
Time-to-Event Analysis of Factors Influencing Delay in Discharge from a Subacute Complex Discharge Unit during the First Year of the Pandemic (2020) in an Irish Tertiary Centre Hospital
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Data Sources
2.3. Statistical Analyses
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, H.; Hara, Y.; Horita, N.; Saigusa, Y.; Kaneko, T. An Early Screening Tool for Discharge Planning Shortened Length of Hospital Stay for Elderly Patients with Community-Acquired Pneumonia. Clin Interv. Aging 2021, 16, 443–450. [Google Scholar] [CrossRef]
- Activity in Acute Public Hospitals in Ireland 2020—HPO November 2021. Available online: http://hpo.ie/latest_hipe_nprs_reports/HIPE_2020/HIPE_Report_2020.pdf (accessed on 5 December 2022).
- Independent Expert Review of Delayed Discharges November 2018. Available online: https://assets.gov.ie/10858/b63d907d251d47d4a5a58ccbc0f280fc.pdf (accessed on 5 December 2022).
- Sezgin, D.; O’Caoimh, R.; O’Donovan, M.R.; Salem, M.A.; Kennelly, S.; Samaniego, L.L.; Carda, C.A.; Rodriguez-Acuña, R.; Inzitari, M.; Hammar, T.; et al. European Union Advantage Joint Action Work Package 7 partners in collaboration with the International Foundation for Integrated Care Special Interest Group on Intermediate Care. Defining the characteristics of intermediate care models including transitional care: An international Delphi study. Aging Clin. Exp. Res. 2020, 32, 2399–2410. [Google Scholar] [CrossRef] [PubMed]
- Rameli, P.M.; Rajendran, N. Outcomes of complex discharge planning in older adults with complex needs: A scoping review. J. Int. Med. Res. 2022, 50, 3000605221110511. [Google Scholar] [CrossRef] [PubMed]
- McGilton, K.S.; Vellani, S.; Krassikova, A.; Robertson, S.; Irwin, C.; Cumal, A.; Bethell, J.; Burr, E.; Keatings, M.; McKay, S.; et al. Understanding transitional care programs for older adults who experience delayed discharge: A scoping review. BMC Geriatr. 2021, 21, 210. [Google Scholar] [CrossRef] [PubMed]
- NHS England Statistics. Monthly Delayed Transfer of Care Situation Reports: Definitions and Guidance. 2015. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/delayed-transfers-of-care/ (accessed on 5 December 2022).
- Rojas-García, A.; Turner, S.; Pizzo, E.; Hudson, E.; Thomas, J.; Raine, R. Impact and experiences of delayed discharge: A mixed- studies systematic review. Health Expect. 2018, 21, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.; Britt, H.; Miller, G.; Henderson, J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open 2014, 4, e004694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramdass, S.K.; Brennan, M.J.; Starr, R.; Lindenauer, P.K.; Liu, X.; Pekow, P.; Stefan, M.S. The Association of Frailty with Discharge Disposition for Hospitalized Community Dwelling Elderly Patients. J. Hosp. Med. 2018, 13, 182–184. [Google Scholar] [CrossRef] [Green Version]
- Wallace, E.; Salisbury, C.; Guthrie, B.; Lewis, C.; Fahey, T.; Smith, S.M. Managing patients with multimorbidity in primary care. BMJ 2015, 350, h176. [Google Scholar] [CrossRef] [Green Version]
- Challis, D.; Hughes, J.; Xie, C.; Jolley, D. An examination of factors influencing delayed discharge of older people from hospital. Int. J. Geriatr. Psychiatry 2014, 29, 160–168. [Google Scholar] [CrossRef]
- Rodríguez Reveggino, B.; Becerra-Bolaños, Á. Transitional Justice after the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 12388. [Google Scholar] [CrossRef]
- Frenkel, W.J.; Jongerius, E.J.; Mandjes-van Uitert, M.J.; van Munster, B.C.; de Rooij, S.E. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: A prospective cohort study. J. Am. Geriatr. Soc. 2014, 62, 342–346. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577, Erratum in Ann. Intern. Med. 2008, 148, 168. [Google Scholar] [CrossRef] [Green Version]
- NCPS. The impact of the Coronavirus Pandemic on Surgery in Ireland—September 2021. Available online: https://www.rcsi.com/dublin/news-and-events/news/news-article/2021/10/impact-of-covid-19-on-surgical-services-detailed-in-new-ncps-report (accessed on 5 December 2022).
- The Impact of COVID-19 on Outpatient Visits in 2020: Visits Remained Stavble, Despite a Late Surge in Cases. Available online: https://www.commonwealthfund.org/publications/2021/feb/impact-covid-19-outpatient-visits-2020-visits-stable-despite-late-surge (accessed on 5 December 2022).
- McDermott, A.; Kerr, G.; Browne, J. Association between clinical frailty scale score and length of stay in a complex discharge unit. Ir. Med. J. 2021, 114, 238. [Google Scholar]
- Fluck, D.; Fry, C.H.; Rankin, S.; Lewis, A.; Robin, J.; Rees, J.; Finch, J.; Jones, Y.; Jones, G.; Tudose, J.; et al. Does the length of stay in hospital affect healthcare outcomes of patients without COVID-19 who were admitted during the pandemic? A retrospective monocentric study. Intern. Emerg. Med. 2022, 17, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Mo, J.; Lim, Z.Y.; Lu, S.Y.; Low, S.G.; Xu, B.; Loo, Y.X.; Koh, C.W.; Kong, L.Y.; Towle, R.M.; et al. Impact of COVID-19 Measures on Discharge Planning and Continuity of Integrated Care in the Community for Older Patients in Singapore. Int. J. Integr. Care 2022, 22, 13. [Google Scholar] [CrossRef] [PubMed]
- Weerahandi, H.; Mak, W.; Burack, O.R.; Canter, B.E.; Reinhardt, J.P.; Boockvar, K.S. Discharge processes in a skilled nursing facility affected by COVID-19. J. Am. Geriatr. Soc. 2021, 69, 2437–2439. [Google Scholar] [CrossRef]
- Zisberg, A.; Zysberg, L.; Young, H.M.; Schepp, K.G. Trait routinization, functional and cognitive status in older adults. Int. J. Aging Hum. Dev. 2009, 69, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Curnow, E.; Tyagi, V.; Salisbury, L.; Stuart, K.; Melville-Jóhannesson, B.; Nicol, K.; McCormack, B.; Dewing, J.; Magowan, R.; Sagan, O.; et al. Person-centered healthcare practice in a pandemic context: An exploration of people’s experience of seeking healthcare support. Front. Rehabil. Sci. 2021, 2, 726210. [Google Scholar] [CrossRef]
- Rodrigues, L.P.; de Oliveira Rezende, A.T.; Delpino, F.M.; Mendonça, C.R.; Noll, M.; Nunes, B.P.; de Oliviera, C.; Silveira, E.A. Association between multimorbidity and hospitalization in older adults: Systematic review and meta-analysis. Age Ageing 2022, 51, afac155. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Chronic condition multimorbidity, AIHW, Australian Government. 2021. Available online: https://www.aihw.gov.au/reports/chronic-disease/chronic-condition-multimorbidity/related-material (accessed on 5 December 2022).
- Valderas, J.M.; Starfield, B.; Sibbald, B.; Salisbury, C.; Roland, M. Defining comorbidity: Implications for understanding health and health services. Ann. Fam. Med. 2009, 7, 357–363. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, J.; Zhao, J.; Tao, H.; Chi, J.; Niu, X.; Zhang, J.; Wang, Y. Menopause and frailty: A scoping review. Menopause 2020, 27, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 and Older People: Impact on Their Lives, Support and Care, Publications Office of the European Union, Luxembourg. Available online: https://www.eurofound.europa.eu/publications/report/2022/covid-19-and-older-people-impact-on-their-lives-support-and-care (accessed on 5 December 2022).
- Brief Update on COVID-19 Outbreaks and Hospital acquired cases in Acute Hospitals Author: Acute Operations HSE and AMRIC Lead. Available online: https://assets.gov.ie/126556/996860e1-2b03-4690-b69b-fedef14aadfe.pdf (accessed on 5 December 2022).



{kind=link}
{kind=link}
| 2020 (n = 390) | |||
|---|---|---|---|
| Patient Characteristics | LOS ≤ 15 days (n = 153) | LOS > 15 days (n = 237) | p <0.05 Statistical significance |
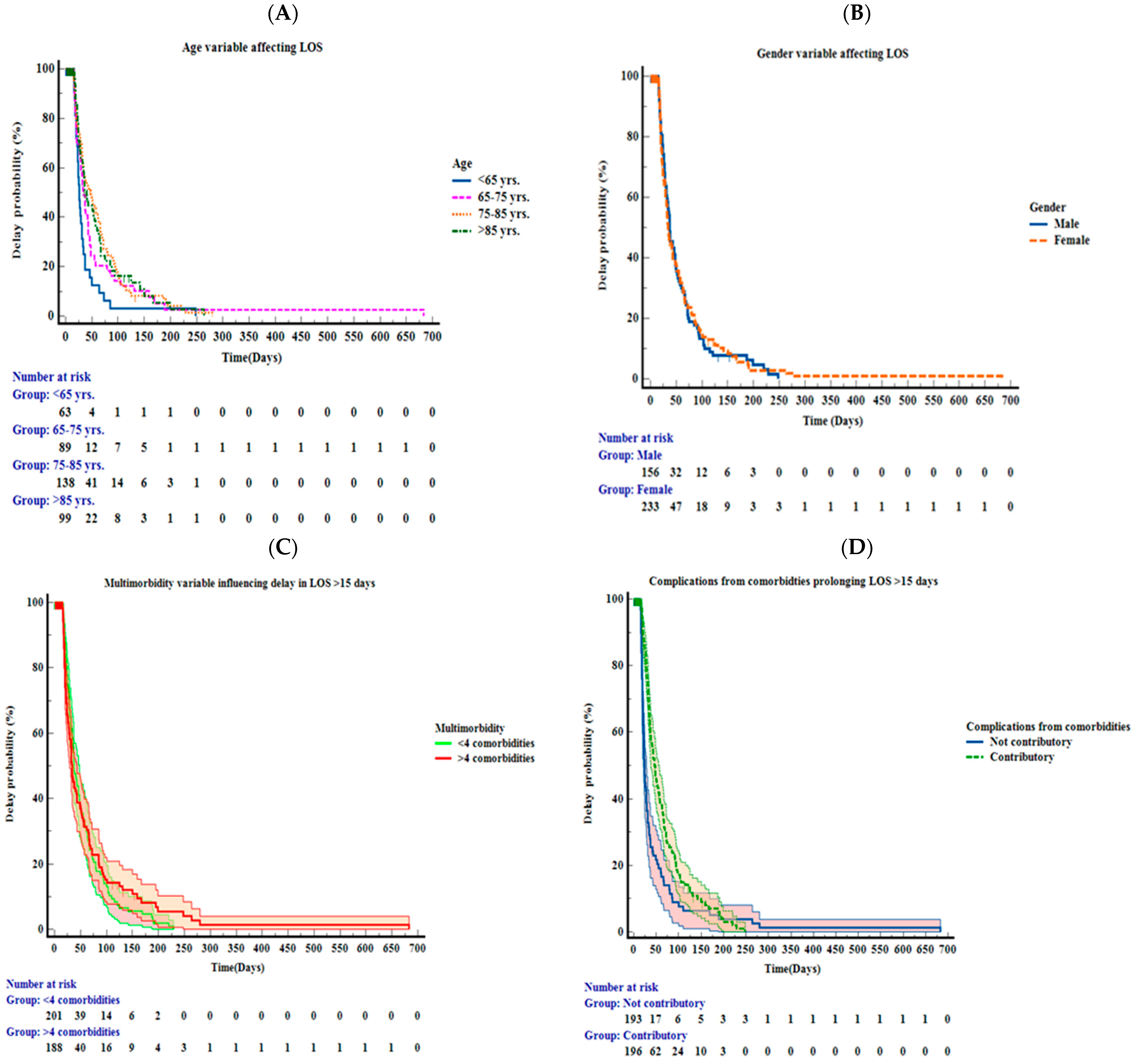
| Age (Mean ± SD) | 75.25 ± 12.50 | 77.51 ± 12.62 | p = 0.038 |
| Gender: Female Male | 62.09% 37.90% | 58.22% 41.77% | p = 0.51 (Yates correction to avoid type 1 error); p = 0.46 |
| Multimorbidity: ≤4 >4 | 15 64 | 99 124 | p < 0.05 |
| Chief Characteristics | Covariates | B Coefficient | Hazard Ratio (95% CI) | p Value | |
|---|---|---|---|---|---|
| Age | <65 | Complications/comorbidities prolonging LOS | −2.329 | 0.097 (0.028–0.340) | <0.001 |
| Healthcare-associated infection | −1.005 | 0.366 (0.095–1.416) | 0.146 | ||
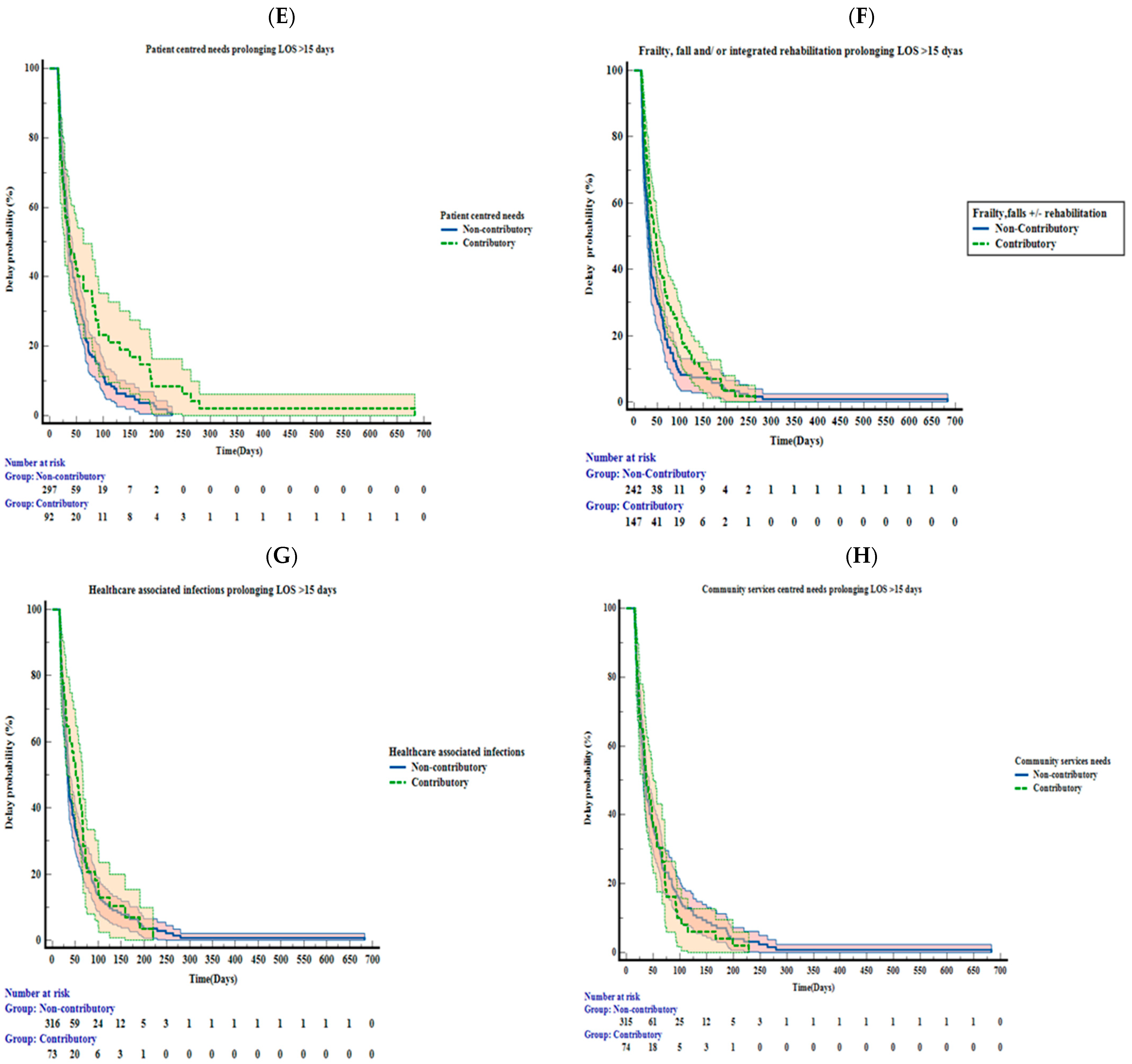
| Frailty, falls, and/or integrated rehabilitation needs | −0.063 | 0.939 (0.272–3.239) | 0.921 | ||
| Patient-centred needs | −0.039 | 0.962 (0.325–2.850) | 0.944 | ||
| Community services | −0.216 | 0.806 (0.321–2.020) | 0.645 | ||
| Age | 65–75 | Complications/comorbidities prolonging LOS | −0.759 | 0.468 (0.206–1.065) | 0.070 |
| Healthcare-associated infection | 0.190 | 1.209 (0.506–2.887) | 0.669 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.893 | 0.410 (0.211–0.795) | 0.008 | ||
| Patient-centred needs | −1.455 | 0.233 (0.077–0.708) | 0.010 | ||
| Community services | 0.67 | 1.069 (0.522–2.188) | 0.855 | ||
| Age | 75–85 | Complications/comorbidities prolonging LOS | −1.270 | 0.281 (0.160–0.492) | <0.001 |
| Healthcare-associated infection | −0.628 | 0.533 (0.288–0.987) | 0.045 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.473 | 0.623 (0.387–1.002) | 0.051 | ||
| Patient-centred needs | −1.199 | 0.301 (0.155–0.588) | <0.001 | ||
| Community services | −0.075 | 0.928 (0.536–1.605) | 0.789 | ||
| Age | >85 | Complications/comorbidities prolonging LOS | −0.619 | 0.539 (0.272–1.065) | 0.075 |
| Healthcare-associated infection | −0.177 | 0.838 (0.369–1.904) | 0.673 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.213 | 0.808 (0.427–1.531) | 0.514 | ||
| Patient-centred needs | −0.498 | 0.608 (0.262–1.408) | 0.246 | ||
| Community services | −0.203 | 0.817 (0.394–1.693) | 0.586 | ||
| Gender | Male | Complications/comorbidities prolonging LOS | −1.930 | 0.145 (0.081–0.261) | <0.001 |
| Healthcare-associated infection | −0.574 | 0.563 (0.314–1.010) | 0.054 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.235 | 0.790 (0.513–1.217) | 0.286 | ||
| Patient-centred needs | −0.751 | 0.472 (0.243–0.917) | 0.027 | ||
| Community services | −0.027 | 0.973 (0.621–1.524) | 0.905 | ||
| Gender | Female | Complications/comorbidities prolonging LOS | −0.736 | 0.479 (0.311–0.737) | <0.001 |
| Healthcare-associated infection | −0.157 | 0.854 (0.524–1.393) | 0.528 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.521 | 0.594 (0.401–0.880) | 0.009 | ||
| Patient-centred needs | −1.018 | 0.361 (0.215–0.608) | <0.001 | ||
| Community services | −0.073 | 0.930 (0.520–1.663) | 0.809 | ||
| Multi morbidity | ≤4 | Complications/comorbidities prolonging LOS | −0.858 | 0.424 (0.267–0.672) | <0.001 |
| Healthcare-associated infection | −0.351 | 0.704 (0.411–1.207) | 0.202 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.843 | 0.431 (0.285–0.651) | <0.001 | ||
| Patient-centred needs | −0.828 | 0.437 (0.247–0.772) | 0.004 | ||
| Community services | −0.234 | 0.792 (0.501–1.252) | 0.317 | ||
| Multi morbidity | >4 | Complications/comorbidities prolonging LOS | −1.179 | 0.308 (0.190–0.497) | <0.001 |
| Healthcare-associated infection | −0.086 | 0.917 (0.551–1.528) | 0.740 | ||
| Frailty, falls, and/or integrated rehabilitation needs | −0.256 | 0.774 (0.512–1.170) | 0.224 | ||
| Patient-centred needs | −1.045 | 0.352 (0.192–0.644) | <0.001 | ||
| Community services | 0.196 | 1.211 (0.739–2.002) | 0.442 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajendran, N.; Rameli, P.M.; Malomo, K.; Byrne, D.; Browne, J.; Ntlholang, O. Time-to-Event Analysis of Factors Influencing Delay in Discharge from a Subacute Complex Discharge Unit during the First Year of the Pandemic (2020) in an Irish Tertiary Centre Hospital. Healthcare 2023, 11, 627. https://doi.org/10.3390/healthcare11040627
Rajendran N, Rameli PM, Malomo K, Byrne D, Browne J, Ntlholang O. Time-to-Event Analysis of Factors Influencing Delay in Discharge from a Subacute Complex Discharge Unit during the First Year of the Pandemic (2020) in an Irish Tertiary Centre Hospital. Healthcare. 2023; 11(4):627. https://doi.org/10.3390/healthcare11040627
Chicago/Turabian StyleRajendran, Nithya, Puteri Maisarah Rameli, Keneilwe Malomo, Declan Byrne, Joseph Browne, and Ontefetse Ntlholang. 2023. "Time-to-Event Analysis of Factors Influencing Delay in Discharge from a Subacute Complex Discharge Unit during the First Year of the Pandemic (2020) in an Irish Tertiary Centre Hospital" Healthcare 11, no. 4: 627. https://doi.org/10.3390/healthcare11040627
{kind=link}