…) It’s not necessary to talk about this.”(C1)
“They just reminded me to take a rest on my bed when I am in pain. They believed I should move less and only perform the movements when I feel good.”(A3)
“If I die in my bed, he [participant’s son] won’t even realize (…) One time I fell and felt dizzy. I went to the washroom to vomit. My son asked ‘Mum, what’s the matter?’ I said, ‘I’m exhausted, I hit my head and it’s painful, I’m also vomiting.’ My son replied, ‘Go to see a doctor!’, and then he left the washroom”(A4)
3.5. Theme 5—Social Activities and Support
3.5.1. Subtheme—Social Activities and Support from Friends
“Sometimes I will share my CLBP condition with the friends I met in the Chinese restaurant.”(A6)
“They [Participant A3’s friends] told me that some movements could be useful to me and encouraged me to try.”(A3)
“Sometimes I call my friends and chat with them when I feel lonely. (…) They care about me.”(H3)
“My friend also take care of me from time to time. My friend cooks meals for me.”(H5)
“I used to visit my relatives. Now I go out less and have fewer chances to go to Chinese restaurant with my friends.”(C1)
3.5.2. Subtheme—Elderly Community Centre (ECC)
“From time to time, there are exercise classes here. I may forget the pain after the exercise. Luckily, there are exercise classes here for me to improve my health. (…) I rely on such classes to do exercise. (…) This friend comes from the centre. (…) I feel better when I come here, it eases my mood. This place is good, it’s helpful for me.”(A1)
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Interview Guide
- Can you share me your low back pain experiences?
- What are your perceived cause(s) of your back pain? Why?
- Have any healthcare professionals or physicians told you the causes of your back pain? What did they say?
- How does your pain feel like?
- Did you see and do things differently after you have this pain?
- How does your typical day look like? Would it be different if your pain level changes in a particular day?
- What did you do to deal with your pain? Were your methods helpful? Are you still doing them? Why or why not?
- Were there any people or organizations provide help or advice to you on your blow back pain issue? Why or why not?
- How did they (people or organizations) help you? Do you find these helps useful? Why or why not?
- Are there any merits or dismerits of having low back pain?
- If your pain completely disappears, what would you like to do? Why?
- If your pain will stay with you forever? What do you think? Why?
- If you want to thank someone because of your low back pain, who would they be? Why?
- If you could do one or two things in exchange for a pain free experience, what would that/those be? Why?
- Do you think your chronic low back pain will be cured? Why or why not? Who told you that?
- 16.
- Apart from what we have discussed, anything you want to tell us?
Appendix B. Representative Quotes from Various Themes and Subthemes
- Representative Quotes for Theme 1—Physical Impacts of Chronic Low Back Pain (CLBP) in Daily Life
- 1.
- “I can’t climb up and bend my back while doing housework. I will call my husband for help when I need to climb up. I can’t do it myself because my back would hurt.”(A4)
- 2.
- “I rarely do housework because the longer I stand in the kitchen, the more pain I feel.”(A6)
- 3.
- “I couldn’t do housework because of LBP.”(C3)
- 4.
- “I can’t kneel down. I am afraid to climb up. Therefore, I can’t clean my windows. I can’t reach high objects, too.”(C4)
- 5.
- “When I am in pain I won’t clean the exhaust fan.”(H4)
- 6.
- “Whenever I sit for a while, I will be in pain…At present, I can’t sit for a long period of time. In the past, I used to sit for almost 1 h. Now I can’t do the same thing as I will feel exhausted and need to get up…I sit at here every day. Then, both my neck and back will be in pain. I am forced to get up.”(A1)
- 7.
- “I am not sitting for too long. …I can’t walk quickly. …”(A2)
- 8.
- “Whenever I leave the bed or sit down, I will feel painful…My shoulders and my back are in pain. I need to move a lot since I can’t sit for too long. After I sat down for a while, I would stand up and go to the kitchen to pour a cup of hot water. After I finished drinking, I would go back to the kitchen to wash my cup. Hence, I always walk around. I won’t sit for a few hours without moving.”(A5)
- 9.
- “I feel pain when I walk. Sometimes, when I sit for long, pain comes. The best posture is lying flat, no pain.”(A6)
- 10.
- “The pain is continuous when I am walking. … I feel painful when I walk.”(C2)
- 11.
- “I can’t stand straight. I have LBP whenever I stand. …I can’t even stand for 5 min after completing a task, I must sit afterwards…”(C3)
- 12.
- “I walked less. I feel tired when I have moved for a while.”(C4)
- 13.
- “… it was exhausting to walk. It’s not a common pain. I have to press on the wall to walk around at home…”(H2)
- 14.
- “I had difficulty in walking. I lay on my bed day and night.”(H3)
- 15.
- “Sometimes when I am tired after moving around, I will be in pain.”(H4)
- 16.
- “Even though I start sleeping at around 11 p.m. I still haven’t fall asleep at around 1 a.m. I sleep poorly now. Sometimes I can only sleep for around 3 to 4 h at night.”(C1)
- 17.
- “I feel tired when I have slept for a long time. Hence, I sleep for a while then get up to move for a while.”(C4)
- 18.
- “It was like a nightmare because I couldn’t sleep well.”(H5)
- 19.
- “I can’t carry heavy objects.”(A1)
- 20.
- “When I am carrying heavy items, I feel like I am falling.”(C2)
- 21.
- “I feel tired when I carry heavy objects. If I carry something heavy, I won’t be able to go upstairs with my legs…I usually use it (a trolley) when I am going to buy something heavy, such as fruits.”(C4)
- 22.
- “It hurts when I am carrying something heavy.”(H1)
- 23.
- “I couldn’t take the stairs.”(C3)
- 24.
- “… I didn’t have the strength to go up and down on stairs, along with difficulty in walking…”(A5)
- 25.
- “I feel uncomfortable when I sit or do exercise. I feel paralyzed.”(H3)
- Representative Quotes for Theme 2—Psychological Impacts of CLBP
- 1.
- “I am not worried about it.”(C4)
- 2.
- “It’s useless to be afraid. I need to take care of myself anyways.”(H5)
- 3.
- “I only worry about him (interviewee’s son), nothing else. I don’t worry about myself, but if I pass away, who will take care of him?”(A1)
- 4.
- “I am worried that it may become worse.”(A2)
- 5.
- “I worry that I will become immobile...”(A6)
- 6.
- “Of course it did. (feeling worried and afraid) Sometimes I pay attention when I walk. It will be terrible if I fall again. I still need to take care of my old husband.”(C1)
- 7.
- “I am afraid I may not be able to walk. It will be miserable to sit on wheelchair.”(C3)
- 8.
- “I am worried, because many people said it can’t be cured. It’s hard to cure it at my age.”(H3)
- 9.
- “Yes (worried she may become a burden of her family), so I need to take good care of myself.”(H4)
- 10.
- “I sometimes feel desperate because of the incurable condition ….I feel bored, very bored. I am an out-going person who loves to go outside, but I can bear for a short walk nowadays, so I…very annoyed, feeling frustrated, and helpless at this moment.”(A6)
- 11.
- “When my treatment is not good enough, I will feel frustrated. When there is suitable treatment, I will be happier.”(H1)
- 12.
- “I am unhappy because I have done less housework.”(C3)
- 13.
- “It’s impossible for my back to fully recover. The LBP may stay with me for my entire life.”(A1)
- 14.
- “I think it (the pain) will stay with me forever.”(A5)
- 15.
- “As I get older, it will also get worse. This disease will not recover.”(C1)
- 16.
- “I don’t want to make anyone in trouble.”(A4)
- 17.
- “They are very busy working; I don’t want to bother them (the interviewee’s family member.”(A6)
- 18.
- “I don’t want them to worry about me. Even if I tell them, they won’t be able to help me.”(C2)
- Representative Quotes for Theme 3—Self-Management of CLBP
- 1.
- “I realize the most important thing is doing exercises. …I have done the exercises at home.”(A5)
- 2.
- “Occasionally there are some stretching exercises at the centre, I will join them. …Sometimes I perform exercises that are suitable for me. I will follow my tablet’s recommendations. …I also do exercises at home every day.”(C1)
- 3.
- “It’s important to do exercise.”(H5)
- 4.
- “…when the pain occurred I would be fine if I put some band-aid and medicated oil on the spot.”(A1)
- 5.
- “Those band-aids, I bought…many people said they are great. I purchased a lot and my home is full of them.”(A2)
- 6.
- “… I also use some band-aid to relieve the pain.”(C3)
- 7.
- “Sometimes I need to apply the medicated oil.”(C1)
- 8.
- “Sometimes I will apply some medicated oil on it. It will be better at that moment, but the pain will occur again next morning.”(H3)
- 9.
- “Sometimes I boil Chinese herbal medicine. Other people, such as the Chinese medicine practitioner, recommended me to boil these. They said these are good for my back and leg. …I felt better after consuming them.”(A1)
- 10.
- “It will be great to consume some Chinese medicine.”(C4)
- 11.
- “Consuming the painkillers could stop the pain at the beginning, but when I consumed too much, my face will be numb”(A4)
- 12.
- “When the pain is weak, I only put on ointment to soothe the pain.”(A4)
- 13.
- “…I also sleep and apply ointment.”(C1)
- 14.
- “…when I am really in pain, I will find someone to massage me…”(A5)
- 15.
- “…I also need to massage myself…”(C1)
- 16.
- “In the past I have received massage in mainland. I felt better after the massage. I used to receive a lot of massage. …The massage is effective.”(C4)
- Representative Quotes for Theme 4—Seeking Help from Clinicians
- 1.
- “The general practitioners only gave me western medicine and painkillers.”(A1)
- 2.
- “I visited the private doctors.”(C3)
- 3.
- “I want to visit the Chinese medicine practitioner. I want to find out whether Chinese medicine can regulate my body.”(A1)
- 4.
- “I always visit the Chinese medicine practitioner. …According to the situation of my LBP, the Chinese medicine practitioner will provide Chinese medicine for me to regulate my body. …The Chinese medicine practitioner will take my pulse. He will check if there are problems because of blood deficiency or old age. Then he will provide some Chinese medicine for me to regulate my body.”(C1)
- 5.
- “The physiotherapists also taught me some exercises to do at home. These are helpful.”(A4)
- 6.
- “I feel better after consuming medicine and receiving physiotherapy.”(H1)
- 7.
- “The physical therapist provided acupuncture for me. Once I received the acupuncture, I felt relaxing”(A5)
- 8.
- “I have begun receiving acupuncture. It will get better gradually.”(H2)
- 9.
- “I visited the orthopedics because I felt a little bit of pain.”(H2)
- 10.
- “I visited the orthopedics in Hong Kong Adventist Hospital.”(H5)
- 11.
- “I tried bone setter once. The practitioner said my bone was crooked…that was pretty much it. Nevertheless, the treatment was painful. He pressed and twisted my body. It was very painful.”(A1)
- 12.
- “I am visiting bone setter now but some people say a certain place provides good acupuncture. I want to try it but I also don’t want to give up on my current bone setting treatment. I think my current treatment is quite useful.”(C3)
- 13.
- “The chiropractor is useful, but I don’t know how long will the treatments last. Besides, it is very expensive.”(H2)
- 14.
- “The chiropractor said he specializes in curing this kind of disease. I also called my son to let him know I will be receiving treatment from the chiropractor. The chiropractor said I need to receive treatment for at least 10 times. Each time cost around 700 HKD. I said I could try 10 times of treatment, the chiropractor told me I should receive 30 times of treatment. Hence, I made a one-time payment and received 30 times of treatment.”(H5)
- 15.
- “The Tui Na or bone setter kept on pressing my affected area, but he didn’t put medicine on it.”(H2)
- 16.
- “Later I visited the acupuncture and Tui Na.”(H3)
- 17.
- “Doctors were nice, they chatted with me.”(H2)
- 18.
- “I chatted with him (bonesetter) about my painful area and how’s the pain. … The private doctors are great as well. The one I often visit also chat with me.”(C3)
- 19.
- “If I visit doctors, they will only give me painkillers. I don’t think that’s effective.”(C2)
- 20.
- “The general practitioners didn’t tell me anything. They just gave me painkillers. If I feel excruciating pain, they will give me an injection.”(C3)
- 21.
- (Did you gain some encouragement from the Chinese medicine practitioner?) “I think that was nice. It felt like someone cared about me.“
- Representative Quotes for Theme 5—Support from Family Members
- 1.
- “My son bought some band-aid from Japan. … I couldn’t do housework because of LBP. I asked my husband to help me do it.”(C3)
- 2.
- “My children paid for it (medical expense).”(H1)
- 3.
- “After 2017, my daughter arranged a domestic helper to deliver meals for me at home. She had to go oversea because of work.”(H3)
- 4.
- “My sons also give me money from time to time.”(H4)
- 5.
- “I usually ask my son to help me do heavy manual labor.”(H5)
- 6.
- “…they just reminded me to take a rest on my bed when I am in pain. They believed I should move less and only perform the movements when I feel good.”(A3)
- 7.
- “…They only ask me to visit doctors.”(A4)
- 8.
- “All four of them (4 daughters of the interviewee) know I have back fatigue. They told me to avoid kneeling and climbing.”(C4)
- 9.
- “My son told me to visit a doctor, but not a western doctor. …My son told me to visit a chiropractor, but it is expensive.”(H2)
- 10.
- “I play mahjong with my children.”(A6)
- 11.
- “He (interviewee’s son) visits me when he got off work…”(H5)
- 12.
- “They (the interviewee’s sons) treat me very well and take good care of me. …my children treat me very well and they give me sufficient care.”(H1)
- Representative Quotes for Theme 6—Social Activities and Support
- 1.
- “… they (interviewee’s friends) would ask me whether it hurt or not. They would also remind me to be careful. … There were many neighbors. I went to Chinese restaurant with them.”(A2)
- 2.
- “… they (interviewee’s friends) gave me some opinion. They told me some movements could be useful and suggested me to try.”(A3)
- 3.
- “I chat with my friends through social media (WhatsApp) groups.”(A4)
- 4.
- “I try to manage my time efficiently, now I usually participate in church activities. … A doctor who went to the same church as mine had helped me through massage. Many people provided care for me.”(A5)
- 5.
- “I am not sure whether I have received physiotherapy, but the neighbors supported my decision to visit the doctor.”(H4)
- 6.
- “Now I can’t travel, such as those trips to mainland. …I am worried that I may hinder others. If I have trouble going up and down, I may get in the way of others. Thus, I shouldn’t join them.”(A2)
- 7.
- “Because of LBP I went out less, plus the pandemic. …I don’t go out much. When I’m in pain I may not go out.”(A4)
- 8.
- “… it makes me feel bored. I used to go shopping a lot, but now I always stay long at home.”(A6)
- 9.
- “I may participate more (go hiking and have dim sum in Chinese restaurant with friends) without the LBP.”(C2)
- 10.
- “I go out less due to LBP. In the past I went out every day.”(H3)
- 11.
- “Now I sign up for some activity classes (in the elderly center). I hope these can be useful for my LBP.”(A3)
- 12.
- “I will join things that may improve my body. Sometimes there are Chinese medicine practitioners who come here to talk about Chinese medicine and acupuncture points. I like to join these. …The center usually invites people to come and provide lectures for us…We have a monthly magazine. I sign up for everything which can be beneficial to my health.”(C1)
- 13.
- “…Sometimes there are lectures about acupressure, I will join these.”(C2)
- 14.
- “At present I have joined the volunteer. Although I can’t carry heavy items, I can participate in activities that only need to use my hands, as well as those that can be carried out when I am sitting.”(C3)
- 15.
- “There are two cycling machines and some treadmills here. I do as many exercises as I can, but I won’t force myself. …I need to make an appointment to do exercise at the center. The staff also taught us to do exercise.”(H3)
- 16.
- “Then, I go to the center and Po Leung Kuk to practice” Tai Chi”. They hired some young people. I took some photos with them. …Po Leung Kuk has many activities. … It’s great that their staff play with us. They really care about us. …they (staff in elder center) taught me how to use these (application for video call).” (H4)
References
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 2015, 49, 73. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P. Diagnosis and classification of chronic low back pain disorders: Maladaptive movement and motor control impairments as underlying mechanism. Man. Ther. 2005, 10, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, A.; Abate, M.; Guralnik, J.M.; Bandinelli, S.; Cecchi, F.; Cherubini, A.; Corsonello, A.; Foschini, N.; Guglielmi, M.; Lauretani, F. From chronic low back pain to disability, a multifactorial mediated pathway: The InCHIANTI study. Spine 2007, 32, E809. [Google Scholar] [CrossRef]
- Rudy, T.E.; Weiner, D.K.; Lieber, S.J.; Slaboda, J.; Boston, R.J. The impact of chronic low back pain on older adults: A comparative study of patients and controls. Pain 2007, 131, 293–301. [Google Scholar] [CrossRef]
- Cole, L.J.; Farrell, M.J.; Gibson, S.J.; Egan, G.F. Age-related differences in pain sensitivity and regional brain activity evoked by noxious pressure. Neurobiol. Aging 2010, 31, 494–503. [Google Scholar] [CrossRef]
- Edwards, R.R.; Fillingim, R.; Ness, T. Age-related differences in endogenous pain modulation: A comparison of diffuse noxious inhibitory controls in healthy older and younger adults. Pain 2003, 101, 155–165. [Google Scholar] [CrossRef]
- Lautenbacher, S.; Kunz, M.; Strate, P.; Nielsen, J.; Arendt-Nielsen, L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain 2005, 115, 410–418. [Google Scholar] [CrossRef]
- De Souza, I.M.B.; Sakaguchi, T.F.; Yuan, S.L.K.; Matsutani, L.A.; Espírito-Santo, A.D.S.D.; Pereira, C.A.D.B.; Marques, A.P. Prevalence of low back pain in the elderly population: A systematic review. Clinics 2019, 74, e789. [Google Scholar]
- Wong, W.S.; Fielding, R. Prevalence and Characteristics of Chronic Pain in the General Population of Hong Kong. J. Pain 2011, 12, 236–245. [Google Scholar] [CrossRef] [Green Version]
- Weiner, D.K.; Haggerty, C.L.; Kritchevsky, S.B.; Harris, T.; Simonsick, E.M.; Nevitt, M.; Newman, A. How Does Low Back Pain Impact Physical Function in Independent, Well-Functioning Older Adults? Evidence from the Health ABC Cohort and Implications for the Future. Pain Med. 2003, 4, 311–320. [Google Scholar] [CrossRef] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Fisker, A.; Petersen, T.; Langberg, H.; Mortensen, O.S. The association between psychosocial distress, pain and disability in patients with persistent low back pain—A cross-sectional study. Cogent Med. 2018, 5, 1534536. [Google Scholar] [CrossRef]
- El Dib, O.E.; El Azeem, S.A.; Awadh, M.S.; Rizk, M. Chronic low back pain & psychological comorbidity. Int. J. Dev. Res. 2019, 9, 25072–25076. [Google Scholar]
- Makris, U.E.; Melhado, T.V.; Lee, S.C.; Hamann, H.A.; Walke, L.M.; Gill, T.M.; Fraenkel, L. Illness Representations of Restricting Back Pain: The Older Person’s Perspective. Pain Med. 2014, 15, 938–946. [Google Scholar] [CrossRef] [Green Version]
- Tong, Y.; Jun, M.; Jiang, Y.; Jian, L.; Gen, Y.; Yufeng, W.; Wenjie, S. Assessing pain among Chinese elderly-chinese health and retirement longitudinal study. Iran. J. Public Health 2018, 47, 553. [Google Scholar]
- Liu, X.-K.; Xiao, S.-Y.; Zhou, L.; Hu, M.; Liu, H.-M. Different predictors of pain severity across age and gender of a Chinese rural population: A cross-sectional survey. BMJ Open 2018, 8, e020938. [Google Scholar] [CrossRef] [Green Version]
- Cho, N.H.; Jung, Y.O.; Lim, S.H.; Chung, C.-K.; Kim, H.A. The Prevalence and Risk Factors of Low Back Pain in Rural Community Residents of Korea. Spine 2012, 37, 2001–2010. [Google Scholar] [CrossRef]
- Wong, C.K.; Mak, R.Y.; Kwok, T.S.; Tsang, J.S.; Leung, M.Y.; Funabashi, M.; Macedo, L.G.; Dennett, L.; Wong, A.Y. Prevalence, Incidence, and Factors Associated with Non-Specific Chronic Low Back Pain in Community-Dwelling Older Adults Aged 60 Years and Older: A Systematic Review and Meta-Analysis. J. Pain 2021, 23, 509–534. [Google Scholar] [CrossRef]
- Wong, A.Y.L.; Forss, K.S.; Jakobsson, J.; Schoeb, V.; Kumlien, C.; Borglin, G. Older adult’s experience of chronic low back pain and its implications on their daily life: Study protocol of a systematic review of qualitative research. Syst. Rev. 2018, 7, 81. [Google Scholar] [CrossRef]
- De Souza, L.H.; Frank, A.O. Experiences of living with chronic back pain: The physical disabilities. Disabil. Rehabil. 2007, 29, 587–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailly, F.; Foltz, V.; Rozenberg, S.; Fautrel, B.; Gossec, L. The impact of chronic low back pain is partly related to loss of social role: A qualitative study. Jt. Bone Spine 2015, 82, 437–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lansbury, G. Chronic pain management: A qualitative study of elderly people’s preferred coping strategies and barriers to management. Disabil. Rehabil. 2000, 22, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Makris, U.E.; Higashi, R.T.; Marks, E.G.; Fraenkel, L.; Gill, T.M.; Friedly, J.L.; Reid, M.C. Physical, Emotional, and Social Impacts of Restricting Back Pain in Older Adults: A Qualitative Study. Pain Med. 2016, 18, 1225–1235. [Google Scholar] [CrossRef] [Green Version]
- Igwesi-Chidobe, C.N.; Kitchen, S.; Sorinola, I.O.; Godfrey, E.L. “A life of living death”: The experiences of people living with chronic low back pain in rural Nigeria. Disabil. Rehabil. 2017, 39, 779–790. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.Y.; Samartzis, D. Low back pain in older adults—The need for specific outcome and psychometric tools. J. Pain Res. 2016, 9, 989–991. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Iecovich, E.; Carmel, S. Differences between Users and Nonusers of Day Care Centers among Frail Older Persons in Israel. J. Appl. Gerontol. 2010, 30, 443–462. [Google Scholar] [CrossRef]
- Baranwal, A.; Mishra, S. Understanding the importance of day care centres for elderly in Mumbai. Asian J. Res. Soc. Sci. Humanit. 2021, 11, 15–22. [Google Scholar] [CrossRef]
- Buchbinder, R.; Underwood, M.; Hartvigsen, J.; Maher, C.G. The Lancet Series call to action to reduce low value care for low back pain: An update. Pain 2020, 161, S57–S64. [Google Scholar] [CrossRef]
- Chang, J.R.; Fu, S.-N.; Li, X.; Li, S.X.; Wang, X.; Zhou, Z.; Pinto, S.M.; Samartzis, D.; Karppinen, J.; Wong, A.Y. The differential effects of sleep deprivation on pain perception in individuals with or without chronic pain: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 66, 101695. [Google Scholar] [CrossRef]
- Schrimpf, M.; Liegl, G.; Boeckle, M.; Leitner, A.; Geisler, P.; Pieh, C. The effect of sleep deprivation on pain perception in healthy subjects: A meta-analysis. Sleep Med. 2015, 16, 1313–1320. [Google Scholar] [CrossRef]
- Chang, J.R.; Wang, X.; Lin, G.; Samartzis, D.; Pinto, S.M.; Wong, A.Y. Are changes in sleep quality/quantity or baseline sleep parameters related to changes in clinical outcomes in patients with nonspecific chronic low back pain? A systematic review. Clin. J. Pain 2022, 38, 292–307. [Google Scholar] [CrossRef]
- Hester, J.; Tang, N.K.Y. Insomnia Co-Occurring with Chronic Pain: Clinical Features, Interaction, Assessments and Possible Interventions. Rev. Pain 2008, 2, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Sun, J.M.; Yoon, K.B.; Moon, J.H.; An, J.R.; Yoon, D.M. Risk Factors Associated with Clinical Insomnia in Chronic Low Back Pain: A Retrospective Analysis in a University Hospital in Korea. Korean J. Pain 2015, 28, 137–143. [Google Scholar] [CrossRef]
- Ronai, P.; Sorace, P. Chronic Nonspecific Low Back Pain and Exercise. Strength Cond. J. 2013, 35, 29–32. [Google Scholar] [CrossRef]
- Serrano-Ibáñez, E.R.; Bendayan, R.; Ramírez-Maestre, C.; López-Martínez, A.E.; Ruíz-Párraga, G.T.; Peters, M.; Esteve, R. Exploring Changes in Activity Patterns in Individuals with Chronic Pain. Int. J. Environ. Res. Public Health 2020, 17, 3560. [Google Scholar] [CrossRef]
- Aldrich, S.; Eccleston, C.; Crombez, G. Worrying about chronic pain: Vigilance to threat and misdirected problem solving. Behav. Res. Ther. 2000, 38, 457–470. [Google Scholar] [CrossRef]
- Rodrigues-de-Souza, D.P.; Palacios-Cena, D.; Moro-Gutierrez, L.; Camargo, P.R.; Salvini, T.F.; Alburquerque-Sendin, F. Socio-cultural factors and experience of chronic low back pain: A Spanish and Brazilian patients’ perspective. A qualitative study. PLoS ONE 2016, 11, e0159554. [Google Scholar] [CrossRef] [Green Version]
- Larsen, E.L.; Nielsen, C.V.; Jensen, C. Getting the pain right: How low back pain patients manage and express their pain experiences. Disabil. Rehabil. 2012, 35, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Allcock, N. Pain in Older People: Reflections and Experiences from an Older Person’s Perspective. 2008. Available online: http://www.britishpainsociety.org/book_pain_in_older_age_ID7826.pdf (accessed on 22 February 2023).
- Wong, A.Y.; Lauridsen, H.H.; Samartzis, D.; Macedo, L.; Ferreira, P.H.; Ferreira, M.L. Global Consensus From Clinicians Regarding Low Back Pain Outcome Indicators for Older Adults: Pairwise Wiki Survey Using Crowdsourcing. JMIR Rehabil. Assist. Technol. 2019, 6, e11127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devraj, R.; Herndon, C.M.; Griffin, J. Pain Awareness and Medication Knowledge: A Health Literacy Evaluation. J. Pain Palliat. Care Pharmacother. 2013, 27, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Schoeb, V. Healthcare Service in Hong Kong and its Challenges. China Perspect. 2016, 2016, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Steiger, F.; Wirth, B.; De Bruin, E.D.; Mannion, A.F. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur. Spine J. 2011, 21, 575–598. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.M.; Boghra, S.B.; Macedo, L.G.; Zheng, Y.-P.; Pang, M.Y.; Cheung, J.P.; Karppinen, J.; Samartzis, D.; Wong, A.Y. Does Motor Control Exercise Restore Normal Morphology of Lumbar Multifidus Muscle in People with Low Back Pain?—A Systematic Review. J. Pain Res. 2021, 14, 2543–2562. [Google Scholar] [CrossRef]
- Taheri, M.; Mohammadi, M.; Paknia, B.; Mohammadbeigi, A. Elderly awareness on healthy lifestyle during aging. Trop. Med. Surg. 2013, 1, 5. [Google Scholar]
- Elderly Commission. Report on Healthy Ageing Executive Summary. Available online: https://www.elderlycommission.gov.hk/en/library/Ex-sum.htm#3 (accessed on 22 February 2023).
- Kovacs, F.M.; Burgos-Alonso, N.; Martín-Nogueras, A.M.; Seco-Calvo, J. The Efficacy and Effectiveness of Education for Preventing and Treating Non-Specific Low Back Pain in the Hispanic Cultural Setting: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 825. [Google Scholar] [CrossRef]
- Ha, J.F.; Longnecker, N. Doctor-Patient Communication: A Review. Ochsner J. 2010, 10, 38–43. [Google Scholar]
- Lam, A.K.; Fung, O.H.; Kwan, C.; Cheung, J.P.; Luk, K.D.; Chiu, A.Y.; Descarreaux, M.; Szeto, G.P.; Wong, A.Y. The Concerns and Experiences of Patients With Lumbar Spinal Stenosis Regarding Prehabilitation and Recovery After Spine Surgery: A Qualitative Study. Arch. Rehabil. Res. Clin. Transl. 2022, 4, 100227. [Google Scholar] [CrossRef]
- Burns, J.; A Mullen, T. The Role of Traditional Chinese Medicine in the Management of Chronic Pain: A Biopsychosocial Approach. J. Patient-Cent. Res. Rev. 2015, 2, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Project Conern Hong Kong. What is “Four Diagnosis Methods”? Project Conern Hong Kong. Available online: http://www.projectconcern.org.hk/en/node/358 (accessed on 22 February 2023).
- Fu, Y.; McNichol, E.; Marczewski, K.; Closs, S.J. Exploring the Influence of Patient-Professional Partnerships on the Self-Management of Chronic Back Pain: A Qualitative Study. Pain Manag. Nurs. 2016, 17, 339–349. [Google Scholar] [CrossRef]
- Demoulin, C.; Gabriel, L.; de Mévergnies, O.N.; Henket, L.; Roussel, N.; Goubert, L.; Vanderthommen, M.; Pitance, L. Several low back pain-related misbeliefs are still around in 2020: A cross-sectional survey in Belgium. Physiother. Res. Int. 2022, 27, e1927. [Google Scholar] [CrossRef]
- Briggs, A.M.; Jordan, J.E.; Buchbinder, R.; Burnett, A.F.; O’Sullivan, P.B.; Chua, J.Y.; Osborne, R.H.; Straker, L.M. Health literacy and beliefs among a community cohort with and without chronic low back pain. Pain 2010, 150, 275–283. [Google Scholar] [CrossRef]
- Liu, F.; Tong, M. The Situated Influence of Chronic Pain Perception on Chinese Older Adults’ Self-Management in Home Care. Geriatrics 2018, 3, 64. [Google Scholar] [CrossRef] [Green Version]
- O’Hagan, E.T.; Di Pietro, F.; Traeger, A.C.; Cashin, A.G.; Hodges, P.W.; Wand, B.M.; O’Neill, S.; Schabrun, S.M.; Harris, I.A.; McAuley, J.H. What messages predict intention to self-manage low back pain? A study of attitudes towards patient education. Pain 2021, 163, 1489–1496. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310. [Google Scholar] [CrossRef]
- Kim, H.S.; Sherman, D.K.; Taylor, S.E. Culture and social support. Am. Psychol. 2008, 63, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Badanta, B.; González-Cano-Caballero, M.; Suárez-Reina, P.; Lucchetti, G.; de Diego-Cordero, R. How Does Confucianism Influence Health Behaviors, Health Outcomes and Medical Decisions? A Scoping Review. J. Relig. Health 2022, 61, 2679–2725. [Google Scholar] [CrossRef]
- Thomas, P.A. Is it better to give or to receive? Social support and the well-being of older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2010, 65, 351–357. [Google Scholar] [CrossRef]
- Haas, M.; Groupp, E.; Muench, J.; Kraemer, D.; Brummel-Smith, K.; Sharma, R.; Ganger, B.; Attwood, M.; Fairweather, A. Chronic Disease Self-Management Program for Low Back Pain in the Elderly. J. Manip. Physiol. Ther. 2005, 28, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Von Korff, M.; Moore, J.E.; Lorig, K.; Cherkin, D.C.; Saunders, K.; González, V.M.; Laurent, D.; Rutter, C.; Comite, F. A randomized trial of a lay person-led self-management group intervention for back pain patients in primary care. Spine 1998, 23, 2608–2615. [Google Scholar] [CrossRef] [PubMed]
- Stenner, P.; Cross, V.; McCrum, C.; McGowan, J.; Defever, E.; Lloyd, P.; Poole, R.; Moore, A.P. Self-management of chronic low back pain: Four viewpoints from patients and healthcare providers. Health Psychol. Open 2015, 2, 2055102915615337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowe, M.; Whitehead, L.; Gagan, M.J.; Baxter, D.; Panckhurst, A. Self-management and chronic low back pain: A qualitative study. J. Adv. Nurs. 2010, 66, 1478–1486. [Google Scholar] [CrossRef]
- Lorig, K.R.; Sobel, D.S.; Stewart, A.L.; Brown Jr, B.W.; Bandura, A.; Ritter, P.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med. Care 1999, 37, 5–14. [Google Scholar] [CrossRef]
- Kongsted, A.; Ris, I.; Kjaer, P.; Hartvigsen, J. Self-management at the core of back pain care: 10 key points for clinicians. Braz. J. Phys. Ther. 2021, 25, 396–406. [Google Scholar] [CrossRef]
- Neville, S.; Adams, J.; Montayre, J.; Larmer, P.; Garrett, N.; Stephens, C.; Alpass, F. Loneliness in Men 60 Years and Over: The Association With Purpose in Life. Am. J. Men Health 2018, 12, 730–739. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Number of Participants | Percentage | |
|---|---|---|
| Age (years) | ||
| 60–70 | 2 | 13.3 |
| 71–80 | 7 | 46.7 |
| 80–90 | 6 | 40 |
| Education | ||
| Primary school or below | 8 | 53.3 |
| Secondary school | 6 | 40 |
| University | 1 | 6.7 |
| Marital status | ||
| Single | 1 | 6.7 |
| Married | 8 | 53.5 |
| Widow | 6 | 40 |
| Household members (living condition) | ||
| With spouse | 5 | 33.3 |
| With children | 2 | 13.3 |
| With spouse and children | 2 | 13.3 |
| With relatives | 1 | 6.7 |
| With domestic helper | 1 | 6.7 |
| Alone | 4 | 26.7 |
| Types of housing | ||
| Public housing apartment | 13 | 86.7 |
| Self-own apartment | 2 | 13.3 |
| History of pain (years) | ||
| 1–10 | 6 | 40 |
| 11–19 | 5 | 33.3 |
| >20 | 4 | 26.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, T.H.T.; Lee, K.S.K.; Lo, S.M.C.; Kan, M.M.P.; Kwan, C.; Opsommer, E.; Anwer, S.; Li, H.; Wong, A.Y.L.; Schoeb, V. Challenges, Concerns, and Experiences of Community-Dwelling Older Women with Chronic Low Back Pain—A Qualitative Study in Hong Kong, China. Healthcare 2023, 11, 945. https://doi.org/10.3390/healthcare11070945
Wong THT, Lee KSK, Lo SMC, Kan MMP, Kwan C, Opsommer E, Anwer S, Li H, Wong AYL, Schoeb V. Challenges, Concerns, and Experiences of Community-Dwelling Older Women with Chronic Low Back Pain—A Qualitative Study in Hong Kong, China. Healthcare. 2023; 11(7):945. https://doi.org/10.3390/healthcare11070945
Chicago/Turabian StyleWong, Tiffany H. T., Kaden S. K. Lee, Sharon M. C. Lo, Mandy M. P. Kan, Crystal Kwan, Emmanuelle Opsommer, Shahnawaz Anwer, Heng Li, Arnold Y. L. Wong, and Veronika Schoeb. 2023. "Challenges, Concerns, and Experiences of Community-Dwelling Older Women with Chronic Low Back Pain—A Qualitative Study in Hong Kong, China" Healthcare 11, no. 7: 945. https://doi.org/10.3390/healthcare11070945