
Prevalence of Symptomatic Knee Osteoarthritis in Saudi Arabia and Associated Modifiable and Non-Modifiable Risk Factors: A Population-Based Cross-Sectional Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
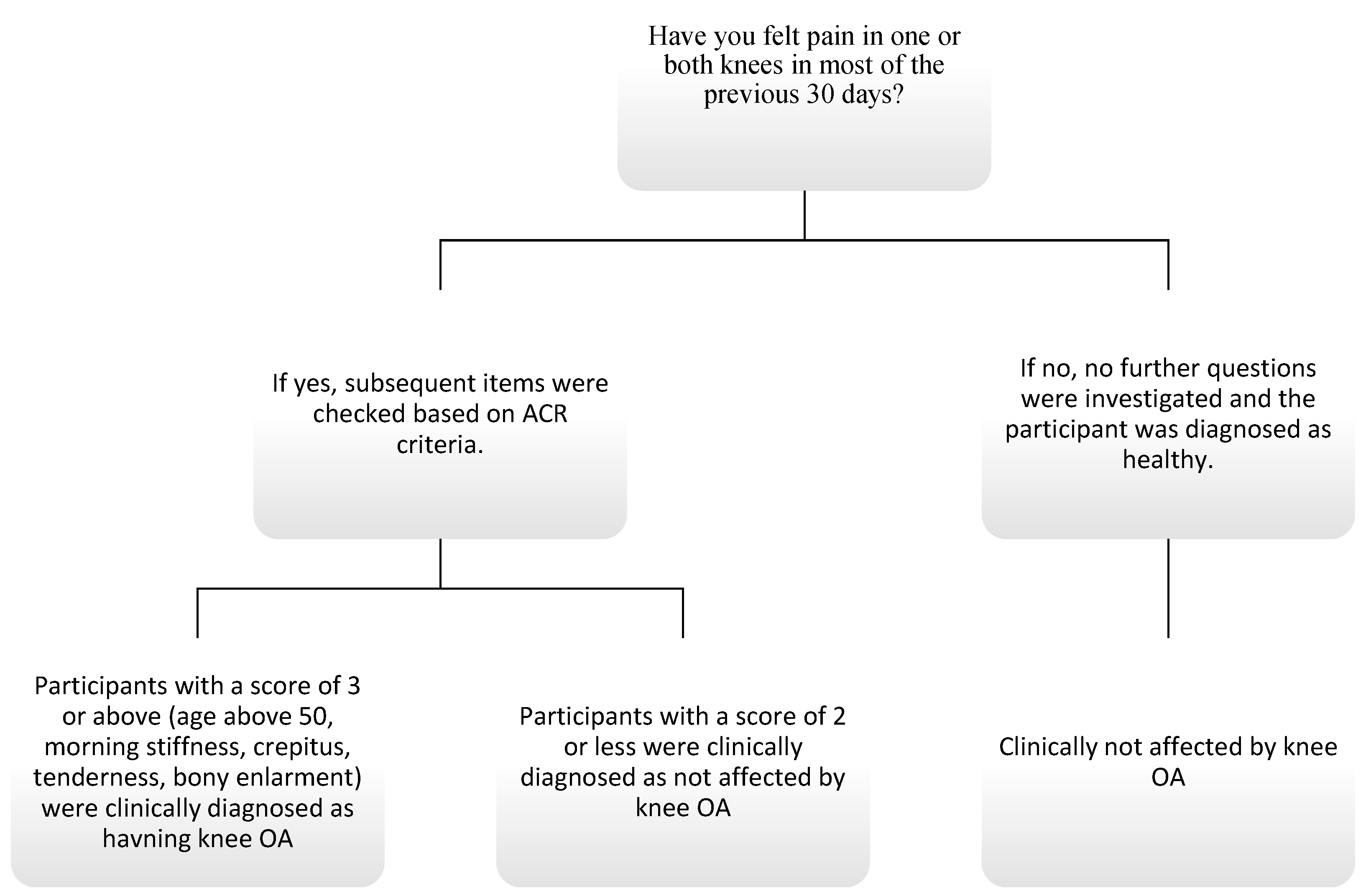
2.2. American College of Rheumatology (ACR) Knee OA Assessment Criteria
2.3. Implementation of the Assessment Criteria
2.4. KOOS Scale
2.5. Scoring to Diagnose Individuals with Knee OA
2.6. Data Collection
2.7. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Arfaj, A.S.; Al-Boukai, A.A. Prevalence of radiographic knee osteoarthritis in Saudi Arabia. Clin. Rheumatol. 2002, 21, 142–145. [Google Scholar] [CrossRef]
- O’Neill, T.W.; Felson, D.T. Mechanisms of Osteoarthritis (OA) Pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Georgiev, T.; Angelov, A.K. Modifiable risk factors in knee osteoarthritis: Treatment implications. Rheumatol. Int. 2019, 39, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Vongsirinavarat, M.; Nilmart, P.; Somprasong, S.; Apinonkul, B. Identification of knee osteoarthritis disability phenotypes regarding activity limitation: A cluster analysis. BMC Musculoskelet. Disord. 2020, 21, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominick, K.L.; Ahern, F.M.; Gold, C.H.; Heller, D.A. Health-related quality of life and health service use among older adults with osteoarthritis. Arthritis Care Res. 2004, 51, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.C. Osteoarthritis of the Knee; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Bindawas, S.M.; Vennu, V.; Alfhadel, S.; Al-Otaibi, A.D.; Binnasser, A.S. Knee pain and health-related quality of life among older patients with different knee osteoarthritis severity in Saudi Arabia. PLoS ONE 2018, 13, e0196150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Arfaj, A.S.; Alballa, S.R.; Al-Saleh, S.S.; Al-Dalaan, A.M.; Bahabry, S.A.; Mousa, M.A.; Al-Sekeit, M.A. Knee osteoarthritis in Al-Qaseem, Saudi Arabia. Saudi Med. J. 2003, 24, 291–293. [Google Scholar]
- Alrowaili, M.G. Magnetic resonance evaluation of knee osteoarthritis among the Saudi Population. Pak. J. Med Sci. 2019, 35, 1575–1581. [Google Scholar] [CrossRef]
- Ahlberg, A.; Linder, B.; Binhemd, T.A. Osteoarthritis of the hip and knee in Saudi Arabia. Int. Orthop. 1990, 14, 29–30. Available online: http://link.springer.com/article/10.1007/BF00183360 (accessed on 1 December 2022). [CrossRef]
- Javaid, M.K.; Kiran, A.; Guermazi, A.; Kwoh, C.K.; Zaim, S.; Carbone, L.; Harris, T.; McCulloch, C.E.; Arden, N.K.; Lane, N.E.; et al. Individual magnetic resonance imaging and radiographic features of knee osteoarthritis in subjects with unilateral knee pain: The health, aging, and body composition study. Arthritis Rheum. 2012, 64, 3246–3255. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Osteoarthritis: Care and management clinical guideline [CG177]. In Musculoskeletal Conditions; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29, 100587. [Google Scholar] [CrossRef] [PubMed]
- Alenazi, A.M.; Alhowimel, A.S.; Alotaibi, M.A.; Alqahtani, B.A.; Alshehri, M.M.; Alanazi, A.D.; Alanazi, A.A.; Alanazi, S.F.; Bindawas, S.M. Prevalence and incidence of osteoarthritis among people living in the Gulf Cooperation Council countries: A systematic review and meta-analysis. Clin. Rheumatol. 2021, 40, 3523–3531. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.B.; Blanco, F.J.; Englund, M.; Karsdal, M.A.; Lohmander, L.S. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthr. Cartil. 2015, 23, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, B. Knee osteoarthritis diagnosis, treatment and associated factors of progression: Part II. Casp. J. Intern. Med. 2011, 2, 249–255. [Google Scholar]
- Almangoush, A.; Herrington, L.; Attia, I.; Jones, R.; Aldawoudy, A.; Aziz, A.A.; Waley, A. Cross-cultural adaptation, reliability, internal consistency and validation of the Arabic version of the Knee injury and Osteoarthritis Outcome Score (KOOS) for Egyptian people with knee injuries. Osteoarthr. Cartil. 2013, 21, 1855–1864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS). Arthritis Care Res. 2011, 63, S208–S228. [Google Scholar] [CrossRef] [Green Version]
- Anuurad, E.; Shiwaku, K.; Nogi, A.; Kitajima, K.; Enkhmaa, B.; Shimono, K.; Yamane, Y. The new BMI criteria for asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J. Occup. Health 2003, 45, 335–343. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Araujo, A.D.; Junqueira, I.D.A.; Oliveira, D.; Brasileiro, A.; Arcanjo, F.L. Comparative study of functional capacity and quality of life among obese and non-obese elderly people with knee osteoarthritis. Rev. Bras. Reumatol. 2016, 56, 126–130. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.W.; Noh, J.H.; Kim, D.J. The prevalence of and demographic factors associated with radiographic knee osteoarthritis in Korean adults aged ≥ 50 years: The 2010-2013 Korea National Health and Nutrition Examination Survey. PLoS ONE 2020, 15, e0230613. [Google Scholar] [CrossRef] [PubMed]
- Heidari, B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Casp. J. Intern. Med. 2011, 2, 205–212. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24024017 (accessed on 3 October 2018).
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.L.; Protheroe, J.; Jordan, K.P. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil 2015, 23, 507–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, S.C.; Valdes, A.M. The Genetics of Osteoarthritis: A Review. J. Funct. Morphol. Kinesiol. 2016, 1, 140–153. [Google Scholar] [CrossRef] [Green Version]
- Snoeker, B.; Turkiewicz, A.; Magnusson, K.; Frobell, R.; Yu, D.; Peat, G.; Englund, M. Risk of knee osteoarthritis after different types of knee injuries in young adults: A population-based cohort study. Br. J. Sports Med. 2020, 54, 725–730. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.; Wang, L.; Meng, F.; Cao, J.; Shen, Y. Association between smoking and risk of knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2017, 25, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Han, K.; Park, Y.G.; Park, S.H. Effects of education, income, and occupation on prevalence and symptoms of knee osteoarthritis. Sci. Rep. 2021, 11, 13983. [Google Scholar] [CrossRef]
- Anderson, A.S.; Loeser, R.F. Why is osteoarthritis an age-related disease? Best Pract. Res. Clin. Rheumatol. 2010, 24, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar]
- Hame, S.L.; Alexander, R.A. Knee osteoarthritis in women. Curr. Rev. Musculoskelet. Med. 2013, 6, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Tian, W.; Wang, Y.; Rong, J.; Bao, C.; Liu, Y.; Zhao, Y.; Wang, C. Body mass index and susceptibility to knee osteoarthritis: A systematic review and meta-analysis. Jt. Bone Spine 2012, 79, 291–297. [Google Scholar] [CrossRef]
- Thigah, A.; Khan, A. Prevalence of Knee Osteoarthritis among Adult Patients Attending Al-iskan Primary Health Care Center. Ann. Clin. Anal. Med. 2020, 9, 272–278. [Google Scholar]
- AlQarni, S.S.M. A Review of Prevalence of Obesity in Saudi Arabia. J. Obes. Eat Disord. 2016, 2, 1–6. [Google Scholar] [CrossRef]
- Bliddal, H.; Leeds, A.R.; Christensen, R. Osteoarthritis, obesity and weight loss: Evidence, hypotheses and horizons—A scoping review. Obes. Rev. 2014, 15, 578–586. [Google Scholar] [CrossRef] [Green Version]
- Iijima, H.; Ohi, H.; Isho, T.; Aoyama, T.; Fukutani, N.; Kaneda, E.; Ohi, K.; Abe, K.; Kuroki, H.; Matsuda, S. Association of bilateral flat feet with knee pain and disability in patients with knee osteoarthritis: A cross-sectional study. J. Orthop. Res. 2017, 35, 2490–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, K.D.; Felson, D.T.; Niu, J.; Hunter, D.J.; Guermazi, A.; Roemer, F.W.; Dufour, A.B.; Gensure, R.H.; Hannan, M.T. Flat Feet Are Associated with Knee Pain and Cartilage Damage in Older Adults NIH Public Access. Arthritis Care Res 2011, 63, 937–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfadhel, S.A.; Vennu, V.; Alnahdi, A.H.; Omar, M.T.; Alasmari, S.H.; AlJafri, Z.; Bindawas, S.M. Cross-cultural adaptation and validation of the Saudi Arabic version of the Knee Injury and Osteoarthritis Outcome Score (KOOS). Rheumatol. Int. 2018, 38, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L.; Woodhouse, L.J.; Nettel-Aguirre, A.; Emery, C.A. Outcomes associated with early post-traumatic osteoarthritis and other negative health consequences 3–10 years following knee joint injury in youth sport. Osteoarthr. Cartil. 2015, 23, 1122–1129. [Google Scholar] [CrossRef] [Green Version]
- Kraus, V.B.; Sprow, K.; Powell, K.E.; Buchner, D.; Bloodgood, B.; Piercy, K.; George, S.M.; Kraus, W.E. Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1324–1339. [Google Scholar] [CrossRef]
- Srikanth, V.K.; Fryer, J.L.; Zhai, G.; Winzenberg, T.M.; Hosmer, D.; Jones, G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthr. Cartil. 2005, 13, 769–781. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.; Moisio, K.; Chmiel, J.; Eckstein, F.; Guermazi, A.; Prasad, P.; Zhang, Y.; Almagor, O.; Belisle, L.; Hayes, K.; et al. External knee adduction and flexion moments during gait and medial tibiofemoral disease progression in knee osteoarthritis. Osteoarthr Cartil. 2015, 23, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radzimski, A.O.; Mündermann, A.; Sole, G. Effect of footwear on the external knee adduction moment—A systematic review. Knee 2012, 19, 163–175. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Number (%) |
|---|---|
| Gender | |
| Male | 431 (19.12) |
| Female | 1823 (80.88) |
| Marital status | |
| Married | 1369 (60.74) |
| Single | 885 (39.26) |
| BMI (kg/m2) | |
| Underweight | 118 (5.24) |
| Normal | 802 (35.58) |
| Overweight | 646 (28.66) |
| Obese | 688 (30.52) |
| Education | |
| Illiterate | 13 (0.58) |
| Primary | 26 (1.15) |
| Intermediate | 60 (2.66) |
| High school | 422 (18.72) |
| Diploma | 224 (9.94) |
| Bachelor’s degree | 1353 (60.03) |
| Master’s/Ph.D. (higher degree) | 156 (6.92) |
| Type of work | |
| Unemployed | 610 (27.06) |
| Office work | 663 (29.41) |
| Fieldwork | 464 (20.59) |
| Mixed (office and field) | 112 (4.97) |
| Retired | 97 (4.30) |
| Housewife | 308 (13.66) |
| Smoking | |
| Smoker | 2101 (93.21) |
| Non-smoker | 153 (6.79) |
| Level of physical activity | |
| Inactive | 1098 (48.71) |
| Low intensity (e.g., walking), requiring low effort | 925 (41.04) |
| Moderate intensity (e.g., jogging), requiring moderate effort | 149 (6.61) |
| High intensity (e.g., running), requiring high effort | 82 (3.64) |
| Age (years) | |
| 18–30 | 997 (44.23) |
| 31–49 | 855 (37.93) |
| ≥50 | 402 (17.83) |
| Variable | Number (%) |
|---|---|
| Diagnosis of knee OA according to our study criteria | |
| No | 1829 (81.14) |
| Yes | 425 (18.86) |
| Duration of knee pain (years) | |
| No pain | 992 (44.01) |
| <1 | 510 (22.63) |
| 1–5 | 478 (21.21) |
| 6–10 | 149 (6.61) |
| 11–15 | 56 (2.48) |
| >15 | 69 (3.06) |
| Affected knee with pain | |
| No | 992 (44.01) |
| Right side | 432 (19.17) |
| Left side | 358 (15.88) |
| Bilateral | 472 (20.94) |
| Previous knee injury | |
| No | 2020 (89.62) |
| Yes | 234 (10.38) |
| Flat feet | |
| No | 1773 (78.66) |
| Yes | 154 (6.83) |
| I do not know | 327 (14.51) |
| Sick leave in previous 12 months due to knee pain (days) | |
| No pain | 992 (44.01) |
| No sick leave | 1016 (45.08) |
| 1–5 | 145 (6.43) |
| 6–10 | 35 (1.55) |
| 11–15 | 7 (0.31) |
| >15 | 59 (2.62) |
| Family history of OA | |
| No | 463 (20.54) |
| Yes | 1437 (63.75) |
| I do not know | 354 (15.71) |
| Variables | Non-OA | OA | p-Value * |
|---|---|---|---|
| n (%) | n (%) | ||
| Gender | <0.01 | ||
| Male | 375 (87.01) | 56 (12.99) | |
| Female | 1454 (79.75) | 369 (20.25) | |
| Age (years) | <0.01 | ||
| 18–30 | 929 (93.18) | 68 (6.82) | |
| 31–49 | 682 (79.77) | 173 (20.23) | |
| ≥50 | 218 (54.23) | 184 (45.77) | |
| BMI | <0.01 | ||
| Underweight | 112 (94.92) | 6 (5.08) | |
| Normal | 722 (90.02) | 80 (9.98) | |
| Overweight | 543 (84.06) | 103 (15.94) | |
| Obese | 452 (65.70) | 236 (34.30) | |
| Previous knee injury (ACL, meniscus) | <0.01 | ||
| No | 1711 (84.70) | 309 (15.30) | |
| Yes | 118 (50.43) | 116 (49.57) | |
| Family history of OA | <0.01 | ||
| No | 410 (88.60) | 53 (11.40) | |
| Yes | 1117 (77.70) | 320 (22.30) | |
| I do not know | 302 (85.30) | 52 (14.70) | |
| Smoking | 0.012 | ||
| Non-smoker | 1693 (80.58) | 408 (19.42) | |
| Smoker | 136 (88.89) | 17 (11.11) | |
| Marital status | |||
| Married | 1019 (74.43) | 350 (25.57) | <0.01 |
| Single | 810 (91.53) | 75 (8.47) | |
| Flat feet | |||
| No | 1471 (82.97) | 302 (17.03) | <0.01 |
| Yes | 105 (68.2) | 49 (31.82) | |
| I do not know | 253 (77.37) | 74 (22.63) | |
| Level of physical activity | |||
| Inactive | 882 (80.33) | 216 (19.67) | <0.01 |
| Low intensity | 738 (79.78) | 187 (20.22) | |
| Moderate intensity | 141 (94.63) | 8 (5.37) | |
| High intensity | 68 (82.93) | 14 (17.07) | |
| Education | <0.01 | ||
| Illiterate | 2 (15.38) | 11(84.62) | |
| Primary | 10 (38.46) | 16 (61.54) | |
| Intermediate | 39 (65.00) | 21 (35.00) | |
| High school | 343 (81.28) | 79 (18.72) | |
| Diploma | 176 (78.57) | 48 (21.43) | |
| Bachelor’s degree | 1126 (83.22) | 227 (16.78) | |
| Master’s/Ph.D. (higher degree) | 133 (85.26) | 23 (14.74) | |
| Variable | B | S.E. | p-Value | OR | 95% C.I. | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Gender (female) | 0.76 | 0.19 | <0.01 | 2.14 | 1.48 | 3.11 |
| Age | 0.06 | 0.01 | <0.01 | 1.06 | 1.05 | 1.07 |
| BMI | 0.07 | 0.01 | <0.01 | 1.07 | 1.04 | 1.09 |
| Smoker (yes) | −0.67 | 0.32 | 0.04 | 0.51 | 0.27 | 0.96 |
| Previous injury to knee (ACL, meniscus) (yes) | 1.37 | 0.17 | <0.01 | 3.95 | 2.81 | 5.56 |
| Education level (illiterate) | Reference | |||||
| Primary | −0.57 | 0.91 | 0.53 | 0.57 | 0.10 | 3.36 |
| Secondary | −1.21 | 0.87 | 0.17 | 0.30 | 0.05 | 1.65 |
| High school | −1.37 | 0.82 | 0.10 | 0.25 | 0.05 | 1.27 |
| Diploma | −1.68 | 0.83 | 0.04 | 0.19 | 0.04 | 0.94 |
| Bachelor’s degree | −1.66 | 0.81 | 0.04 | 0.19 | 0.04 | 0.93 |
| Master’s/Ph.D. (higher degree) | −2.11 | 0.85 | 0.01 | 0.12 | 0.02 | 0.64 |
| Family history of OA (no) | Reference | |||||
| Yes | 0.49 | 0.18 | 0.01 | 1.63 | 1.15 | 2.32 |
| I do not know | 0.32 | 0.24 | 0.18 | 1.37 | 0.86 | 2.20 |
| Level of physical activity (no) | Reference | |||||
| Low intensity | −0.08 | 0.13 | 0.53 | 0.92 | 0.72 | 1.19 |
| Moderate intensity | −1.15 | 0.40 | 0.00 | 0.32 | 0.14 | 0.70 |
| High intensity | 0.90 | 0.34 | 0.01 | 2.47 | 1.28 | 4.77 |
| Constant | −5.11 | 0.94 | 0.00 | 0.01 | ||
| KOOS | Diagnosis | Number | Mean ± SD | p-Value between Non-OA and OA | Effect Size | p-Value between Non-OA with Knee Pain and OA | Effect Size |
|---|---|---|---|---|---|---|---|
| Pain | Non-OA * | 1829 | 88.40 ± 14.55 | <0.01 | <0.01 | ||
| Knee pain without OA ** | 837 | 79.99 ± 15.37 | 1.96 | 1.32 | |||
| Knee OA *** | 425 | 58.24 ± 18.32 | |||||
| Symptoms | Non-OA | 1829 | 80.91 ± 13.56 | <0.01 | <0.01 | ||
| Knee pain without OA | 837 | 78.04 ± 13.32 | 1.81 | 1.58 | |||
| Knee OA | 425 | 55.29 ± 16.28 | |||||
| ADL | Non-OA | 1829 | 89.58 ± 14.41 | <0.01 | <0.01 | ||
| Knee pain without OA | 838 | 83.48 ± 15.93 | 1.97 | 1.42 | |||
| Knee OA | 425 | 58.74 ± 20.15 | |||||
| Sports | Non-OA | 1829 | 81.90 ± 22.73 | <0.01 | <0.01 | ||
| Knee pain without OA | 838 | 71.12 ± 25.01 | 1.86 | 1.29 | |||
| Knee OA | 425 | 38.61 ± 25.46 | |||||
| QOL | Non-OA | 1829 | 81.90 ± 20.66 | <0.01 | <0.01 | ||
| Knee pain without OA | 838 | 70.14 ± 21.35 | 1.68 | 1.08 | |||
| Knee OA | 425 | 46.75 ± 22.05 | |||||
| Total | Non-OA | 1829 | 84.54 ± 14.43 | <0.01 | <0.01 | ||
| Knee pain without OA | 837 | 76.55 ± 15.15 | 2.19 | 1.56 | |||
| Knee OA | 425 | 51.53 ± 17.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Althomali, O.W.; Amin, J.; Acar, T.; Shahanawaz, S.; Talal Abdulrahman, A.; Alnagar, D.K.; Almeshari, M.; Alzamil, Y.; Althomali, K.; Alshoweir, N.; et al. Prevalence of Symptomatic Knee Osteoarthritis in Saudi Arabia and Associated Modifiable and Non-Modifiable Risk Factors: A Population-Based Cross-Sectional Study. Healthcare 2023, 11, 728. https://doi.org/10.3390/healthcare11050728
Althomali OW, Amin J, Acar T, Shahanawaz S, Talal Abdulrahman A, Alnagar DK, Almeshari M, Alzamil Y, Althomali K, Alshoweir N, et al. Prevalence of Symptomatic Knee Osteoarthritis in Saudi Arabia and Associated Modifiable and Non-Modifiable Risk Factors: A Population-Based Cross-Sectional Study. Healthcare. 2023; 11(5):728. https://doi.org/10.3390/healthcare11050728
Chicago/Turabian StyleAlthomali, Omar W., Junaid Amin, Tolgahan Acar, Syed Shahanawaz, Alanazi Talal Abdulrahman, Dalia Kamal Alnagar, Meshari Almeshari, Yasser Alzamil, Kamal Althomali, Noorah Alshoweir, and et al. 2023. "Prevalence of Symptomatic Knee Osteoarthritis in Saudi Arabia and Associated Modifiable and Non-Modifiable Risk Factors: A Population-Based Cross-Sectional Study" Healthcare 11, no. 5: 728. https://doi.org/10.3390/healthcare11050728