

Exploration of Sex and Age-Based Associations in Clinical Characteristics, Predictors of Severity, and Duration of Stay among COVID-19 Patients at the University Hospital of Saudi Arabia

 , , and
, , and
Abstract
:1. Introduction
1.1. Objectives of the Study
1.1.1. Aim of the Study
1.1.2. Specific Objectives
- To assess the severity of different symptoms and signs of COVID-19 disease that developed in patients.
- To investigate the differences in clinical variables with age, sex, and different co-morbidities.
- To compare the outcome of COVID-19 patients by severity levels.
- To assess the predictors of severity and duration of hospital stay (DoHS).
2. Materials and Methods
2.1. Study Design and Setting
2.2. Population
2.3. Institutional Ethical Approval
2.4. Data Collection
2.5. Data Management and Analysis Plan
3. Results
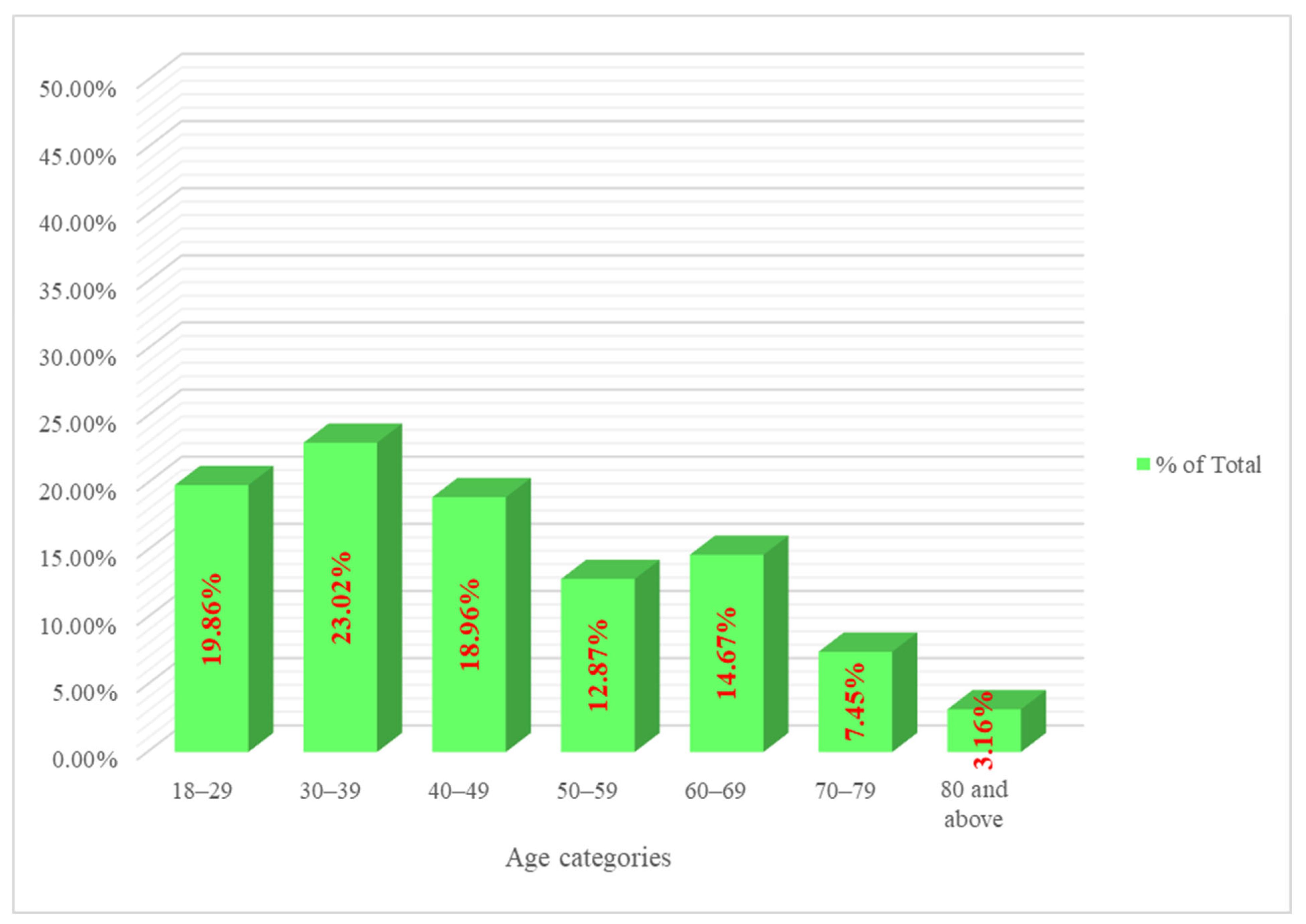
3.1. Age and Sex
3.2. Clinical Characteristics of COVID-19 among Study Participants
3.3. A. Different Age Groups
3.4. B. Sex-Based Differences
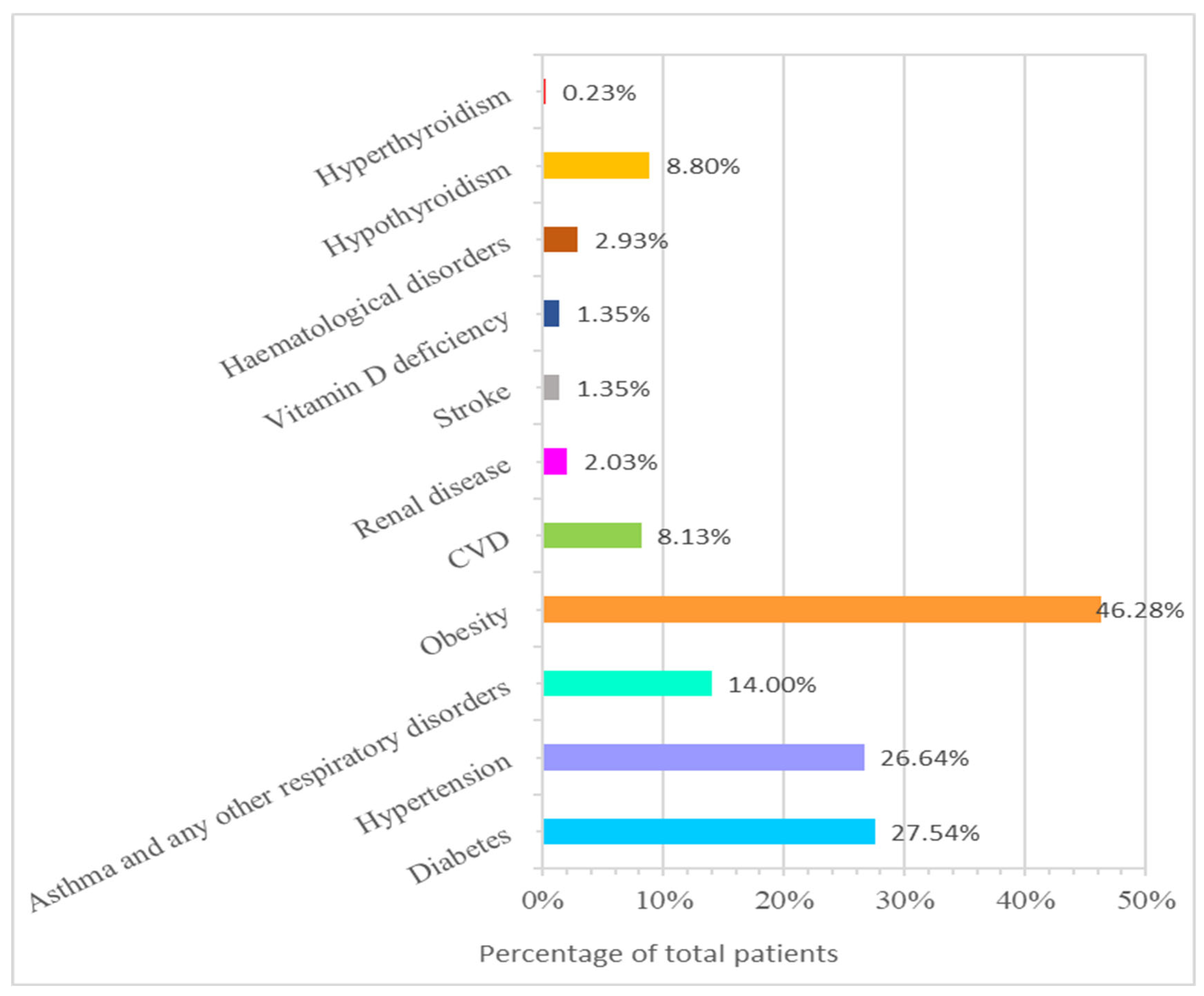
3.5. Co-Morbidities in the Study Participants
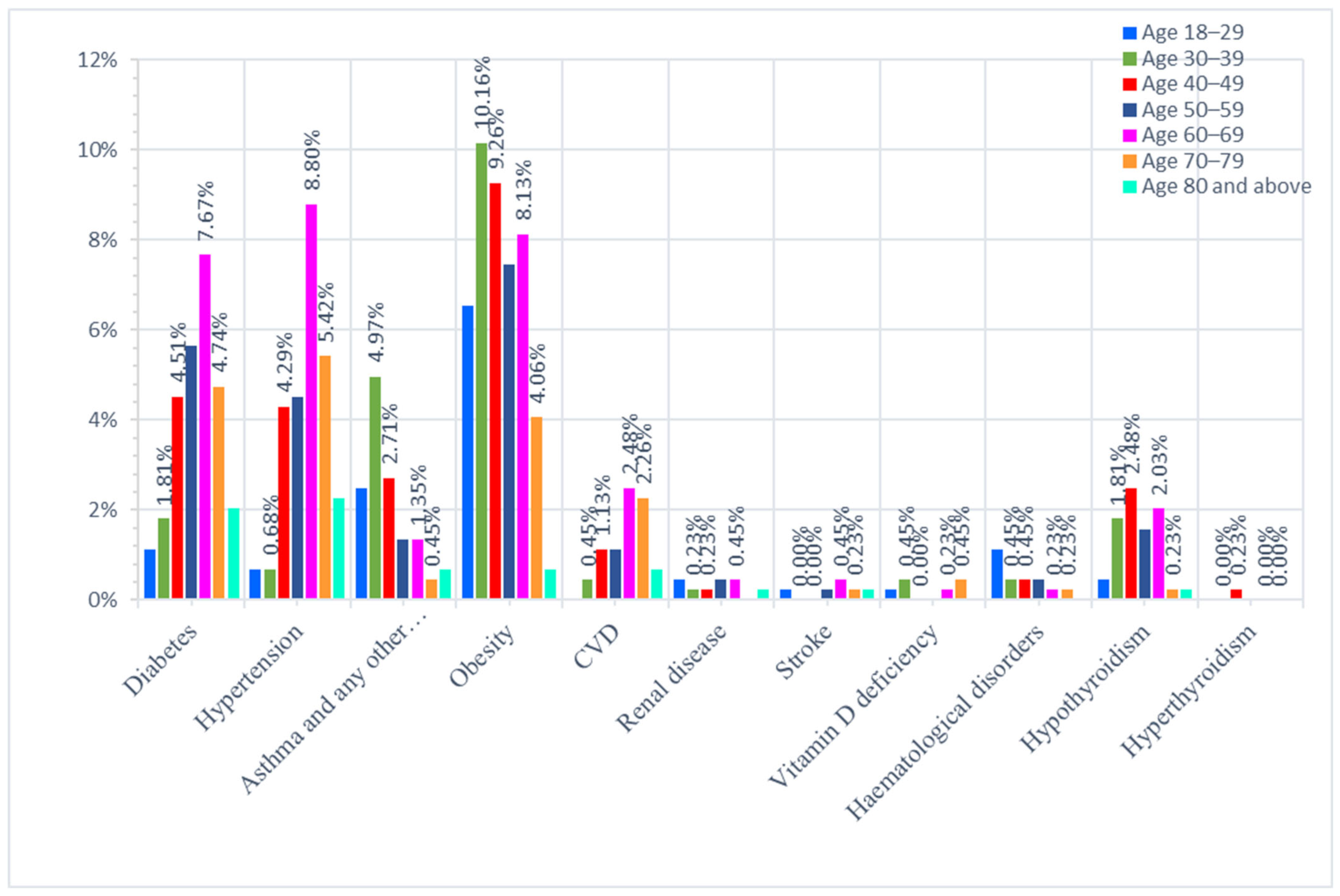
3.6. A. Different Age Groups
3.7. B. Sex-Based Differences
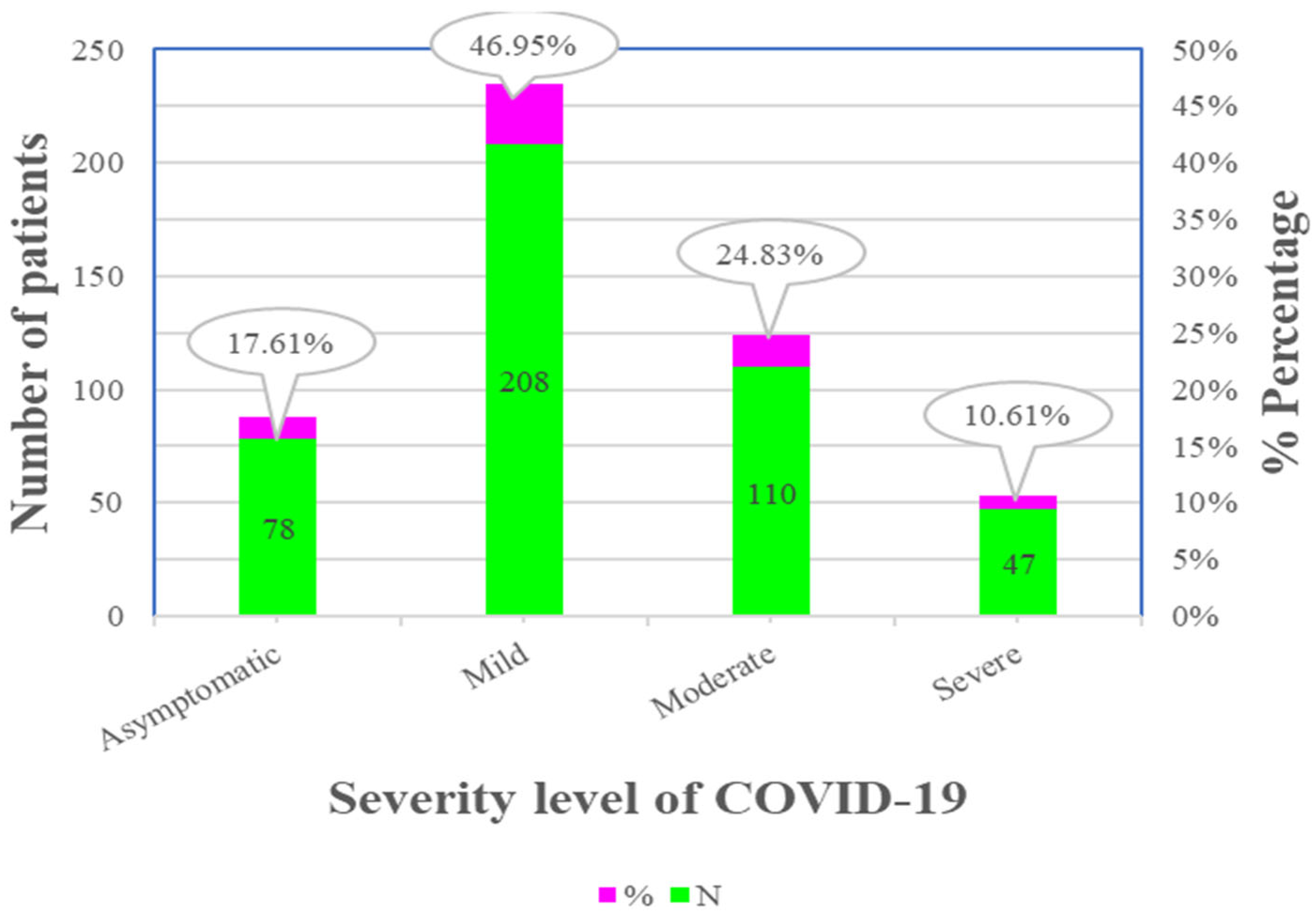
3.8. The Severity of COVID-19
3.9. Predictors of Severity and Duration of Hospital Stay (DoHS)
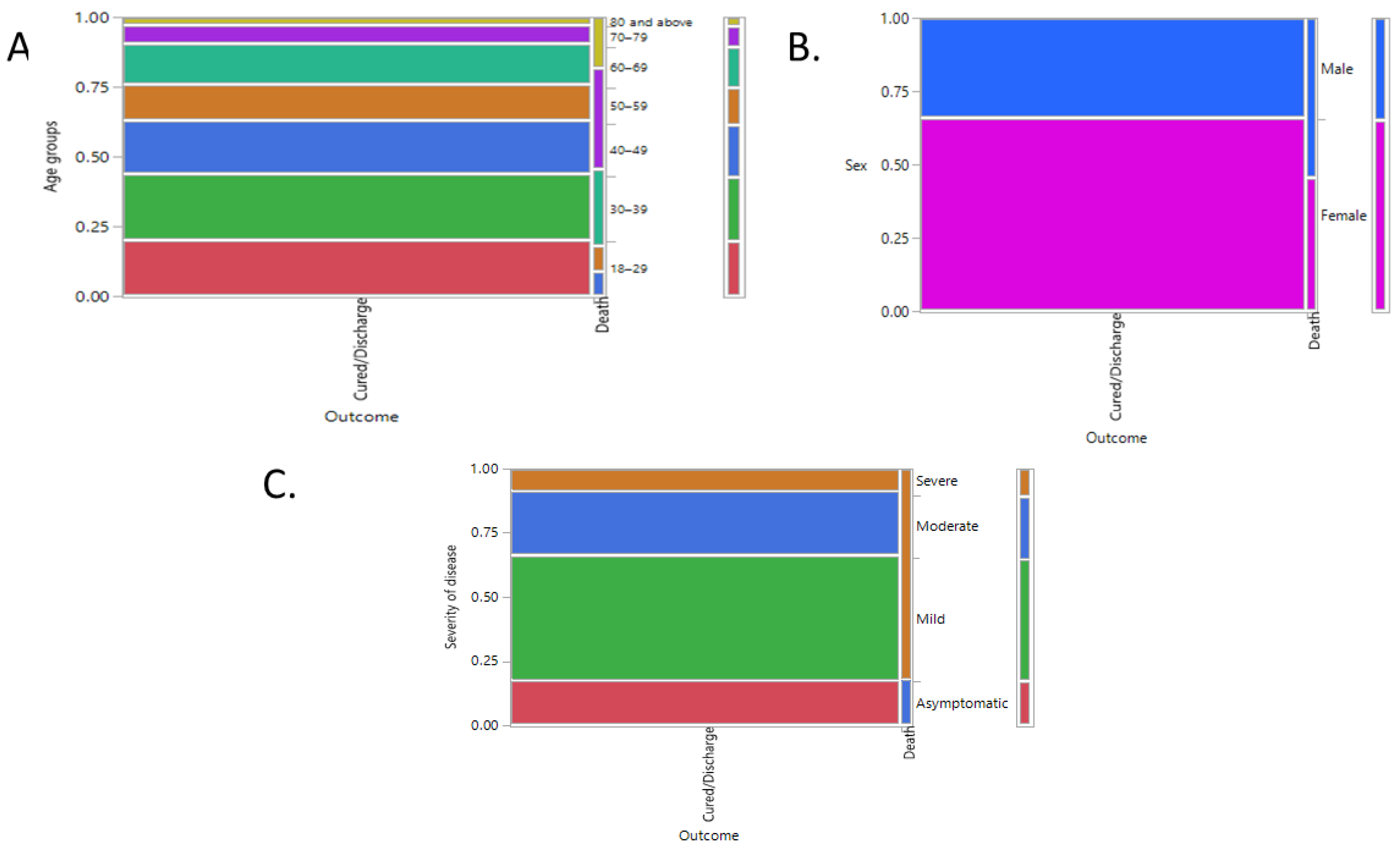
3.10. The Outcome of COVID-19 Patients with Severity Level, Age, and Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Alhazzani, W.; Alshahrani, M.; Alshamsi, F.; Aljuhani, O.; Eljaaly, K.; Hashim, S.; Alqahtani, R.; Alsaleh, D.; Al Duhailib, Z.; Algethamy, H.; et al. The Saudi Critical Care Society practice guidelines on the management of COVID-19 in the ICU: Therapy section. J. Infect. Public Health 2022, 15, 142–151. [Google Scholar] [CrossRef]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef] [PubMed]
- The Government of Saudi Arabia, Riyadh. Key Health Indicators 2021; MOH Publications: Riyadh, Saudi Arabia, 2021.
- Qureshi, A.Z.; Ullah, S.; Ullah, R. The trend of hospital accreditation in the Kingdom of Saudi Arabia. Saudi Med. J. 2012, 33, 1350–1351. [Google Scholar] [PubMed]
- Joint Commission International: Chicago, IL, USA. 2023. Available online: http://www.jointcommissioninternational.org/JCI-Accredited-Organizations/ (accessed on 15 February 2023).
- The Government of Saudi Arabia, Riyadh. The Kingdom of Saudi Arabia’s Experience in Health Preparedness and Response to COVID-19 Pandemic; MOH Publications: Riyadh, Saudi Arabia, 2020.
- Khan, A.; Alsofayan, Y.; Alahmari, A.; Alowais, J.; Algwizani, A.; Alserehi, H.; Assiri, A.; Jokhdar, H. COVID-19 in Saudi Arabia: The national health response. East. Mediterr. Health J. 2021, 27, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2020; Available online: https://covid19.who.int/ (accessed on 15 February 2023).
- Ibrahim, M.E.; Al-Aklobi, O.S.; Abomughaid, M.M.; Al-Ghamdi, M.A. Epidemiological, clinical, and laboratory findings for patients of different age groups with confirmed coronavirus disease 2019 (COVID-19) in a hospital in Saudi Arabia. PLoS ONE 2021, 16, e0250955. [Google Scholar] [CrossRef]
- Chen, R.; Chen, J.; Meng, Q.-T. Chest computed tomography images of early coronavirus disease (COVID-19). Can. J. Anaesth. J. Can. D’anesthésie 2020, 67, 754–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.; Zhang, X.; Qu, J. Coronavirus disease 2019 (COVID-19): A clinical update. Front. Med. 2020, 14, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Aljondi, R.; Alghamdi, S.; Tajaldeen, A.; Abdelaziz, I.; Bushara, L.; Alghamdi, H.A.; Alhinishi, H.; Alharbi, B.; Alshehri, R.; Aljehani, A.; et al. Chest Radiological Findings and Clinical Characteristics of Laboratory-Confirmed COVID-19 Patients from Saudi Arabia. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e932441. [Google Scholar] [CrossRef]
- Zeng, H.; Ma, Y.; Zhou, Z.; Liu, W.; Huang, P.; Jiang, M.; Liu, Q.; Chen, P.; Luo, H.; Chen, Y. Spectrum and Clinical Characteristics of Symptomatic and Asymptomatic Coronavirus Disease 2019 (COVID-19) With and Without Pneumonia. Front. Med. 2021, 8, 645651. [Google Scholar] [CrossRef] [PubMed]
- Bairwa, M.; Kumar, R.; Beniwal, K.; Kalita, D.; Bahurupi, Y. Hematological profile and biochemical markers of COVID-19 non-survivors: A retrospective analysis. Clin. Epidemiol. Glob. Health 2021, 11, 100770. [Google Scholar] [CrossRef]
- Ghaith, M.M.; Albanghali, M.A.; Aldairi, A.F.; Iqbal, M.S.; Almaimani, R.A.; AlQuthami, K.; Alqasmi, M.H.; Almaimani, W.; El-Readi, M.Z.; Alghamdi, A.; et al. Potential Predictors of Poor Prognosis among Severe COVID-19 Patients: A Single-Center Study. Can. J. Infect. Dis. Med. Microbiol. J. Can. Des. Mal. Infect. Microbiol. Med. 2021, 2021, 6656092. [Google Scholar] [CrossRef] [PubMed]
- Kantri, A.; Ziati, J.; Khalis, M.; Haoudar, A.; El Aidaoui, K.; Daoudi, Y.; Chikhaoui, I.; El Yamani, K.; Mouhaoui, M.; El Bakkouri, J.; et al. Hematological and biochemical abnormalities associated with severe forms of COVID-19: A retrospective single-center study from Morocco. PLoS ONE 2021, 16, e0246295. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MOH. COVID-19 Statistics E-Platform. Available online: https://covid19.moh.gov.sa/ (accessed on 15 February 2023).
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Ling, Y.; Bai, T.; Xie, Y.; Huang, J.; Li, J.; Xiong, W.; Yang, D.; Chen, R.; Lu, F.; et al. COVID-19 with Different Severities: A Multicenter Study of Clinical Features. Am. J. Respir. Crit. Care Med. 2020, 201, 1380–1388. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Gao, X.; Yang, D.; Yuan, Z.; Zhang, Y.; Li, H.; Gao, P.; Liu, X.; Zhao, W.; Xiao, T.; Guan, Y.; et al. Improving the early diagnosis of suspected patients with COVID-19: A retrospective study of 106 patients. J. Infect. Dev. Ctries. 2020, 14, 547–553. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Shao, J.; Guo, Y.; Peng, X.; Li, Z.; Hu, D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr. Pulmonol. 2020, 55, 1169–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Channappanavar, R.; Fett, C.; Mack, M.; Ten Eyck, P.P.; Meyerholz, D.K.; Perlman, S. Sex-Based Differences in Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Infection. J. Immunol. 2017, 198, 4046–4053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Lake, M.A. What we know so far: COVID-19 current clinical knowledge and research. Clin. Med. 2020, 20, 124–127. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbadage, T.; Peterson, B.M.; Awada, J.; Buck, A.S.; Ramirez, D.A.; Wilson, J.; Gunasekera, R.S. Systematic Review and Meta-Analysis of Sex-Specific COVID-19 Clinical Outcomes. Front. Med. 2020, 7, 348. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Strope, J.D.; Chau, C.H.; Figg, W.D. Are sex discordant outcomes in COVID-19 related to sex hormones? Semin. Oncol. 2020, 47, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Ortona, E.; Pierdominici, M.; Rider, V. Editorial: Sex Hormones and Gender Differences in Immune Responses. Front. Immunol. 2019, 10, 1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Yu, X.; Zhao, H.; Wang, H.; Zhao, R.; Sheng, J. Host susceptibility to severe COVID-19 and establishment of a host risk score: Findings of 487 cases outside Wuhan. Crit. Care 2020, 24, 108. [Google Scholar] [CrossRef] [Green Version]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health TMIH 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Luzi, L.; Radaelli, M.G. Influenza and obesity: Its odd relationship and the lessons for COVID-19 pandemic. Acta Diabetol. 2020, 57, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Weir, E.K.; Thenappan, T.; Bhargava, M.; Chen, Y. Does vitamin D deficiency increase the severity of COVID-19? Clin. Med. 2020, 20, e107–e108. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2021, 93, 733–740. [Google Scholar] [CrossRef]
- Singh, S.K.; Jain, R.; Singh, S. Vitamin D deficiency in patients with diabetes and COVID-19 infection. Diabetes Metab. Syndr. 2020, 14, 1033–1035. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; The Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Jain, V.; Yuan, J.M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Alwafi, H.; Naser, A.Y.; Qanash, S.; Brinji, A.S.; Ghazawi, M.A.; Alotaibi, B.; Alghamdi, A.; Alrhmani, A.; Fatehaldin, R.; Alelyani, A.; et al. Predictors of Length of Hospital Stay, Mortality, and Outcomes Among Hospitalised COVID-19 Patients in Saudi Arabia: A Cross-Sectional Study. J. Multidiscip. Healthc. 2021, 14, 839–852. [Google Scholar] [CrossRef]
- Alghamdi, S. Clinical characteristics and treatment outcomes of severe (ICU) COVID-19 patients in Saudi Arabia: A single centre study. Saudi Pharm. J. SPJ Off. Publ. Saudi Pharm. Soc. 2021, 29, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, Y.; Wei, L.; Ji, J.S.; Liu, Y.; Liu, R.; Zha, Y.; Chang, X.; Zhang, L.; Liu, Q.; et al. What are the risk factors of hospital length of stay in the novel coronavirus pneumonia (COVID-19) patients? A survival analysis in southwest China. PLoS ONE 2022, 17, e0261216. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.; Chun, B.C. An interim review of the epidemiological characteristics of 2019 novel coronavirus. Epidemiol. Health 2020, 42, e2020006. [Google Scholar] [CrossRef] [Green Version]
- Alboaneen, D.; Pranggono, B.; Alshammari, D.; Alqahtani, N.; Alyaffer, R. Predicting the Epidemiological Outbreak of the Coronavirus Disease 2019 (COVID-19) in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 4568. [Google Scholar] [CrossRef]
- Abolfotouh, M.A.; Musattat, A.; Alanazi, M.; Alghnam, S.; Bosaeed, M. Clinical characteristics and outcome of COVID-19 illness and predictors of in-hospital mortality in Saudi Arabia. BMC Infect. Dis. 2022, 22, 950. [Google Scholar] [CrossRef] [PubMed]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: A meta-analysis of 59 studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef] [PubMed]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, D.; Dai, X.; Ni, Y.; Xu, X. Change of serum uric acid and progression of cardiometabolic multimorbidity among middle aged and older adults: A prospective cohort study. Front. Public Health 2022, 10, 1012223. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, W.; Wang, Y.; Xiong, Y.; Chen, S.; Han, J.; Wu, Q. A comparative overview of COVID-19, MERS and SARS: Review article. Int. J. Surg. 2020, 81, 1–8. [Google Scholar] [CrossRef]
- Longo, M.; Caruso, P.; Maiorino, M.I.; Bellastella, G.; Giugliano, D.; Esposito, K. Treating type 2 diabetes in COVID-19 patients: The potential benefits of injective therapies. Cardiovasc. Diabetol. 2020, 19, 115. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.Q.; Peng, H.J. Characteristics of and Public Health Responses to the Coronavirus Disease 2019 Outbreak in China. J. Clin. Med. 2020, 9, 575. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Yang, L.; Li, Y.; Liang, B.; Li, L.; Ye, T.; Li, L.; Liu, D.; Gui, S.; Hu, Y.; et al. Factors associated with death outcome in patients with severe coronavirus disease-19 (COVID-19): A case-control study. Int. J. Med. Sci. 2020, 17, 1281–1292. [Google Scholar] [CrossRef]
- Yan, Y.; Yang, Y.; Wang, F.; Ren, H.; Zhang, S.; Shi, X.; Yu, X.; Dong, K. Clinical characteristics and outcomes of patients with severe COVID-19 with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001343. [Google Scholar] [CrossRef]
- Ferrando, C.; Mellado-Artigas, R.; Gea, A.; Arruti, E.; Aldecoa, C.; Bordell, A.; Adalia, R.; Zattera, L.; Ramasco, F.; Monedero, P.; et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: A prospective, cohort, multicentre study. Rev. Esp. Anestesiol. Reanim. 2020, 67, 425–437. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asymptomatic | Mild COVID-19 | Moderate COVID-19 | Severe COVID-19 | |
|---|---|---|---|---|
| Severe Cases | Critical Cases | |||
| COVID-19 PCR + ve, no symptoms | Symptoms (fever, cough, myalgia), RR < 24, SPo2 > 94% in room air, no pneumonia | Symptoms with shortness of breath, RR 24–30, SPo2 90–94 in room air, pneumonia | Pneumonia plus any one of the following: RR > 30, SPo2 < 90 in room air, severe respiratory distress, requiring respiratory support | ARDS, respiratory failure requiring ventilation support, sepsis, septic shock, MODS |
| Clinical Characteristics | N | Percentage |
|---|---|---|
| Fever | 247 | 55.76% |
| Cough | 236 | 53.27% |
| Dyspnea | 168 | 37.92% |
| Headache | 99 | 22.35% |
| Nausea/Vomiting | 76 | 17.16% |
| Myalgia | 86 | 19.41% |
| Diarrhea | 90 | 20.32% |
| Ageusia | 28 | 6.32% |
| Abdominal pain | 36 | 8.13% |
| Arthralgia | 11 | 2.48% |
| Anosmia | 15 | 3.39% |
| Symptoms | Age Groups (Years) | Sex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80 and Above | p-Value | Female % | Male % | p-Value | |
| Fever | <0.0001 **** | 0.0103 * | |||||||||
| Yes | 8.80% | 9.03% | 11.51% | 9.03% | 10.38% | 4.97% | 2.03% | 51.38% | 64.05% | ||
| No | 11.06% | 14.00% | 7.45% | 3.84% | 4.29% | 2.48% | 1.13% | 48.62% | 35.95% | ||
| Cough | <0.0001 **** | 0.3679 | |||||||||
| Yes | 8.35% | 8.35% | 10.84% | 9.48% | 9.48% | 4.97% | 1.81% | 51.72% | 56.21% | ||
| No | 11.51% | 14.67% | 8.13% | 3.39% | 5.19% | 2.48% | 1.35% | 48.28% | 43.79% | ||
| Dyspnea | <0.0001 **** | 0.4136 | |||||||||
| Yes | 3.61% | 6.09% | 7.45% | 7.45% | 8.80% | 3.16% | 1.35% | 36.55% | 40.52% | ||
| No | 16.25% | 16.93% | 11.51% | 5.42% | 5.87% | 4.29% | 1.81% | 63.45% | 59.48% | ||
| Headache | 0.09 | 0.1329 | |||||||||
| Yes | 6.09% | 5.42% | 3.39% | 3.16% | 3.39% | 0.68% | 0.23% | 24.48% | 18.30% | ||
| No | 13.77% | 17.61% | 15.58% | 9.71% | 11.29% | 6.77% | 2.93% | 75.52% | 81.70% | ||
| Nausea/Vomiting | 0.058 | 0.8424 | |||||||||
| Yes | 3.61% | 2.48% | 3.84% | 2.93% | 3.61% | 0.45% | 0.23% | 16.90% | 17.65% | ||
| No | 16.25% | 20.54% | 15.12% | 9.93% | 11.06% | 7.00% | 2.93% | 83.10% | 82.35% | ||
| Myalgia | 0.438 | 0.2299 | |||||||||
| Yes | 2.48% | 4.06% | 4.06% | 3.39% | 3.39% | 1.58% | 0.45% | 21.03% | 16.34% | ||
| No | 17.38% | 18.96% | 14.90% | 9.48% | 11.29% | 5.87% | 2.71% | 78.97% | 83.66% | ||
| Diarrhoea | 0.180 | 0.9834 | |||||||||
| Yes | 4.06% | 3.16% | 5.64% | 3.16% | 2.71% | 1.13% | 0.45% | 20.34% | 20.26% | ||
| No | 15.80% | 19.86% | 13.32% | 9.71% | 11.96% | 6.32% | 2.71% | 79.66% | 79.74% | ||
| Ageusia | 0.006 ** | 0.3459 | |||||||||
| Yes | 1.58% | 2.26% | 2.03% | 0.23% | 0.00% | 0.23% | 0.00% | 5.52% | 7.84% | ||
| No | 18.28% | 20.77% | 16.93% | 12.64% | 14.67% | 7.22% | 3.16% | 94.48% | 92.16% | ||
| Abdominal pain | 0.025 * | 0.0937 | |||||||||
| Yes | 2.48% | 1.81% | 2.03% | 0.00% | 1.13% | 0.23% | 0.45% | 9.66% | 5.23% | ||
| No | 17.38% | 21.22% | 16.93% | 12.87% | 13.54% | 7.22% | 2.71% | 90.34% | 94.77% | ||
| Anosmia | 0.212 | 0.5056 | |||||||||
| Yes | 0.45% | 1.58% | 0.90% | 0.23% | 0.23% | 0.00% | 0.00% | 3.79% | 2.61% | ||
| No | 19.41% | 21.44% | 18.06% | 12.64% | 14.45% | 7.45% | 3.16% | 96.21% | 97.39% | ||
| Arthralgia | 0.550 | 0.1697 | |||||||||
| Yes | 0.45% | 0.90% | 0.23% | 0.23% | 0.68% | 0.00% | 0.00% | 1.72% | 3.92% | ||
| No | 19.41% | 22.12% | 18.74% | 12.64% | 14.00% | 7.45% | 3.16% | 98.28% | 96.08% | ||
| Co-Morbidities | Age Groups (Years) | Sex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80 and Above | p-Value | Female % | Male % | p-Value | |
| Diabetes | <0.0001 **** | ||||||||||
| Yes | 1.13% | 1.81% | 4.51% | 5.64% | 7.67% | 4.74% | 2.03% | 25.17% | 32.03% | 0.1272 | |
| No | 18.74% | 21.22% | 14.45% | 7.22% | 7.00% | 2.71% | 1.13% | 74.83% | 67.97% | ||
| Hypertension | <0.0001 **** | 0.0119 * | |||||||||
| Yes | 0.68% | 0.68% | 4.29% | 4.51% | 8.80% | 5.42% | 2.26% | 22.76% | 33.99% | ||
| No | 19.19% | 22.35% | 14.67% | 8.35% | 5.87% | 2.03% | 0.90% | 77.24% | 66.01% | ||
| Asthma and any other respiratory disorders | 0.1663 | 0.3063 | |||||||||
| Yes | 2.48% | 4.97% | 2.71% | 1.35% | 1.35% | 0.45% | 0.68% | 12.76% | 16.34% | ||
| No | 17.38% | 18.06% | 16.25% | 11.51% | 13.32% | 7.00% | 2.48% | 87.24% | 83.66% | ||
| Obesity | 0.102 | 0.0467 * | |||||||||
| Yes | 6.55% | 10.16% | 9.26% | 7.45% | 8.13% | 4.06% | 0.68% | 52.76% | 33.99% | ||
| No | 13.32% | 12.87% | 9.71% | 5.42% | 6.55% | 3.39% | 2.48% | 47.24% | 66.01% | ||
| CVD | <0.0001 **** | 0.0467 * | |||||||||
| Yes | 0.00% | 0.45% | 1.13% | 1.13% | 2.48% | 2.26% | 0.68% | 6.21% | 11.76% | ||
| No | 19.86% | 22.57% | 17.83% | 11.74% | 12.19% | 5.19% | 2.48% | 93.79% | 88.24% | ||
| Renal disease | 0.6263 | 0.1933 | |||||||||
| Yes | 0.45% | 0.23% | 0.23% | 0.45% | 0.45% | 0.00% | 0.23% | 1.38% | 3.27% | ||
| No | 19.41% | 22.80% | 18.74% | 12.42% | 14.22% | 7.45% | 2.93% | 98.62% | 96.73% | ||
| Stroke | 0.2038 | 0.3252 | |||||||||
| Yes | 0.23% | 0.00% | 0.00% | 0.23% | 0.45% | 0.23% | 0.23% | 1.72% | 0.65% | ||
| No | 19.64% | 23.02% | 18.96% | 12.64% | 14.22% | 7.22% | 2.93% | 98.28% | 99.35% | ||
| Vitamin D deficiency | 0.2782 | 0.0235 * | |||||||||
| Yes | 0.23% | 0.45% | 0.00% | 0.00% | 0.23% | 0.45% | 0.00% | 2.07% | 0.00% | ||
| No | 19.64% | 22.57% | 18.96% | 12.87% | 14.45% | 7.00% | 3.16% | 97.93% | 100.00% | ||
| Hematological disorders | 0.7098 | 0.3623 | |||||||||
| Yes | 1.13% | 0.45% | 0.45% | 0.45% | 0.23% | 0.23% | 0.00% | 3.45% | 1.96% | ||
| No | 18.74% | 22.57% | 18.51% | 12.42% | 14.45% | 7.22% | 3.16% | 96.55% | 98.04% | ||
| Hypothyroidism | 0.0481 * | 0.0448 * | |||||||||
| Yes | 0.45% | 1.81% | 2.48% | 1.58% | 2.03% | 0.23% | 0.23% | 10.69% | 5.23% | ||
| No | 19.41% | 21.22% | 16.48% | 11.29% | 12.64% | 7.22% | 2.93% | 89.31% | 94.77% | ||
| Hyperthyroidism | 0.7658 | 0.357 | |||||||||
| Yes | 0.00% | 0.00% | 0.23% | 0.00% | 0.00% | 0.00% | 0.00% | 0.34% | 0.00% | ||
| No | 19.86% | 23.02% | 18.74% | 12.87% | 14.67% | 7.45% | 3.16% | 99.66% | 100.00% | ||
| Parameters | Age Groups (Years) | Sex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80 and Above | p-Value | Female % | Male % | p-Value | |
| Required O2 on arrival | <0.0001 **** | 0.0081 * | |||||||||
| Yes | 1.13% | 1.35% | 4.06% | 2.71% | 4.97% | 2.48% | 1.35% | 14.48% | 24.84% | ||
| No | 18.74% | 21.67% | 14.90% | 10.16% | 9.71% | 4.97% | 1.81% | 85.52% | 75.16% | ||
| Systemic IV steroids | <0.0001 **** | 0.0294 * | |||||||||
| Yes | 1.35% | 3.39% | 4.97% | 4.74% | 6.32% | 3.16% | 1.81% | 22.41% | 32.03% | ||
| No | 18.51% | 19.64% | 14.00% | 8.13% | 8.35% | 4.29% | 1.35% | 77.59% | 67.97% | ||
| Transferred to ICU | <0.0001 **** | 0.0417 * | |||||||||
| Yes | 0.90% | 0.90% | 3.39% | 2.26% | 3.61% | 2.48% | 0.68% | 11.72% | 18.95% | ||
| No | 18.96% | 22.12% | 15.58% | 10.61% | 11.06% | 4.97% | 2.48% | 88.28% | 81.05% | ||
| Required intubation | 0.0024 ** | 0.0609 | |||||||||
| Yes | 0.00% | 0.23% | 0.90% | 0.68% | 1.13% | 1.13% | 0.00% | 2.76% | 6.58% | ||
| No | 19.91% | 22.85% | 17.87% | 12.22% | 13.57% | 6.33% | 3.17% | 97.24% | 93.42% | ||
| Home isolation | 2.26% | 3.61% | 3.16% | 0.23% | 0.68% | 0.45% | 0.00% | 0.0037 ** | 11.38% | 8.50% | 0.3373 |
| A | |||
|---|---|---|---|
| Clinical Parameters | Severity of Disease | ||
| Mild % | Severe % | p-Value | |
| I. Symptoms | |||
| Fever | 45.1 | 75.16 | <0.0001 **** |
| Cough | 41.26 | 75.16 | <0.0001 **** |
| Dyspnea | 24.83 | 61.78 | <0.0001 **** |
| Headache | 24.48 | 18.47 | 0.1424 |
| Nausea/Vomiting | 15.73 | 19.75 | 0.2879 |
| Myalgia | 17.83 | 22.29 | 0.2597 |
| Diarrhea | 17.13 | 26.11 | 0.0264 * |
| Ageusia | 8.39 | 2.55 | 0.0096 ** |
| Abdominal pain | 9.09 | 6.37 | 0.3075 |
| Arthralgia | 3.15 | 1.27 | 0.2016 |
| Anosmia | 3.5 | 3.18 | 0.8616 |
| II. Co-morbidities | |||
| Diabetes | 21.51 | 40.4 | <0.0001 **** |
| Hypertension | 45.22 | 54.78 | <0.0001 **** |
| Asthma and any other RS disorders | 12.54 | 16.56 | 0.2567 |
| Obesity | 44.8 | 50.33 | 0.2729 |
| Cardiovascular disease (MI, CHF, others) | 3.94 | 15.23 | <0.0001 **** |
| Renal disease | 2.15 | 1.99 | 0.9095 |
| Cancer/leukemia | 0.00% | 0.00% | |
| Stroke | 1.08 | 1.99 | 0.4523 |
| Vitamin D deficiency | 1.79 | 0.66 | 0.3114 |
| Hematological disorders | 3.58 | 0.66 | 0.067 |
| Hypothyroidism | 7.53 | 10.6 | 0.2851 |
| Hyperthyroidism | 0.36 | 0.00% | 0.352 |
| B | |||
| Mild | Severe | p-Value | |
| I. Age Groups (Years) | |||
| 18–29 | 27.27% (78) | 6.37% (10) | <0.0001 **** |
| 30–39 | 29.37% (84) | 11.46% (18) | |
| 40–49 | 16.78% (48) | 22.93% (46) | |
| 50–59 | 10.49% (30) | 17.20% (27) | |
| 60–69 | 9.79% (28) | 23.57% (37) | |
| 70–79 | 5.24% (15) | 11.46% (18) | |
| 80 and Above | 1.05% (3) | 7.01% (11) | |
| II. Gender | |||
| Female | 70.98% | 55.41% | 0.0011 ** |
| Male | 29.02% | 44.59% | |
| C | |||
| Parameters | Severity of Disease | ||
| Mild % | Severe % | p-Value | |
| Home isolation | 12.59 | 6.37 | 0.0336 * |
| Required O2 on arrival | 3.5 | 44.59 | <0.0001 **** |
| Transferred to ICU | 0.7 | 38.85 | <0.0001 **** |
| Required intubation | 0.35 | 10.9 | <0.0001 **** |
| Chest X-ray: pneumonia | 23.78 | 92.99 | <0.0001 **** |
| Systemic IV steroids | 11.89 | 50.96 | <0.0001 **** |
| Systemic oral steroids | 22.93 | 6.64 | <0.0001 **** |
| Level1 | Level2 | Odds Ratio | Lower 95% | Upper 95% | Prob > Chisq | |
|---|---|---|---|---|---|---|
| Sex | Male | Female | 1.49 | 0.74 | 2.98 | 0.26 |
| Required O2 on arrival | Yes | No | 7.89 | 2.64 | 23.60 | 0.0002 *** |
| Transferred to ICU | Yes | No | 26.01 | 3.52 | 192.32 | 0.0014 ** |
| Diabetes | Yes | No | 0.88 | 0.39 | 1.96 | 0.75 |
| Hypertension | Yes | No | 0.79 | 0.33 | 1.86 | 0.58 |
| Asthma and any other respiratory disorders | Yes | No | 2.40 | 0.95 | 6.06 | 0.06 |
| CVD (MI, CHF, others) | Yes | No | 3.37 | 1.04 | 10.89 | 0.0425 * |
| Renal disease | Yes | No | 0.14 | 0.01 | 4.13 | 0.26 |
| Stroke | Yes | No | 20.52 | 1.29 | 326.53 | 0.0324 * |
| Hematological disorders | Yes | No | 0.21 | 0.01 | 5.62 | 0.35 |
| Hypothyroidism | Yes | No | 1.15 | 0.37 | 3.56 | 0.80 |
| Hyperthyroidism | Yes | No | 0.00 | 0.00 | 1.00 | |
| Chest X-ray: Pneumonia | Yes | No | 27.90 | 11.63 | 66.96 | <0.0001 **** |
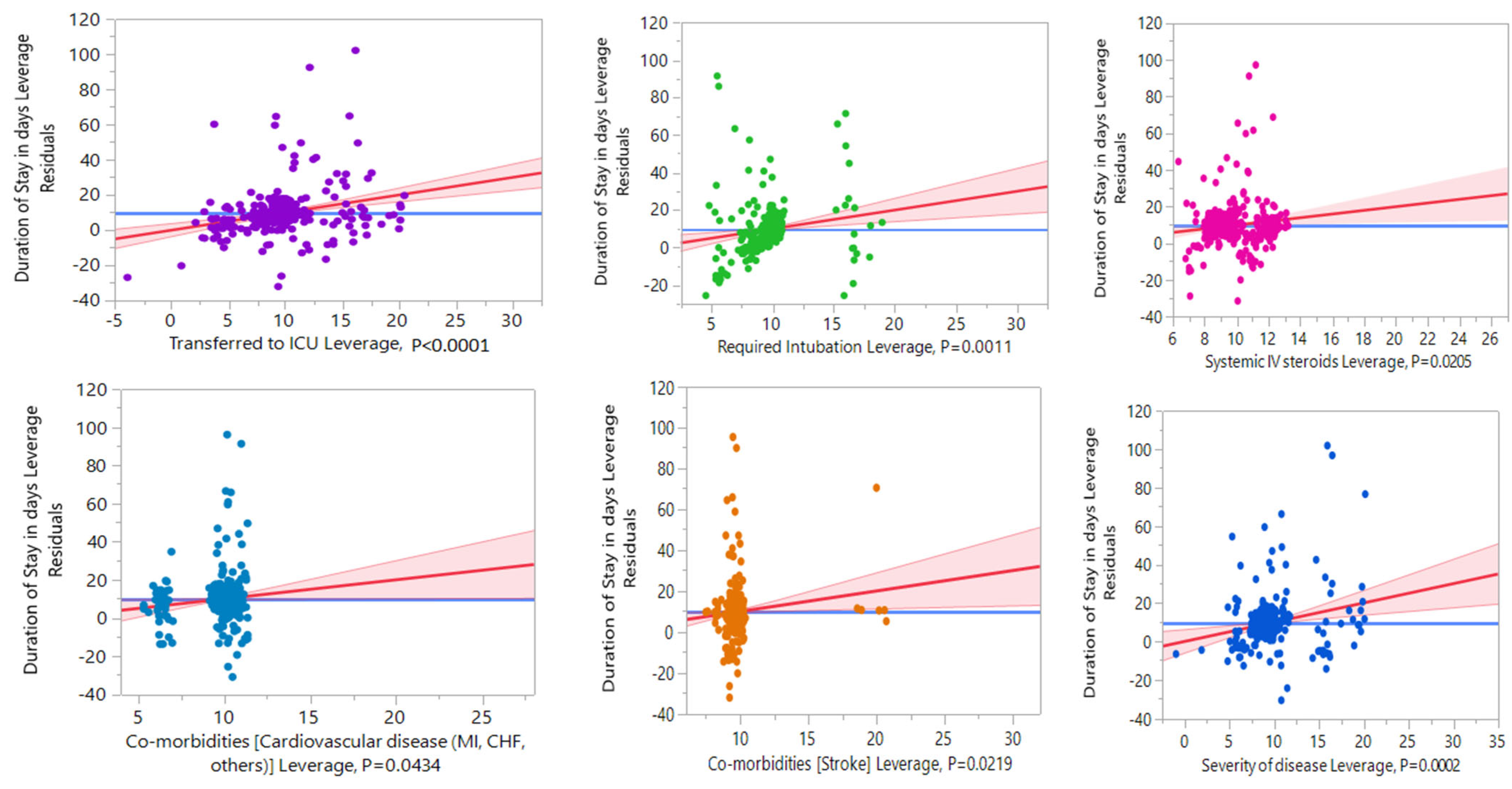
| Duration of Hospital Stay | Standard Least Squares Method Estimates | |||||
|---|---|---|---|---|---|---|
| Term | Mean | Std ERROR | Estimate | Std Error | t Ratio | Prob > |t| |
| Duration of hospital stay (days): maximum = 118, minimum = 1, mean = 9.72 ± 14.2 (SD), median = 6 | ||||||
| Intercept | 24.493488 | 7.154958 | 3.42 | 0.0007 *** | ||
| Systemic IV steroids | ||||||
| No | 6.5915 | 7.1781791 | −1.756811 | 0.755274 | −2.33 | 0.0205 * |
| Yes | 18.7281 | 7.2112043 | Reference | |||
| Transferred to ICU | ||||||
| No | 6.4316 | 7.2047820 | −6.417144 | 1.196474 | −5.36 | <0.0001 **** |
| Yes | 29.8871 | 7.3034964 | Reference | |||
| Required intubation | ||||||
| No | 8.3420 | 7.1128093 | −5.656731 | 1.717231 | −3.29 | 0.0011 ** |
| Yes | 42.2222 | 7.5955612 | Reference | |||
| Cardiovascular disease (MI, CHF, others) | ||||||
| No | 9.5074 | 7.0680036 | 2.1945388 | 1.082989 | 2.03 | 0.0434 * |
| Yes | 12.1389 | 7.4010742 | Reference | |||
| Stroke | ||||||
| No | 9.5092 | 6.9696932 | −5.621868 | 2.442903 | −2.30 | 0.0219 * |
| Yes | 25.1667 | 8.1083768 | Reference | |||
| Severity of disease | ||||||
| Asymptomatic | 5.5385 | 7.4129636 | −3.295884 | 1.507726 | −2.19 | 0.0294 * |
| Mild | 5.5577 | 7.2660448 | −3.364786 | 1.06918 | −3.15 | 0.0018 ** |
| Moderate | 11.2455 | 7.2969359 | −1.7349 | 1.191134 | −1.46 | 0.1460 |
| Severe | 32.0000 | 7.2273743 | Reference | |||
| Outcome | 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80 and Above | Total | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Cured and discharged | 85 | 99 | 80 | 55 | 60 | 28 | 12 | 419 | 0.0013 ** |
| 100% | 100% | 98.77% | 98.21% | 95.24% | 87.50% | 85.71% | |||
| Death | 0 | 0 | 1 | 1 | 3 | 4 | 2 | 11 | |
| 0% | 0% | 1.23% | 1.79% | 4.76% | 12.50% | 14.29% | |||
| Total | 85 | 99 | 81 | 56 | 63 | 32 | 14 | 430 |
| Parameters | Main Results of Current Study | Results of Previous Studies | New Contributions/Important Highlights of Current Study | |
|---|---|---|---|---|
| Clinical characteristics | Fever | Most frequent symptoms | Similar results seen [30,31,32,33] | Statistically more commonly in older patients of age groups 60–69 years, 70–79 years, and 80 years old and more compared to younger groups. |
| Cough | ||||
| Dyspnea | ||||
| Ageusia | Other symptoms found | Nonspecific symptoms | Statistically higher in younger age groups than in older patients. | |
| Abdominal pain | ||||
| Co-morbidities | Diabetes | Most frequent co-morbidities | Diabetes and HTN were the most common co-morbid conditions [22,39] | a. More 60–69 years older patients had statistically higher HTN, DM, CHF, and hypothyroidism. b. Diabetes and HTN were common in ages 70–79 years, 50–59 years, and 40–49 years. In contrast, asthma and other respiratory disorders were comparatively higher in the younger age group of 30–39 years. c. More males suffered HTN and cardiovascular disease, while obesity, hypothyroidism, and vitamin D deficiencies were comparatively higher in females. |
| Hypertension | ||||
| Asthma/respiratory disorders | ||||
| Predictors of severity | Pneumonia on chest X-ray | Statistically significant differences found for pneumonia, CVD, stroke, ICU, and mechanical ventilation | Older age, male sex, and presence of co-morbidities associated with severe disease at admission [22] | a. The age groups of 70–79 years and 60–69 years required intubation, which was statistically significant compared to younger patients. b. A higher percentage of males were given oxygen support on arrival and treated with systemic steroids. c. Age groups 70–79 years and 80 and above were significantly associated with in-hospital mortality. d. Nearly 55.67% of “70–79 years” and the majority of “80 and above” were suffering severe disease at the time of admission, and nearly 15% of each group succumbed to the disease. |
| Co-morbid conditions such as CVD, stroke | ||||
| ICU stay | ||||
| Mechanical ventilation | ||||
| Length of hospital stay | The median period of hospital stay was six days | Similar results seen [49] | It was significantly longer in patients with severe disease who needed oxygen support or mechanical ventilation, as expected, and also longer in patients with CVD or stroke and administered systemic intravenous steroids. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assiri, R.A.; Bepari, A.; Patel, W.; Hussain, S.A.; Niazi, S.K.; Alshangiti, A.; Alshangiti, S.A.; Cordero, M.A.W.; Sheereen, S. Exploration of Sex and Age-Based Associations in Clinical Characteristics, Predictors of Severity, and Duration of Stay among COVID-19 Patients at the University Hospital of Saudi Arabia. Healthcare 2023, 11, 751. https://doi.org/10.3390/healthcare11050751
Assiri RA, Bepari A, Patel W, Hussain SA, Niazi SK, Alshangiti A, Alshangiti SA, Cordero MAW, Sheereen S. Exploration of Sex and Age-Based Associations in Clinical Characteristics, Predictors of Severity, and Duration of Stay among COVID-19 Patients at the University Hospital of Saudi Arabia. Healthcare. 2023; 11(5):751. https://doi.org/10.3390/healthcare11050751
Chicago/Turabian StyleAssiri, Rasha Assad, Asmatanzeem Bepari, Waseemoddin Patel, Syed Arif Hussain, Shaik Kalimulla Niazi, Asma Alshangiti, Safia Ali Alshangiti, Mary Anne Wong Cordero, and Shazima Sheereen. 2023. "Exploration of Sex and Age-Based Associations in Clinical Characteristics, Predictors of Severity, and Duration of Stay among COVID-19 Patients at the University Hospital of Saudi Arabia" Healthcare 11, no. 5: 751. https://doi.org/10.3390/healthcare11050751