
Foreign Healthcare Professionals in Germany: A Questionnaire Survey Evaluating Discrimination Experiences and Equal Treatment at Two Large University Hospitals
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Questionnaire Survey
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
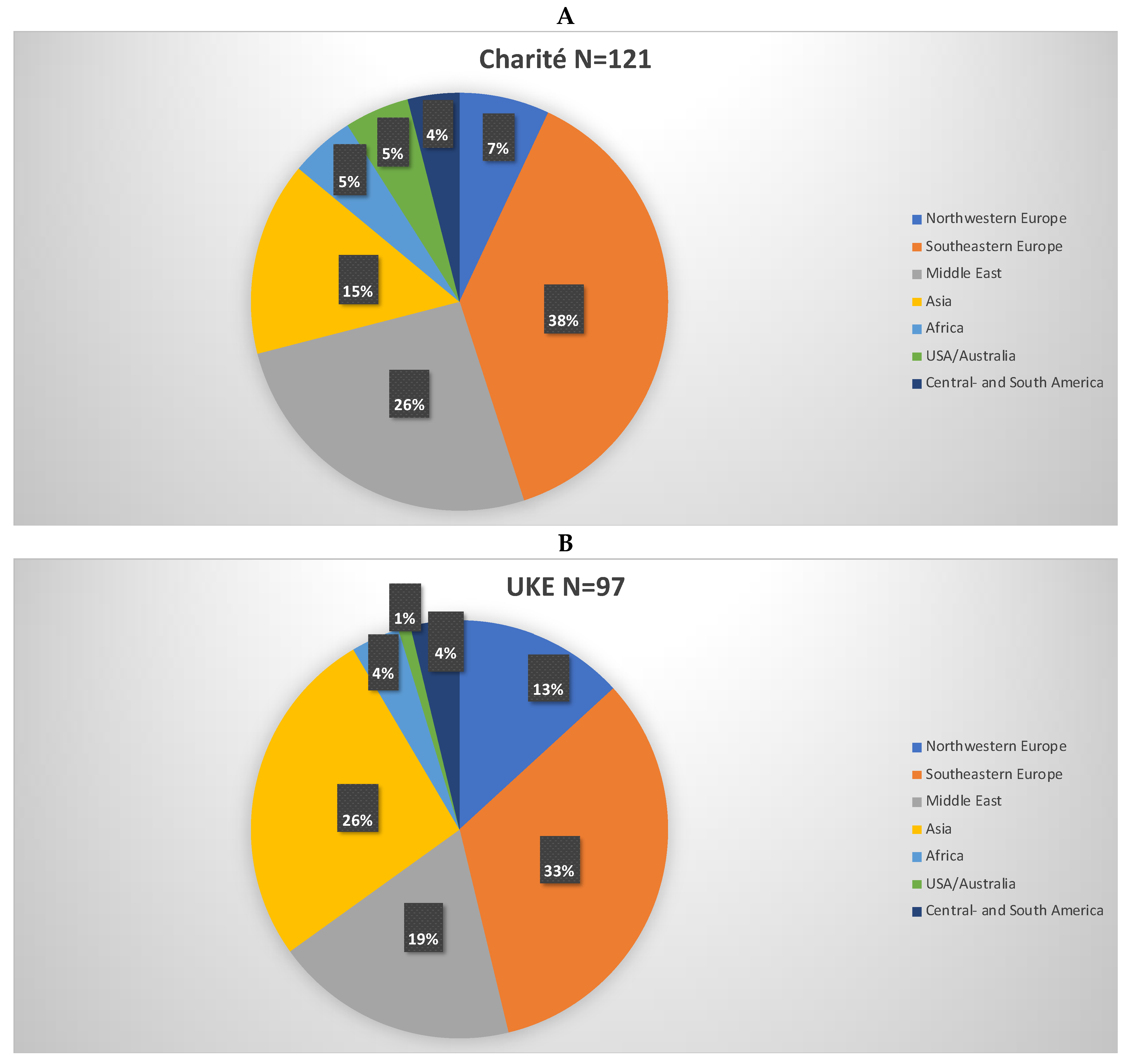
3.1. Study Population
3.2. Labour Market Access
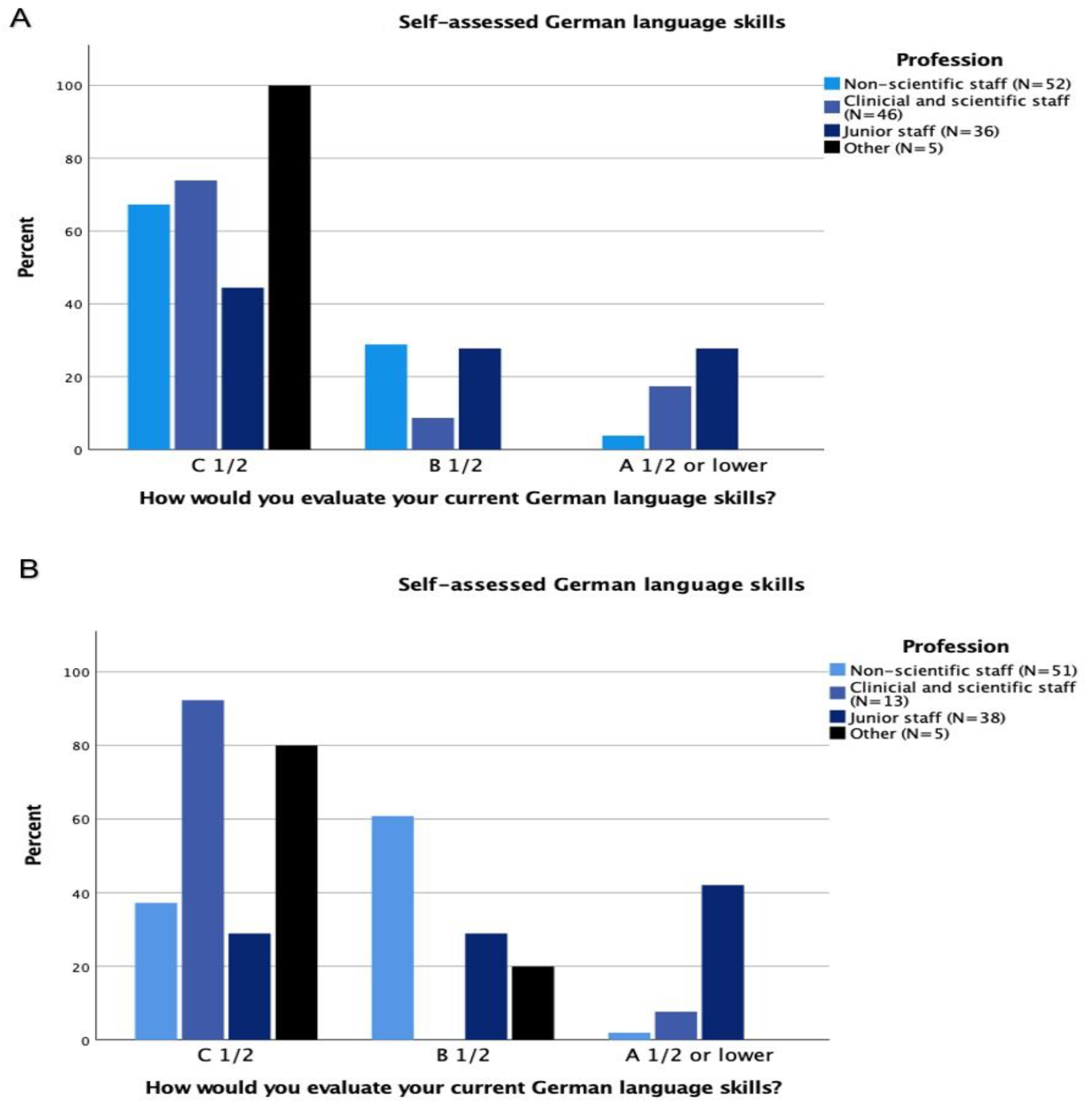
3.3. Language
3.4. Workplace Discrimination Experiences
3.5. Perception of Equality at Work
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistisches Bundesamt 2019. Bevölkerung und Erwerbstätigkeit. Bevölkerung mit Migrationshintergrund—Ergebnisse des Mikrozensus 2019. Fachserie 1 Reihe 22. Wiesbaden 2020. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Publikationen/_publikationen-innen-migrationshintergrund.html (accessed on 3 September 2022).
- Young, R.; Noble, J.; Mahon, A.; Maxted, M.; Grant, J.; Sibbald, B. Evaluation of international recruitment of health professionals in England. J. Health Serv. Res. Policy 2010, 15, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Hörmann, G. Migration and health—From deficiency analysis to diversity vision? Gesundheitswesen 2011, 73, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Bundesärztekammer 2020. Auslaendische Ärztinnen-und Ärzte 2020. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/pdf-Ordner/Statistik_2020/Tabelle_10-Auslaendische_AErztinnen_AErzte.pdf (accessed on 3 September 2022).
- OECD. Stat. Health Workforce Migration. Available online: https://stats.oecd.org/Index.aspx (accessed on 3 September 2022).
- Clark, P.F.; Stewart, J.B. The Globalization of the Labour Market for Health-Care Professionals. Int. Labour Rev. 2008, 145, 37–64. [Google Scholar] [CrossRef]
- Hall, S. Populismus, Hegemonie, Globalisierung (German); Argument-Verlag: Hamburg, Germany, 2013; p. 259. [Google Scholar]
- Hall, S.; Gieben, B. The Formations of Modernity; Polity Press: Cambridge, UK, 1991. [Google Scholar]
- Hall, S. The Spectacle of the ‘Other’; Sage & the Open University: Newbury Park, CA, USA, 1997. [Google Scholar]
- Gramsci, A. Prison Notebooks; Columbia University Press: New York, NY, USA, 1992. [Google Scholar]
- Racine, L. Racialization in nursing: Rediscovering Antonio Gramsci’s concepts of hegemony and subalternity. Nurs. Inq. 2021, 28, e12398. [Google Scholar] [CrossRef] [PubMed]
- Hall, S. Stuart Hall: Race, the Floating Signifier; Mass Media Education Foundation: Northampton, UK, 2002. [Google Scholar]
- Hall, S. Modernity: An Introduction to Modern Societies; Polity Press in Association with Blackwell: Cambridge, UK, 2003. [Google Scholar]
- Hall, S. Cultural Identity and Diaspora in Colonial Discourse and Post-Colonial Theory by Patrick Williams; Laura Chrisman: London, UK, 2005. [Google Scholar]
- Balibar, E. Politics and the Other Scene; Verso: London, UK; New York, NY, USA, 2002; p. 176. [Google Scholar]
- Foucault, M. The Order of Things; Routledge: London, UK, 1975. [Google Scholar]
- Hagey, R.; Choudhry, U.; Guruge, S.; Turrittin, J.; Collins, E.; Lee, R. Immigrant nurses’ experience of racism. J. Nurs. Sch. 2001, 33, 389–394. [Google Scholar] [CrossRef]
- Foroutan, N.; Beigang, S. Ergebnisse einer Repräsentativ- und einer Betroffenenbefragung der Antidiskriminierungsstelle des Bundes. Available online: https://www.antidiskriminierungsstelle.de/SharedDocs/downloads/DE/publikationen/Expertisen/expertise_diskriminierungserfahrungen_in_deutschland.html (accessed on 17 September 2022).
- Klingler, C. Herausforderungen in der Integration Migrierter Ärzte: Die Perspektiven der Migranten und des Aufnehmenden Systems (German). Ph.D. Thesis, Ludwig-Maximilians-Universität München, München, Germany, 2019. Available online: https://edoc.ub.uni-muenchen.de/24145/2/Klingler_Corinna.pdf (accessed on 1 February 2022).
- Roth, C.; Berger, S.; Krug, K.; Mahler, C.; Wensing, M. Internationally trained nurses and host nurses’ perceptions of safety culture, work-life-balance, burnout, and job demand during workplace integration: A cross-sectional study. BMC Nurs. 2021, 20, 77. [Google Scholar] [CrossRef]
- Solum, E.M.; Viken, B.; Lyberg, A. First Year’s Work Experiences of Foreign Educated Nurses Coming to Norway From Other European Countries. SAGE Open Nurs. 2020, 6, 2377960820970003. [Google Scholar] [CrossRef]
- Marsching, B. Migration. Experiences of Philippine Nurses in Vorarlberg and Vienna. Available online: https://utheses.univie.ac.at/detail/7862# (accessed on 21 September 2022).
- Halley, M.C.; Rustagi, A.S.; Torres, J.S.; Linos, E.; Plaut, V.; Mangurian, C.; Choo, E.; Linos, E. Physician mothers’ experience of workplace discrimination: A qualitative analysis. BMJ 2018, 363, k4926. [Google Scholar] [CrossRef] [Green Version]
- Rauh, B.; Strohmer, J.; Weber, J.M. Das Unbehagen Im und Mit Dem Subjekt (German); Verlag Barbara Budrich: Leverkusen-Opladen, Germany, 2019. [Google Scholar]
- Foroutan, N. Die postmigrantische Gesellschaft: Ein Versprechen der Pluralen Demokratie (German); Transcript Verlag: Bielefeld, Germany, 2021. [Google Scholar]
- Nwabuzo, O. Racism and Discrimination in the Context of Migration to Europe. European Network Against Racism Shadow Report 2015–2016. OECD 2018. Available online: https://ec.europa.eu/migrant-integration/library-document/racism-and-discrimination-context-migration-europe-0_en (accessed on 3 September 2022).
- Supik, L. Statistik und Rassismus. Das Dilemma der Erfassung von Ethnizität (German); Campus Verlag: Frankfurt, Germany, 2014. [Google Scholar]
- Zick, A.; Kuepper, B. Die Geforderte Mitte Rechtsextreme und Demokratiegefaehrdende Einstellungen in Deutschland 2020/21 (German); Friedrich-Ebert Stiftung: Bonn, Germany, 2020. [Google Scholar]
- Papendick, M.; Rees, J.; Waeschle, F.; Zick, A. Multidimensionaler Erinnerungsmonitor: Studie III. Available online: https://pub.uni-bielefeld.de/record/2949171 (accessed on 3 September 2022).
- Zick, A. Vorurteile und Rassismus eine Sozialpsychologische Analyse (German); Waxmann: München, Germany, 1997. [Google Scholar]
- Hansen, N. Die Verarbeitung von Diskriminierung. Psychologische Grundlagen und Anwendungsperspektiven (German); Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2009. [Google Scholar]
- International Convention on the Elimination of All Forms of Racial Discrimination. Available online: https://www.ohchr.org/sites/default/files/cerd.pdf (accessed on 3 September 2022).
- Sellers, R.M.; Shelton, J.N. The role of racial identity in perceived racial discrimination. J. Pers. Soc. Psychol. 2003, 84, 1079–1092. [Google Scholar] [CrossRef]
- Likupe, G. Experiences of African nurses and the perception of their managers in the NHS. J Nurs Manag. 2015, 23, 231–241. [Google Scholar] [CrossRef]
- Woodhams, C.; Williams, M.; Dacre, J.; Parnerkar, I.; Sharma, M. Retrospective observational study of ethnicity-gender pay gaps among hospital and community health service doctors in England. BMJ Open 2021, 11, e051043. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.; Goudie, R.; Sutton, M.; Gravelle, H.; Elliott, R.; Hole, A.R.; Ma, A.; Sibbald, B.; Skåtun, D. Determinants of general practitioners’ wages in England. Health Econ. 2011, 20, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, D.; Zhang, J.; Salway, S.; Nazroo, J.; Booth, A.; Villarroel-Williams, N.; Bécares, L.; Esmall, A. Ethnic Inequalities in Healthcare: A Rapid Evidence Review. NHS Race and Health Observatory 2022. Available online: https://www.nhsrho.org/wp-content/uploads/2022/02/RHO-Rapid-Review-Final-Report_v.7.pdf (accessed on 3 September 2022).
- Hallett, N.; Wagstaff, C.; Barlow, T. Nursing students’ experiences of violence and aggression: A mixed-methods study. Nurse Educ. Today 2021, 105, 105024. [Google Scholar] [CrossRef] [PubMed]
- Alexis, O. Internationally recruited nurses’ experiences in England: A survey approach. Nurs. Outlook 2015, 63, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Bond, S.; Merriman, C.; Walthall, H. The experiences of international nurses and midwives transitioning to work in the UK: A qualitative synthesis of the literature from 2010 to 2019. Int. J. Nurs. Stud. 2020, 110, 103693. [Google Scholar] [CrossRef]
- O’Brien, T.; Ackroyd, S. Understanding the recruitment and retention of overseas nurses: Realist case study research in National Health Service Hospitals in the UK. Nurs Inq. 2012, 19, 39–50. [Google Scholar] [CrossRef]
- Scammell, J.M.; Olumide, G. Racism and the mentor-student relationship: Nurse education through a white lens. Nurse Educ. Today 2012, 32, 545–550. [Google Scholar] [CrossRef]
- West, M.; Dawson, J.; Kaur, M. Making the Difference Diversity and Inclusion in the NHS. The Kings Fund 2015. Available online: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Making-the-difference-summary-Kings-Fund-Dec-2015.pdf (accessed on 3 September 2022).
- Rhead, R.D.; Chui, Z.; Bakolis, I.; Gazard, B.; Harwood, H.; MacCrimmon, S.; Woodhead, C.; Hatch, S.L. Impact of workplace discrimination and harassment among National Health Service staff working in London trusts: Results from the TIDES study. BJPsych Open 2020, 7, e10. [Google Scholar] [CrossRef]
- Johnson, J.; Cameron, L.; Mitchinson, L.; Parmar, M.; Opio-Te, G.; Louch, G.; Grange, A. An investigation into the relationships between bullying, discrimination, burnout and patient safety in nurses and midwives: Is burnout a mediator? J. Res. Nurs. 2019, 24, 604–619. [Google Scholar] [CrossRef] [Green Version]
- Raj, A.; Kumra, T.; Darmstadt, G.L.; Freund, K.M. Achieving Gender and Social Equality: More Than Gender Parity Is Needed. Acad. Med. 2019, 94, 1658–1664. [Google Scholar] [CrossRef]
- VanIneveld, C.H.; Cook, D.J.; Kane, S.L.; King, D. Discrimination and abuse in internal medicine residency. The Internal Medicine Program Directors of Canada. J. Gen. Intern. Med. 1996, 11, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Carr, P.L.; Ash, A.S.; Friedman, R.H.; Szalacha, L.; Barnett, R.C.; Palepu, A.; Moskowitz, M.M. Faculty perceptions of gender discrimination and sexual harassment in academic medicine. Ann. Intern. Med. 2000, 132, 889–896. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Charité | UKE | |||
|---|---|---|---|---|
| n | % | n | % | |
| Gender | 136 | 100 | 107 | 100 |
| Female | 83 | 61 | 72 | 66 |
| Male | 53 | 39 | 34 | 34 |
| Other | 0 | 1 | 1 | |
| Country of birth | 121 | 100 | 97 | 100 |
| EU | 40 | 33 | 33 | 30 |
| Non-EU | 81 | 67 | 64 | 59 |
| Degrees | 132 | 100 | 107 | 100 |
| Abroad | 75 | 53 | 75 | 69 |
| Germany | 57 | 40 | 29 | 27 |
| Vocational training | 25 | 17.6 | 15 | 14 |
| University degree | 110 | 77.5 | 92 | 86 |
| Bachelor | 25 | 17.6 | 36 | 33 |
| Master | 27 | 19 | 29 | 27 |
| Diploma | 7 | 5 | 8 | 7 |
| PhD/doctorate | 12 | 8.5 | 14 | 13 |
| Medical Doctor | 46 | 32 | ||
| Other | 4 | 3 | 5 | 4.5 |
| Citizenship | 142 | 100 | 109 | 100 |
| German | 44 | 31 | 26 | 24 |
| Non-German | 98 | 69 | 83 | 76 |
| Residence status | 98 | 100 | 77 | 100 |
| Temporary (only employees born outside the European Union) | 41 | 43 | 38 | 49 |
| Permanent | 54 | 57 | 39 | 50 |
| NA | 3 | 3 | 6 | 8 |
| Survey language | 142 | 100 | 109 | 100 |
| German | 102 | 72 | 57 | 52 |
| English | 40 | 28 | 52 | 48 |
| Charité | UKE | |||
|---|---|---|---|---|
| Position | N | Percentage (%) | N | Percentage (%) |
| Three categories: | ||||
| Clinical and scientific staff | 46 | 32.4 | 14 | 12.8 |
| Junior staff | 36 | 25.4 | 38 | 34.9 |
| Non-scientific staff | 52 | 36.6 | 51 | 46.8 |
| Other | 5 | 3.5 | 5 | 4.6 |
| NA | 3 | 2.1 | 1 | 0.9 |
| Total | 142 | 100 | 109 | 100 |
| Clinical and scientific staff | ||||
| Resident | 22 | 47.8 | 4 | 28.5 |
| Specialist doctor | 10 | 21.7 | 6 | 42.9 |
| Researcher | 13 | 28.3 | 2 | 14.3 |
| Other | 1 | 2.2 | 0 | 0 |
| NA | 0 | 0 | 2 | 14.3 |
| Total | 46 | 100 | 14 | 100 |
| Junior staff | ||||
| PhD student | 14 | 38.9 | 19 | 50 |
| Postdoc | 13 | 36.1 | 18 | 47.4 |
| Other | 6 | 16.7 | 1 | 2.6 |
| NA | 3 | 8.3 | 0 | 0 |
| Total | 36 | 100 | 38 | 100 |
| Non-scientific staff | ||||
| Nurse | 39 | 75 | 43 | 84.3 |
| Technologist | 13 | 25 | 8 | 15.7 |
| Total | 52 | 100 | 51 | 100 |
| A | |||||
|---|---|---|---|---|---|
| Charité—Country of Birth | |||||
| Frequency | Percentage | Valid Percentage | Cumulative Percentage | ||
| Valid | Albania | 7 | 4.9 | 5.8 | 5.8 |
| Belarus | 1 | 0.7 | 0.8 | 6.6 | |
| Bosnia and Herzegovina | 1 | 0.7 | 0.8 | 7.4 | |
| Brazil | 2 | 1.4 | 1.7 | 9.1 | |
| Bulgaria | 4 | 2.8 | 3.3 | 12.4 | |
| China | 6 | 4.2 | 5.0 | 17.4 | |
| Colombia | 1 | 0.7 | 0.8 | 18.2 | |
| Croatia | 3 | 2.1 | 2.5 | 20.7 | |
| Czech Republic | 1 | 0.7 | 0.8 | 21.5 | |
| Estonia | 1 | 0.7 | 0.8 | 22.3 | |
| Ethiopia | 1 | 0.7 | 0.8 | 23.1 | |
| France | 2 | 1.4 | 1.7 | 24.8 | |
| Ghana | 1 | 0.7 | 0.8 | 25.6 | |
| Greece | 2 | 1.4 | 1.7 | 27.3 | |
| Honduras | 1 | 0.7 | 0.8 | 28.1 | |
| Hungary | 2 | 1.4 | 1.7 | 29.8 | |
| India | 2 | 1.4 | 1.7 | 31.4 | |
| Indonesia | 2 | 1.4 | 1.7 | 33.1 | |
| Iran | 3 | 2.1 | 2.5 | 35.5 | |
| Iraq | 1 | 0.7 | 0.8 | 36.4 | |
| Israel | 1 | 0.7 | 0.8 | 37.2 | |
| Italy | 8 | 5.6 | 6.6 | 43.8 | |
| Kazakhstan | 4 | 2.8 | 3.3 | 47.1 | |
| Kenya | 1 | 0.7 | 0.8 | 47.9 | |
| Mexico | 3 | 2.1 | 2.5 | 50.4 | |
| Mongolia | 1 | 0.7 | 0.8 | 51.2 | |
| Netherlands | 1 | 0.7 | 0.8 | 52.1 | |
| Philippines | 1 | 0.7 | 0.8 | 52.9 | |
| Poland | 8 | 5.6 | 6.6 | 59.5 | |
| Portugal | 2 | 1.4 | 1.7 | 61.2 | |
| Romania | 2 | 1.4 | 1.7 | 62.8 | |
| Russia | 4 | 2.8 | 3.3 | 66.1 | |
| Saudi Arabia | 3 | 2.1 | 2.5 | 68.6 | |
| Serbia | 2 | 1.4 | 1.7 | 70.2 | |
| South Africa | 1 | 0.7 | 0.8 | 71.1 | |
| Spain | 3 | 2.1 | 2.5 | 73.6 | |
| Sri Lanka | 2 | 1.4 | 1.7 | 75.2 | |
| Suisse | 1 | 0.7 | 0.8 | 76.0 | |
| Sweden | 1 | 0.7 | 0.8 | 76.9 | |
| Syria | 5 | 3.5 | 4.1 | 81.0 | |
| Tajikistan | 2 | 1.4 | 1.7 | 82.6 | |
| Thailand | 2 | 1.4 | 1.7 | 84.3 | |
| Tunisia | 1 | 0.7 | 0.8 | 85.1 | |
| Turkey | 7 | 4.9 | 5.8 | 90.9 | |
| Ukraine | 2 | 1.4 | 1.7 | 92.6 | |
| USA | 7 | 4.9 | 5.8 | 98.3 | |
| Russia | 1 | 0.7 | 0.8 | 99.2 | |
| Vietnam | 1 | 0.7 | 0.8 | 100.0 | |
| Total | 121 | 85.2 | 100.0 | ||
| NA | 21 | 14.8 | |||
| Total | 142 | 100.0 | |||
| B | |||||
| UKE—Country of Birth | |||||
| Frequency | Percentage | Valid Percentage | Cumulative Percentage | ||
| Valid | Albania | 1 | 0.9 | 1.0 | 1.0 |
| Argentina | 1 | 0.9 | 1.0 | 2.1 | |
| Austria | 1 | 0.9 | 1.0 | 3.1 | |
| Belarus | 1 | 0.9 | 1.0 | 4.1 | |
| Belgium | 1 | 0.9 | 1.0 | 5.2 | |
| Bosnia and Herzegovina | 2 | 1.8 | 2.1 | 7.2 | |
| Brazil | 1 | 0.9 | 1.0 | 8.2 | |
| Bulgaria | 1 | 0.9 | 1.0 | 9.3 | |
| Cameroon | 1 | 0.9 | 1.0 | 10.3 | |
| China | 5 | 4.6 | 5.2 | 15.5 | |
| Croatia | 3 | 2.8 | 3.1 | 18.6 | |
| Denmark | 1 | 0.9 | 1.0 | 19.6 | |
| Finland | 1 | 0.9 | 1.0 | 20.6 | |
| France | 5 | 4.6 | 5.2 | 25.8 | |
| Georgia | 1 | 0.9 | 1.0 | 26.8 | |
| Greece | 1 | 0.9 | 1.0 | 27.8 | |
| India | 3 | 2.8 | 3.1 | 30.9 | |
| Iran | 9 | 8.3 | 9.3 | 40.2 | |
| Ireland | 1 | 0.9 | 1.0 | 41.2 | |
| Israel | 2 | 1.8 | 2.1 | 43.3 | |
| Italy | 3 | 2.8 | 3.1 | 46.4 | |
| Japan | 2 | 1.8 | 2.1 | 48.5 | |
| Kazakhstan | 1 | 0.9 | 1.0 | 49.5 | |
| Kosovo | 2 | 1.8 | 2.1 | 51.5 | |
| Latvia | 1 | 0.9 | 1.0 | 52.6 | |
| Lebanon | 1 | 0.9 | 1.0 | 53.6 | |
| Luxembourg | 1 | 0.9 | 1.0 | 54.6 | |
| Morocco | 1 | 0.9 | 1.0 | 55.7 | |
| Nepal | 1 | 0.9 | 1.0 | 56.7 | |
| Netherlands | 1 | 0.9 | 1.0 | 57.7 | |
| Philippines | 15 | 13.8 | 15.5 | 73.2 | |
| Poland | 5 | 4.6 | 5.2 | 78.4 | |
| Portugal | 3 | 2.8 | 3.1 | 81.4 | |
| Romania | 2 | 1.8 | 2.1 | 83.5 | |
| Russia | 1 | 0.9 | 1.0 | 84.5 | |
| Saudi Arabia | 2 | 1.8 | 2.1 | 86.6 | |
| Serbia | 2 | 1.8 | 2.1 | 88.7 | |
| Somalia | 1 | 0.9 | 1.0 | 89.7 | |
| Spain | 2 | 1.8 | 2.1 | 91.8 | |
| Syria | 3 | 2.8 | 3.1 | 94.8 | |
| Tunesia | 1 | 0.9 | 1.0 | 95.9 | |
| United Arab Emirates | 1 | 0.9 | 1.0 | 96.9 | |
| USA | 1 | 0.9 | 1.0 | 97.9 | |
| Vietnam | 2 | 1.8 | 2.1 | 100.0 | |
| Total | 97 | 89.0 | 100.0 | ||
| NA | 12 | 11.0 | |||
| Total | 109 | 100.0 | |||
| Non-Scientific Staff | Clinical and Scientific Staff | Junior Staff | Other | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Charité | Yes | No | Missing | Yes | No | Missing | Yes | No | Missing | Yes | No | Missing | |
| Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | ||
| Experience of discrimination | by peers | 16 | 34 | 2 | 8 | 37 | 1 | 2 | 34 | 0 | 0 | 4 | 1 |
| by superiors | 8 | 39 | 5 | 9 | 35 | 2 | 4 | 30 | 2 | 2 | 0 | ||
| by patients | 5 | 42 | 5 | 4 | 39 | 3 | 4 | 31 | 1 | 4 | 1 | ||
| Non-Scientific Staff | Clinical and Scientific Staff | Junior Staff | Other | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UKE | Yes | No | Missing | Yes | No | Missing | Yes | No | Missing | Yes | No | Missing | |
| Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | Number | ||
| Experience of discrimination based on the migration background | by peers | 18 | 28 | 5 | 1 | 13 | 0 | 5 | 33 | 0 | 2 | 3 | 0 |
| by superiors | 11 | 34 | 6 | 0 | 14 | 0 | 3 | 34 | 1 | 2 | 3 | 0 | |
| by patients | 9 | 31 | 11 | 2 | 8 | 4 | 0 | 4 | 34 | 0 | 5 | 0 | |
| Perception of Equal Treatment | Charité | UKE | ||
|---|---|---|---|---|
| N | % | N | % | |
| Contract | 138 | 100 | 102 | 100 |
| Yes | 112 | 81.2 | 84 | 82.4 |
| No | 26 | 18.8 | 18 | 17.6 |
| Weekly working hours | 140 | 100 | 104 | 100 |
| Yes | 127 | 90.7 | 89 | 85.6 |
| No | 13 | 9.3 | 15 | 14.4 |
| Working times | 120 | 100 | 95 | 100 |
| Yes | 101 | 84.2 | 82 | 86.3 |
| No | 19 | 15.8 | 13 | 13.7 |
| Payment | 136 | 100 | 100 | 100 |
| Yes | 108 | 79.4 | 82 | 82 |
| No | 28 | 20.6 | 18 | 18 |
| Distribution of tasks within team | 137 | 100 | 100 | 100 |
| Yes | 107 | 78.1 | 75 | 75 |
| No | 30 | 21.9 | 25 | 25 |
| Appreciation of work performance by colleagues | 133 | 100 | 100 | 100 |
| Yes | 109 | 82 | 74 | 74 |
| No | 24 | 18 | 26 | 26 |
| Appreciation of work performance by superiors | 132 | 100 | 103 | 100 |
| Yes | 99 | 75 | 77 | 74.8 |
| No | 33 | 25 | 26 | 25.2 |
| Appreciation of work performance by patients | 99 | 100 | 63 | 100 |
| Yes | 89 | 89.9 | 47 | 74.6 |
| No | 10 | 10.1 | 16 | 25.4 |
| Opportunities for further training and promotion | 129 | 100 | 94 | 100 |
| Yes | 79 | 61.2 | 63 | 67 |
| No | 50 | 38.8 | 31 | 33 |
| Opportunity to express ones opinion in discussions among colleagues | 135 | 100 | 96 | 100 |
| Yes | 108 | 80 | 77 | 80.2 |
| No | 27 | 20 | 19 | 19.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Can, E.; Konrad, C.M.; Khan-Gökkaya, S.; Molwitz, I.; Nawabi, J.; Yamamura, J.; Hamm, B.; Keller, S. Foreign Healthcare Professionals in Germany: A Questionnaire Survey Evaluating Discrimination Experiences and Equal Treatment at Two Large University Hospitals. Healthcare 2022, 10, 2339. https://doi.org/10.3390/healthcare10122339
Can E, Konrad CM, Khan-Gökkaya S, Molwitz I, Nawabi J, Yamamura J, Hamm B, Keller S. Foreign Healthcare Professionals in Germany: A Questionnaire Survey Evaluating Discrimination Experiences and Equal Treatment at Two Large University Hospitals. Healthcare. 2022; 10(12):2339. https://doi.org/10.3390/healthcare10122339
Chicago/Turabian StyleCan, Elif, Clara Milena Konrad, Sidra Khan-Gökkaya, Isabel Molwitz, Jawed Nawabi, Jin Yamamura, Bernd Hamm, and Sarah Keller. 2022. "Foreign Healthcare Professionals in Germany: A Questionnaire Survey Evaluating Discrimination Experiences and Equal Treatment at Two Large University Hospitals" Healthcare 10, no. 12: 2339. https://doi.org/10.3390/healthcare10122339