
Determining the Role of Employee Engagement in Nurse Retention along with the Mediation of Organizational Culture
Abstract
:1. Introduction
2. Theoretical Framework and Research Hypothesis
2.1. Theoretical Underpinning
2.2. Employee Engagement
2.3. Organizational Culture
2.4. Retention
2.5. Research Hypothesis
2.5.1. Employee Engagement and Retention
Employee Engagement and Organizational Culture
Organizational Culture and Retention
Organizational Culture as Mediator between Employee Engagement and Nurse Retention
3. Research Methodology
3.1. Design and Sample
3.2. Ethical Consent
3.3. Data Analysis/Measures
4. Results
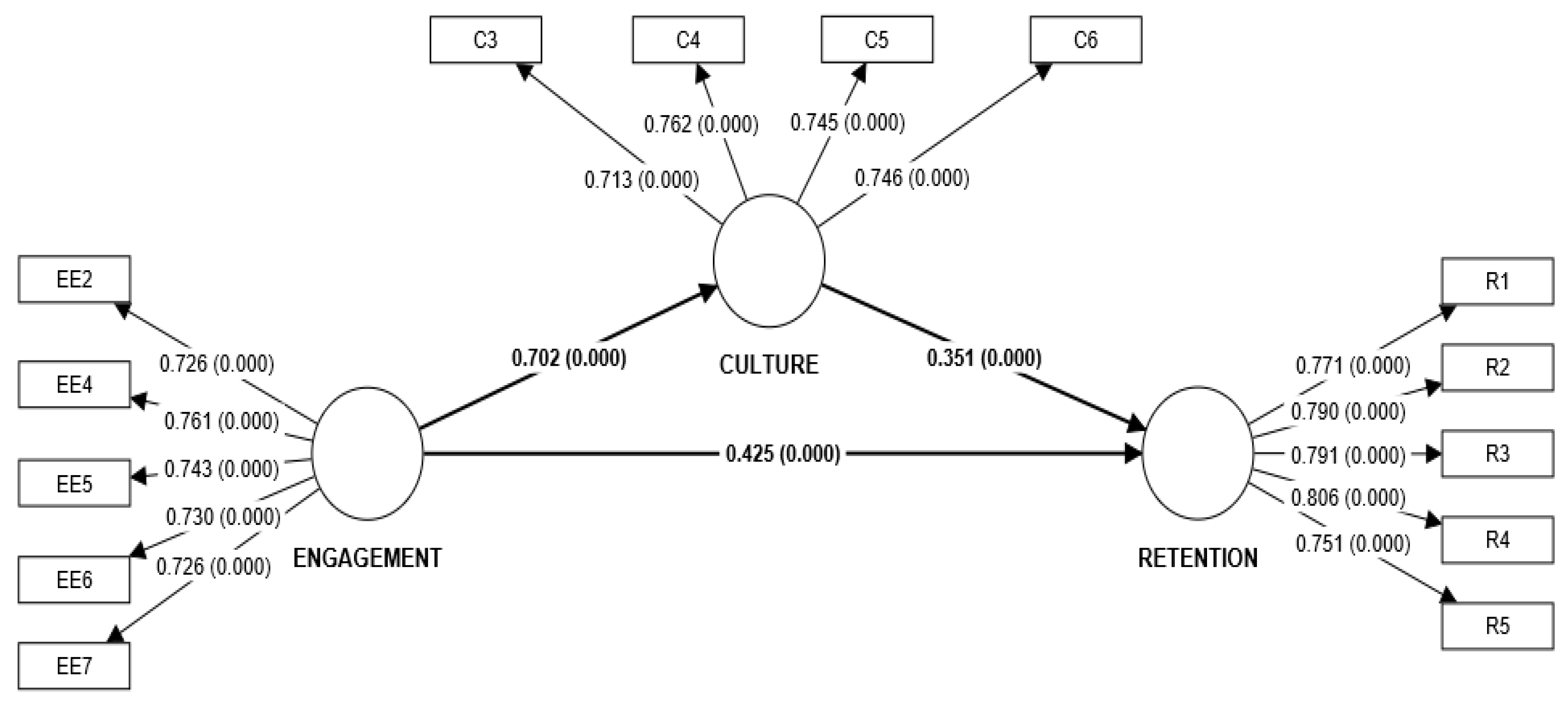
4.1. Measurement/Outer Model
4.2. Structural/Inner Model
4.3. Mediation Analysis
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Construct of the Study | Item |
| EE | EE1 I understand the vision of the hospital. |
| EE2 I feel strong & vigorous at my job. | |
| EE3 I feel enthusiastic about the challenges at work. | |
| EE4 Hospital conducts engaging activities (for example: games, role play etc.) at regular basis | |
| EE5 I am satisfied with engaging activities conducted | |
| EE6 I collaborate with my co-workers to achieve work goals. | |
| EE7 My team is my inspiration at work | |
| OC | OC |
| OC1 I can always talk with someone at work if I have work related problem | |
| OC2 My Seniors treat me with respect. | |
| OC3 Hospital provides flexible work arrangements. | |
| OC4 Hospital adapts change quickly. | |
| OC5 My supervisor recognizes and rewards my effort. | |
| OC6 My Relationship with colleagues is friendly as well as professional. | |
| Retention | RTN |
| R1 I see my future in this hospital | |
| R2 I do not intend to leave the hospital in near future | |
| R3 Presently, I am not searching for job in another hospital | |
| R4 It is unlikely that I will look for a job in near future | |
| R5 I will continue to work in this hospital despite of being offered by other hospital |
References
- Gebregziabher, D.; Berhanie, E.; Berihu, H.; Belstie, A.; Teklay, G. The relationship between job satisfaction and turnover intention among nurses in Axum comprehensive and specialized hospital Tigray, Ethiopia. BMC Nurs. 2020, 19, 79. [Google Scholar] [CrossRef] [PubMed]
- Nayak, T.; Sahoo, C.K.; Mohanty, P.K.; Sundaray, B.K. HR interventions and quality of work life of healthcare employees: An investigation. Ind. Commer. Train. 2016, 48, 234–240. [Google Scholar] [CrossRef]
- Perry, S.J.; Richter, J.P.; Beauvais, B. The effects of nursing satisfaction and turnover cognitions on patient attitudes and outcomes: A three-level multisource study. Health Serv. Res. 2018, 53, 4943–4969. [Google Scholar] [CrossRef] [PubMed]
- Ray, P. Nursing in Kolkata: Everyday Politics of Labour, Power and Subjectivities. South Asia Res. 2020, 40, 40–57. [Google Scholar] [CrossRef]
- Falatah, R. The Impact of the Coronavirus Disease (COVID-19) Pandemic on Nurses’ Turnover Intention: An Integrative Review. Nurs. Rep. 2021, 11, 787–810. [Google Scholar] [CrossRef]
- Nei, D.; Snyder, L.A.; Litwiller, B.J. Promoting retention of nurses: A meta-analytic examination of causes of nurse turnover. Health Care Manag. Rev. 2015, 40, 237–253. [Google Scholar] [CrossRef]
- Dracup, K.; Bryan-Brown, C.W. From novice to expert to mentor: Shaping the future. Am. J. Crit. Care 2004, 13, 448–450. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, P.; Maruotti, A.; Saucedo, A.R.; Redfern, O.C.; Ball, J.E.; Briggs, J.; Dall’Ora, C.; Schmidt, P.E.; Smith, G.B. Nurse staffing, nursing assistants and hospital mortality: Retrospective longitudinal cohort study. BMJ Qual. Saf. 2019, 28, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Maiti, M.; Das, D. A descriptive study on Non-Communicable Disease among nursing personals in a Medical Teaching Institute, Kolkata. Int. J. Health Clin. Res. 2022, 5, 95–100. [Google Scholar]
- Bae, S.H.; Mark, B.; Fried, B. Impact of nursing unit turnover on patient outcomes in hospitals. J. Nurs. Scholarsh. 2010, 42, 40–49. [Google Scholar] [CrossRef]
- Ismail, M.; Angham, A.M.; Abed, A.; DN, S. Impact of nursing staff perception of work environment on turnover rate in hemodialysis unit. Med. J. Cairo Univ. 2020, 88, 85–90. [Google Scholar]
- Moloney, W.; Boxall, P.; Parsons, M.; Cheung, G. Factors predicting registered nurses’ intentions to leave their organisation and profession? A job demands-resources framework. J. Adv. Nurs. 2018, 74, 864–875. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.C. Improving Healthcare Worker Retention through Decreasing Burnout and Increasing Employee Engagement. Ph.D. Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2022. [Google Scholar]
- Muwonge, I.D. Work Life Balance, Employee Engagement and Retention among Nurses of Mengo Hospital, Kampala. Ph.D. Thesis, Makerere University, Kampala, Uganda, 2022. [Google Scholar]
- Forde-Johnston, C.; Stoermer, F. Giving nurses a voice through ‘listening to staff’ conversations to inform nurse retention and reduce turnover. Br. J. Nurs. 2022, 31, 632–638. [Google Scholar] [CrossRef]
- Moscelli, G.; Sayli, M.; Mello, M. Staff Engagement, Coworkers’ Complementarity and Employee Retention: Evidence from English NHS Hospitals, 2022; IZA—Institute of Labor Economics: Bonn, Germany, 2022; ISSN 2365-9793. [Google Scholar]
- Guerrero, S.; Chênevert, D.; Kilroy, S. New graduate nurses’ professional commitment: Antecedents and outcomes. J. Nurs. Scholarsh. 2017, 49, 572–579. [Google Scholar] [CrossRef]
- Nurdiana, N.; Hariyati, R.T.S.; Gayatri, D. Head nurse strategy for increasing nurse retention: A factor analysis. Enferm. Clin. 2019, 29, 560–566. [Google Scholar] [CrossRef]
- Kim, E.G.; Jung, M.S.; Kim, J.K.; You, S.J. Factors affecting new graduate nurses’ intention on retention in hospitals: Focused on nursing organizational culture, empowering leadership and organizational socialization. J. Korean Acad. Nurs. Adm. 2020, 26, 31–41. [Google Scholar] [CrossRef]
- Cho, H.H.; Kim, E.Y. Effect of nursing organizational culture, organizational health, and job crafting on intent to stay among registered nurses. J. Korean Acad. Nurs. Adm. 2020, 26, 172–180. [Google Scholar] [CrossRef]
- Rigby, C.S.; Ryan, R.M. Self-determination theory in human resource development: New directions and practical considerations. Adv. Dev. Hum. Resour. 2018, 20, 133–147. [Google Scholar] [CrossRef]
- Bock, L. Work Rules! Insights from Inside Google That Will Transform How You Live and Lead; Grand Central: New York, NY, USA, 2015. [Google Scholar]
- Fowler, S. Why Motivating People Doesn’t Work... and What Does: The New Science of Leading, Energizing, and Engaging; Berrett-Koehler: Oakland, CA, USA, 2014. [Google Scholar]
- Truss, C.; Soane, E.; Edwards, C.; Wisdom, K.; Croll, A.; Burnett, J. Working Life: Employee Attitudes and Engagement 2006; Chartered Institute of Personnel and Development: London, UK, 2007. [Google Scholar]
- Gadolin, C.; Andersson, T. Healthcare quality improvement work: A professional employee perspective. Int. J. Health Care Qual. Assur. 2017, 30, 410–423. [Google Scholar] [CrossRef] [PubMed]
- García-Sierra, R.; Fernández-Castro, J. Relationships between leadership, structural empowerment, and engagement in nurses. J. Adv. Nurs. 2018, 74, 2809–2819. [Google Scholar] [CrossRef]
- Divyarajaram. Functions of Organisational Culture. Author Stream. 2014. Available online: www.authorstream.com/presentation/divyarajaram1390912-functions-of-organisational-culture/ (accessed on 1 May 2021).
- Thokozani, S.B.M.; Maseko, B. Strong vs. weak organizational culture: Assessing the impact on employee motivation. Arab. J. Bus. Manag. Rev. 2017, 7, 2–5. [Google Scholar]
- Odor, H.O. Organisational culture and dynamics. Glob. J. Manag. Bus. Res. 2018, 18, 23–29. [Google Scholar]
- Lee, E.; Jang, I. Nurses’ fatigue, job stress, organizational culture, and turnover intention: A culture–work–health model. West. J. Nurs. Res. 2020, 42, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, H.Y. Retention Rates and the Associated Risk Factors of Turnover among Newly Hired Nurses at South Korean Hospitals: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 10013. [Google Scholar] [CrossRef]
- Efendi, F.; Kurniati, A.; Bushy, A.; Gunawan, J. Concept analysis of nurse retention. Nurs. Health Sci. 2019, 21, 422–427. [Google Scholar] [CrossRef]
- Quek, S.J.; Thomson, L.; Houghton, R.; Bramley, L.; Davis, S.; Cooper, J. Distributed leadership as a predictor of employee engagement, job satisfaction and turnover intention in UK nursing staff. J. Nurs. Manag. 2021, 29, 1544–1553. [Google Scholar] [CrossRef]
- Steiner, S.; Cropley, M.; Simonds, L.; Heron, R. Reasons for staying with your employer: Identifying the key organizational predictors of employee retention within a global energy business. J. Occup. Environ. Med. 2020, 62, 289–295. [Google Scholar] [CrossRef]
- Kashyap, V.; Chaudhary, R. Linking employer brand image and work engagement: Modelling organizational identification and trust in organization as mediators. South Asian J. Hum. Resour. Manag. 2019, 6, 177–201. [Google Scholar] [CrossRef]
- Nekula, P.; Koob, C. Associations between culture of health and employee engagement in social enterprises: A cross-sectional study. PLoS ONE 2021, 16, e0245276. [Google Scholar] [CrossRef] [PubMed]
- Arasanmi, C.N.; Krishna, A. Employer branding: Perceived organisational support and employee retention–the mediating role of organisational commitment. Ind. Commer. Train. 2019, 51, 174–183. [Google Scholar] [CrossRef]
- Tsarenko, Y.; Leo, C.; Herman, H.M. When and why do social resources influence employee advocacy? The role of personal investment and perceived recognition. J. Bus. Res. 2018, 82, 260–268. [Google Scholar] [CrossRef]
- Halbesleben, J.R.; Wheeler, A.R. The relative roles of engagement and embeddedness in predicting job performance and intention to leave. Work. Stress 2008, 22, 242–256. [Google Scholar] [CrossRef]
- Parent, J.D.; Lovelace, K.J. Employee engagement, positive organizational culture and individual adaptability. Horizon 2018, 26, 206–214. [Google Scholar] [CrossRef]
- Braithwaite, J.; Westbrook, J.; Pawsey, M.; Greenfield, D.; Naylor, J.; Iedema, R.; Runciman, B.; Redman, S.; Jorm, C.; Robinson, M.; et al. A prospective, multi-method, multidisciplinary, multi-level, collaborative, social organizational design for researching health sector accreditation. BMC Health Serv. Res. 2006, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Flodgren, G.; Pomey, M.P.; Taber, S.A.; Eccles, M.P. Effectiveness of external inspection of compliance with standards in improving healthcare organization behaviour, healthcare professional behaviour or patient outcomes. Cochrane Database Syst. Rev. 2011, 9, CD008992. Available online: https://www.ncbi.nlm.nih.gov/pubmed/22071861 (accessed on 1 October 2022).
- Henseler, J.; Dijkstra, T.K.; Sarstedt, M.; Ringle, C.M.; Diamantopoulos, A.; Straub, D.W.; Ketchen, D.J., Jr.; Hair, J.F.; Hult, G.T.M.; Calantone, R.J. Common beliefs and reality about PLS: Comments on Rönkkö and Evermann. Organ. Res. Methods 2013, 17, 182–209. [Google Scholar] [CrossRef] [Green Version]
- Rigdon, E.E. Rethinking partial least squares path modeling: Breaking chains and forging ahead. Long Range Plan. 2014, 47, 161–167. [Google Scholar] [CrossRef]
- Henseler, J.; Hubona, G.; Ray, P.A. Using PLS path modeling in new technology research: Updated guidelines. Ind. Manag. Data Syst. 2016, 116, 2–20. [Google Scholar] [CrossRef]
- Kock, N. Common method bias in PLS-SEM: A full collinearity assessment approach. Int. J. e-Collab. (IJEC) 2015, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Black, W.C.; Babin, B.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Chin, W.W. The partial least squares approach to structural equation modeling. In Modern Methods for Business Research; Marcoulides, G.A., Ed.; Erlbaum: Mahwah, NJ, USA, 1998; pp. 295–358. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Shmueli, G.; Ray, S.; Estrada, J.M.V.; Chatla, S.B. The elephant in the room: Predictive performance of PLS models. J. Bus. Res. 2016, 69, 4552–4564. [Google Scholar] [CrossRef]
- Becker, J.-M.; Rai, A.; Rigdon, E. Predictive validity and formative measurement in structural equation modelling: Embracing practical relevance. In Proceedings of the International Conference on Information Systems (ICIS), Milano, Italy, 15–18 December 2013. [Google Scholar]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed, a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Kock, N. Advanced mediating effects tests, multigroup analyses, and measurement model assessments in PLS-based SEM. Int. J. e-Collab. 2014, 10, 1–13. [Google Scholar]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 3rd ed.; Sage: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Sheehan, C.; Tham, T.L.; Holland, P.; Cooper, B. Psychological contract fulfilment, engagement and nurse professional turnover intention. Int. J. Manpow. 2019, 40, 2–16. [Google Scholar] [CrossRef]
- Gambino, K. Motivation for entry, occupational commitment and intent to remain: A survey regarding Registered Nurse retention. J. Adv. Nurs. 2010, 66, 2532–2541. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Ekhsan, M.; Badrianti, Y.; Aeni, N. Employer Branding and Employee Retention: The Role of Mediating Employee Engagement. In Proceedings of the 1st International Conference on Research in Social Sciences and Humanities(ICoRSH 2020), Berlin, Germany, 17–19 December 2021; Atlantis Press: Amsterdam, The Netherlands, 2021; pp. 671–676. [Google Scholar]
- Olafsen, A.H.; Niemiec, C.P.; Halvari, H.; Deci, E.L.; Williams, G.C. On the dark side of work: A longitudinal analysis using self-determination theory. Eur. J. Work. Organ. Psychol. 2017, 26, 275–285. [Google Scholar] [CrossRef]


{kind=link}
| Frequency | % | Mean | SD | ||
|---|---|---|---|---|---|
| Gender | Female | 421 | 67 | ||
| Male | 207 | 33 | |||
| Age group | 21–31 | 452 | 72 | ||
| 32–42 | 166 | 26.4 | |||
| >42 | 10 | 1.6 | |||
| Marital status | Single | 430 | 68.5 | ||
| Married | 198 | 31.5 | |||
| Qualification | Graduate/Diploma | 503 | 80.1 | ||
| Postgraduate | 124 | 19.7 | |||
| Doctorate | 1 | 0.2 | |||
| Designation | Staff nurse | 461 | 73.4 | ||
| Supervisor/In charge | 148 | 23.6 | |||
| Head nurse | 19 | 3 | |||
| Total experience | <3 years | 350 | 55.7 | ||
| 3–6 years | 212 | 33.8 | |||
| 6–9 years | 53 | 8.4 | |||
| >9 years | 13 | 2.1 | |||
| Income (in rupees, p.a.) | <0.3 million | 408 | 65 | ||
| 0.3–0.5 million | 199 | 31.7 | |||
| >0.5 million | 21 | 3.3 | |||
| Employee engagement | 1.98 | 0.642 | |||
| Organizational culture | 1.98 | 0.89 | |||
| Retention | 2.58 | 0.764 | |||
| Cronbach’s Alpha | rho_A | Composite Reliability | Average Variance Extracted (AVE) | |
|---|---|---|---|---|
| Employee engagement | 0.790 | 0.790 | 0.856 | 0.544 |
| Organizational culture | 0.728 | 0.729 | 0.830 | 0.550 |
| Retention | 0.841 | 0.842 | 0.887 | 0.611 |
| Employee Engagement | Organizational Culture | Retention | ||||
|---|---|---|---|---|---|---|
| F&L | HTMT | F&L | HTMT | F&L | HTMT | |
| Employee engagement | ||||||
| 0.737 | 0.702 | 0.885 | ||||
| Organizational culture | 0.742 | |||||
| Retention | 0.672 | 0.824 | 0.650 | 0.829 | 0.782 | |
| Explanatory Power: R Square | R Square | R Square Adjusted |
|---|---|---|
| Retention | 0.514 | 0.513 |
| Organizational culture | 0.493 | 0.493 |
| Effect Size: F Square | ||
| Employee engagement -> retention | 0.189 | |
| Organizational Culture -> retention | 0.129 | |
| Employee engagement -> org. culture | 0.974 | |
| Q2 | Model Fit | |
|---|---|---|
| Culture | 0.489 | |
| Retention | 0.447 | |
| SRMR | 0.059 |
| DIRECT EFFECTS | |||
|---|---|---|---|
| Path | Coefficient | T Statistics | p-Values |
| Employee engagement -> retention | 0.426 * | 7.025 | 0.000 |
| Employee engagement -> organizational culture | 0.704 * | 31.792 | 0.000 |
| Organizational Culture -> retention | 0.352 * | 7.971 | 0.000 |
| INDIRECT EFFECTS | |||
| Path | Coefficient | T Statistics | p-Values |
| Employee engagement -> organizational culture -> retention | 0.248 * | 6.579 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goyal, R.; Kaur, G. Determining the Role of Employee Engagement in Nurse Retention along with the Mediation of Organizational Culture. Healthcare 2023, 11, 760. https://doi.org/10.3390/healthcare11050760
Goyal R, Kaur G. Determining the Role of Employee Engagement in Nurse Retention along with the Mediation of Organizational Culture. Healthcare. 2023; 11(5):760. https://doi.org/10.3390/healthcare11050760
Chicago/Turabian StyleGoyal, Ridhya, and Gurvinder Kaur. 2023. "Determining the Role of Employee Engagement in Nurse Retention along with the Mediation of Organizational Culture" Healthcare 11, no. 5: 760. https://doi.org/10.3390/healthcare11050760