
Relationship between Isokinetic Trunk Muscle Strength and Return to Sports Competition after Conservative Therapy in Fresh Cases of Lumbar Spondylolysis: A Retrospective Observational Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Participants
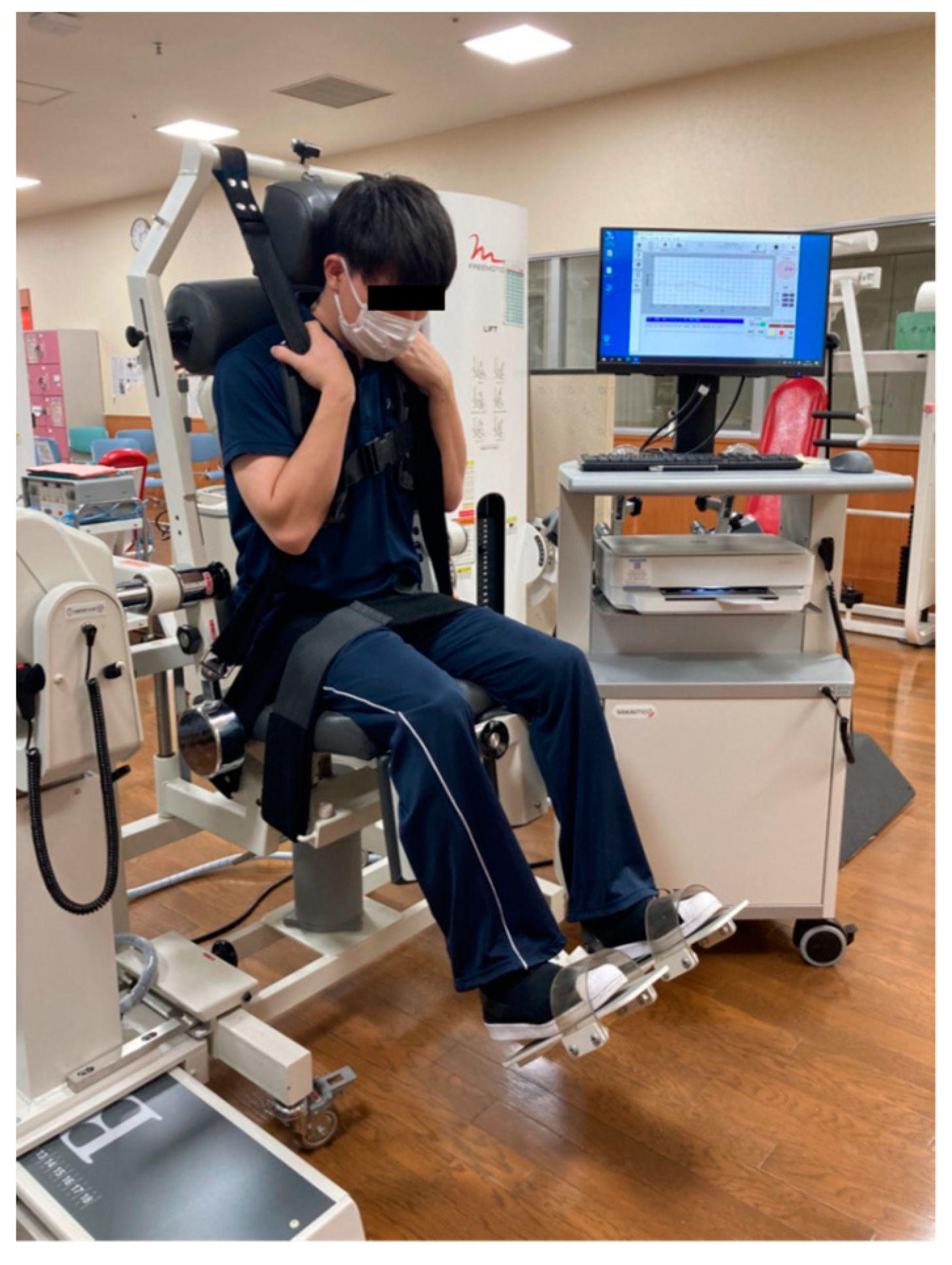
2.3. Isokinetic Trunk Muscle Strength
2.4. Data Processing
3. Results
3.1. Difference in Muscle Strength between the First and 1M
3.1.1. Angular Velocity of 60°/s
3.1.2. Angular Velocity of 120°/s, 180°/s
3.2. Correlation between Isokinetic Trunk Muscle Strength at First and Return to Sports Competition Days
3.2.1. Angular Velocity of 60°/s
3.2.2. Angular Velocity of 120°/s, 180°/s
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chosa, E.; Totoribe, K.; Tajima, N. A Biomechanical Study of Lumbar Spondylolysis Based on a Three-Dimensional Finite Element Method. J. Orthop. Res. 2004, 22, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.E.; Baker, D.; McHolick, W.J.; Yuan, H.A.; Lubicky, J.P. The Natural History of Spondylolysis and Spondylolisthesis. J. Bone Joint Surg. Am. 1984, 66, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Ochoa, J.K.; Lubinus, A.; Timon, S.; Lee, Y.P.; Bhatia, N.N. Management of Lumbar Spondylolysis in the Adolescent Athlete: A Review of over 200 Cases. Spine J. 2022, 22, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Takahashi, H.; Nakajima, A.; Kubota, G.; Watanabe, A.; Nakajima, T.; Eguchi, Y.; Orita, S.; Fukuchi, H.; Yanagawa, N.; et al. Prevalence of Lumbar Spondylolysis and Spondylolisthesis in Patients with Degenerative Spinal Disease. Sci. Rep. 2020, 10, 6739. [Google Scholar] [CrossRef] [Green Version]
- Sairyo, K.; Goel, V.K.; Masuda, A.; Vishnubhotla, S.; Faizan, A.; Biyani, A.; Ebraheim, N.; Yonekura, D.; Murakami, R.-I.; Terai, T. Three Dimensional Finite Element Analysis of the Pediatric Lumbar Spine. Part II: Biomechanical Change as the Initiating Factor for Pediatric Isthmic Spondylolisthesis at the Growth Plate. Eur. Spine J. 2006, 15, 930–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, Y.; Sakai, T.; Sairyo, K. What Type of Orthosis Is Optimal for Conservative Treatment of Lumbar Spondylolysis? A Biomechanical Analysis. Spine Surg. Relat. Res. 2020, 4, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Sairyo, K.; Sakai, T.; Yasui, N.; Dezawa, A. Conservative Treatment for Pediatric Lumbar Spondylolysis to Achieve Bone Healing Using a Hard Brace: What Type and How Long? Clinical Article. J. Neurosurg. Spine 2012, 16, 610–614. [Google Scholar] [CrossRef]
- Christensen, B.; Dyrberg, E.; Aagaard, P.; Kjaer, M.; Langberg, H. Short-Term Immobilization and Recovery Affect Skeletal Muscle but Not Collagen Tissue Turnover in Humans. J. Appl. Physiol. (1985) 2008, 105, 1845–1851. [Google Scholar] [CrossRef] [Green Version]
- Hortobágyi, T.; Dempsey, L.; Fraser, D.; Zheng, D.; Hamilton, G.; Lambert, J.; Dohm, L. Changes in Muscle Strength, Muscle Fibre Size and Myofibrillar Gene Expression after Immobilization and Retraining in Humans. J. Physiol. 2000, 524, 293–304. [Google Scholar] [CrossRef] [Green Version]
- Hides, J.; Stanton, W. Muscle Imbalance among Elite Australian Rules Football Players: A Longitudinal Study of Changes in Trunk Muscle Size. J. Athl. Train. 2012, 47, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Iwamoto, J.; Takeda, T.; Wakano, K. Returning Athletes with Severe Low Back Pain and Spondylolysis to Original Sporting Activities with Conservative Treatment. Scand. J. Med. Sci. Sports 2004, 14, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Goetzinger, S.; Courtney, S.; Yee, K.; Welz, M.; Kalani, M.; Neal, M. Spondylolysis in Young Athletes: An Overview Emphasizing Nonoperative Management. J. Sports Med. (Hindawi. Publ. Corp) 2020, 2020, 9235958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- el Rassi, G.; Takemitsu, M.; Woratanarat, P.; Shah, S.A. Lumbar Spondylolysis in Pediatric and Adolescent Soccer Players. Am. J. Sports Med. 2005, 33, 1688–1693. [Google Scholar] [CrossRef]
- Wren, T.A.L.; Ponrartana, S.; Aggabao, P.C.; Poorghasamians, E.; Skaggs, D.L.; Gilsanz, V. Increased Lumbar Lordosis and Smaller Vertebral Cross-Sectional Area Are Associated With Spondylolysis. Spine 2018, 43, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Peng, B.-G.; Li, Y.-C.; Zhang, N.-Y.; Yang, L.; Li, D.-M. Differences of Sagittal Lumbosacral Parameters between Patients with Lumbar Spondylolysis and Normal Adults. Chin. Med. J. (Engl.) 2016, 129, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Albanese, M.; Pizzutillo, P.D. Family Study of Spondylolysis and Spondylolisthesis. J. Pediatr. Orthop. 1982, 2, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Tsukagoshi, Y.; Kamegaya, M.; Tatsumura, M.; Tomaru, Y.; Kamada, H.; Morita, M.; Saisu, T.; Nomura, S.; Ikezawa, Y.; Yamazaki, M. Characteristics and Diagnostic Factors Associated with Fresh Lumbar Spondylolysis in Elementary School-Aged Children. Eur. Spine J. 2020, 29, 2465–2469. [Google Scholar] [CrossRef]
- Iwaki, K.; Sakai, T.; Hatayama, D.; Hayashi, Y.; Inoue, N.; Mitsumoto, M.; Hattori, Y.; Goto, T.; Sairyo, K.; Tsuji, S. Physical Features of Pediatric Patients with Lumbar Spondylolysis and Effectiveness of Rehabilitation. J. Med. Investig. 2018, 65, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Crisco, J.J.; Panjabi, M.M.; Yamamoto, I.; Oxland, T.R. Euler Stability of the Human Ligamentous Lumbar Spine. Part II: Experiment. Clin. Biomech. 1992, 7, 27–32. [Google Scholar] [CrossRef]
- Izzo, R.; Guarnieri, G.; Guglielmi, G.; Muto, M. Biomechanics of the Spine. Part I: Spinal Stability. Eur. J. Radiol. 2013, 82, 118–126. [Google Scholar] [CrossRef]
- Lawrence, K.J.; Elser, T.; Stromberg, R. Lumbar Spondylolysis in the Adolescent Athlete. Phys. Ther. Sport 2016, 20, 56–60. [Google Scholar] [CrossRef]
- Standaert, C.J.; Herring, S.A. Expert Opinion and Controversies in Sports and Musculoskeletal Medicine: The Diagnosis and Treatment of Spondylolysis in Adolescent Athletes. Arch. Phys. Med. Rehabil. 2007, 88, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Grabiner, M.D.; Jeziorowski, J.J.; Divekar, A.D. Isokinetic Measurements of Trunk Extension and Flexion Performance Collected with the Biodex Clinical Data Station. J. Orthop. Sports Phys. Ther. 1990, 11, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.-W.; Chen, L.-C.; Hsu, H.-H.; Chiang, S.-L.; Li, M.-H.; Jiang, S.-H.; Tsai, K.-C. Isokinetic Muscle Strength of the Trunk and Bilateral Knees in Young Subjects with Lumbar Disc Herniation. Spine 2005, 30, E528–E533. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.-Z.; Liu, X.; Ni, G.-X. Angular Velocity Affects Trunk Muscle Strength and EMG Activation during Isokinetic Axial Rotation. Biomed Res. Int. 2014, 2014, 623191. [Google Scholar] [CrossRef] [PubMed]
- Belavý, D.L.; Gast, U.; Felsenberg, D. Exercise and Transversus Abdominis Muscle Atrophy after 60-d Bed Rest. Med. Sci. Sports Exerc. 2017, 49, 238–246. [Google Scholar] [CrossRef]
- Clark, B.C.; Issac, L.C.; Lane, J.L.; Damron, L.A.; Hoffman, R.L. Neuromuscular Plasticity during and Following 3 Wk of Human Forearm Cast Immobilization. J. Appl. Physiol. (1985) 2008, 105, 868–878. [Google Scholar] [CrossRef] [Green Version]
- Lundbye-Jensen, J.; Nielsen, J.B. Immobilization Induces Changes in Presynaptic Control of Group Ia Afferents in Healthy Humans. J. Physiol. 2008, 586, 4121–4135. [Google Scholar] [CrossRef]
- Murray, M.K.; Maxwell, J. Consideration of sport demands for an 18-year-old lacrosse player with recalcitrant symptomatic spondylolysis: A case report. Int. J. Sports Phys. Ther. 2020, 15, 1196–1210. [Google Scholar] [CrossRef]
- Hides, J.A.; Belavý, D.L.; Stanton, W.; Wilson, S.J.; Rittweger, J.; Felsenberg, D.; Richardson, C.A. Magnetic Resonance Imaging Assessment of Trunk Muscles during Prolonged Bed Rest. Spine 2007, 32, 1687–1692. [Google Scholar] [CrossRef]
- Trappe, S.; Trappe, T.; Gallagher, P.; Harber, M.; Alkner, B.; Tesch, P. Human Single Muscle Fibre Function with 84 Day Bed-Rest and Resistance Exercise. J. Physiol. 2004, 557, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Mülkoğlu, C.; Taşkın, S.; Vural, S.; Mansız Kaplan, B.; Selvi, A.B.; Genç, H. Isokinetic Evaluation of the Trunk Muscle Strength in Housewives with Fibromyalgia: A Cross-Sectional Study. Adv. Rheumatol. 2020, 60, 40. [Google Scholar] [CrossRef] [PubMed]
- Al-Shenqiti, A.M.; Emara, H.A.; Algarni, F.S.; Khaled, O.A. Isokinetic Trunk Muscle Performance in Adolescents with Different Body Mass Indices. J. Taibah. Univ. Med. Sci. 2021, 16, 550–557. [Google Scholar] [CrossRef]
- Tsuboi, H.; Nishimura, Y.; Sakata, T.; Tanina, H.; Arakawa, H.; Nakamura, T.; Umezu, Y.; Tajima, F. Properties of Paraspinal Muscles in Japanese High School Baseball Players With Terminal-Stage Lumbar Spondylolysis. PM&R 2018, 10, 175–182. [Google Scholar] [CrossRef]
- Hiemstra, L.A.; Webber, S.; MacDonald, P.B.; Kriellaars, D.J. Hamstring and Quadriceps Strength Balance in Normal and Hamstring Anterior Cruciate Ligament-Reconstructed Subjects. Clin. J. Sport Med. 2004, 14, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Croisier, J.-L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.-M. Strength Imbalances and Prevention of Hamstring Injury in Professional Soccer Players: A Prospective Study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | |
|---|---|
| Sex, n; Male/Female | 10/0 |
| Age (years) | 13.5 ± 1.7 |
| body weight (kg) | 56.5 ± 9.1 |
| The level of separation | L4; 2, L5; 8 |
| Separation Characteristics, unilateral/bilateral | 5/5 |
| Sports competition, n; baseball/soccer/track and field/volleyball/basketball | 3/4/1/1/1 |
| Corset wearing period (days) | 56.0 ± 17.0 |
| Corset off to return to sports competition (days) | 42.8 ± 22.7 |
| First (n = 10) | 1M (n = 10) | p-Value | 95% CI | Effect Size | ||
|---|---|---|---|---|---|---|
| 60°/s | ||||||
| maximum torque/body weight ratio | 88.1 ± 27.59 | 125.9 ± 33.61 | 0.003 * | −59.25 | −16.37 | 1.26 |
| maximum torque generation time | 443.0 ± 336.68 | 293.2 ± 198.96 | 0.223 | −115.30 | 414.90 | 0.40 |
| maximum torque angle | 115.0 ± 16.45 | 116.2 ± 20.20 | 0.877 | −18.31 | 15.91 | 0.05 |
| maximum work/body weight ratio | 78.7 ± 25.79 | 104.6 ± 32.64 | 0.004 | −41.10 | −10.56 | 1.21 |
| 120°/s | ||||||
| maximum torque/body weight ratio | 71.4 ± 16.28 | 116.5 ± 34.66 | <0.001 * | −64.13 | −26.05 | 1.69 |
| maximum torque generation time | 235.0 ± 119.19 | 194.0 ± 101.67 | 0.318 | −46.64 | 128.64 | 0.34 |
| maximum torque angle | 115.0 ± 18.38 | 117.7 ± 12.84 | 0.615 | −14.44 | 9.04 | 0.17 |
| maximum work/body weight ratio | 63.7 ±18.34 | 92.5 ± 31.86 | 0.003 * | −44.70 | −12.74 | 1.29 |
| 180°/s | ||||||
| maximum torque/body weight ratio | 59.0 ± 17.07 | 95.57 ± 41.91 | 0.010 * | −61.96 | −11.26 | 1.03 |
| maximum torque generation time | 213.0 ± 82.7 | 168.0 ± 72.23 | 0.080 | −6.61 | 96.61 | 0.62 |
| maximum torque angle | 107.8 ± 13.37 | 112.3 ± 13.28 | 0.269 | −13.15 | 4.15 | 0.60 |
| maximum work/body weight ratio | 40.1 (34.9−43.5) | 84.7 (64.6−139.4) | 0.037 * | - | - | 0.66 |
| First (n = 10) | 1M (n = 10) | p-Value | 95% CI | Effect Size | ||
|---|---|---|---|---|---|---|
| 60°/s | ||||||
| Flexion/Extension ratio | 67.4 (53.4−81.5) | 65.5 (57.6−77.2) | 0.959 | - | - | 0.16 |
| maximum torque/body weight ratio | 59.6 ± 11.44 | 84.1 ± 18.14 | 0.002 * | −36.85 | −12.17 | 1.42 |
| maximum torque generation time | 435.0 (130.0−680.0) | 170.0 (150.0−320.0) | 0.168 | - | - | 0.44 |
| maximum torque angle | 82.5 (73.0−100.0) | 73.5 (72.0−76.0) | 0.168 | - | - | 0.44 |
| maximum work/body weight ratio | 50.8 ± 13.28 | 60.8 ± 10.73 | 0.002 * | −15.34 | −4.62 | 1.33 |
| 120°/s | ||||||
| Flexion/Extension ratio | 75.7 (49.8−78.3) | 61.4 (56.5−63.6) | 0.333 | - | - | 0.31 |
| maximum torque/body weight ratio | 46.7 (39.8−57.0) | 64.1 (57.4−85.7) | 0.005 * | - | - | 0.89 |
| maximum torque generation time | 345.0 (280.0 - 450.0) | 180.0 (170.0−250.0) | 0.028 * | - | - | 0.69 |
| maximum torque angle | 95.2 ± 14.80 | 86.2 ± 10.08 | 0.201 | −5.76 | 23.76 | 0.44 |
| maximum work/body weight ratio | 38.4 ±15.10 | 54.8 ± 15.47 | <0.001 * | −22.63 | −10.15 | 1.88 |
| 180°/s | ||||||
| Flexion/Extension ratio | 70.2 (64.6−77.1) | 55.5 (48.4−85.10) | 0.575 | - | - | 0.18 |
| maximum torque/body weight ratio | 41.0 ± 13.87 | 55.5 ± 14.01 | 0.005 * | −23.50 | −5.46 | 1.15 |
| maximum torque generation time | 352.0 ± 124.79 | 268.0 ± 98.52 | 0.030 * | 10.03 | 157.97 | 0.81 |
| maximum torque angle | 112.0 (98.0−114.0) | 102.0 (97.0−111.0) | 0.415 | - | - | 0.26 |
| maximum work/body weight ratio | 27.6 ± 13.99 | 39.8 ± 16.29 | <0.001 * | −16.85 | −6.35 | 1.58 |
| p-Value | 95%CI | r-Value | Power (1-β) | ||
|---|---|---|---|---|---|
| 60°/s | |||||
| maximum torque / body weight ratio | 0.674 | −0.53 | 0.71 | 0.153 | 0.07 |
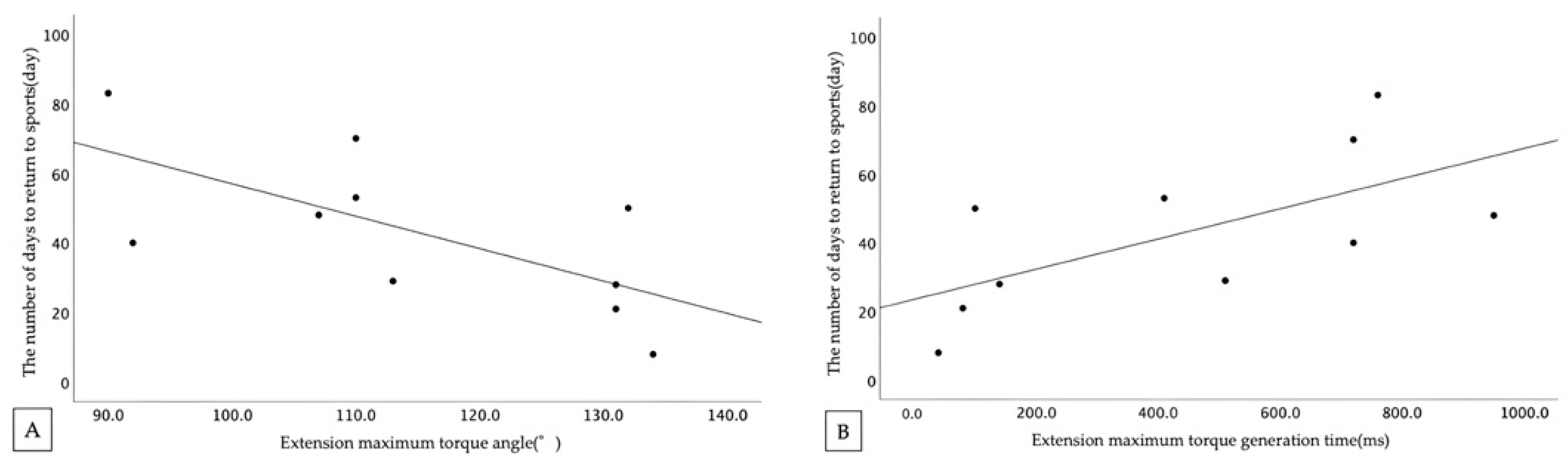
| maximum torque generation time | 0.041 * | 0.04 | 0.91 | 0.651 ** | 0.62 |
| maximum torque angle | 0.033 * | −0.92 | −0.08 | −0.674 ** | 0.58 |
| maximum work / body weight ratio | 0.348 | −0.38 | 0.80 | 0.332 | 0.154 |
| 120°/s | |||||
| maximum torque / body weight ratio | 0.667 | −0.72 | 0.52 | −0.156 | 0.07 |
| maximum torque generation time | 0.904 | −0.60 | 0.66 | 0.044 | 0.051 |
| maximum torque angle | 0.683 | −0.53 | 0.71 | 0.148 | 0.068 |
| maximum work / body weight ratio | 0.621 | −0.73 | 0.51 | −0.179 | 0.077 |
| 180°/s | |||||
| maximum torque / body weight ratio | 0.828 | −0.58 | 0.68 | 0.079 | 0.055 |
| maximum torque generation time | 0.431 | −0.77 | 0.42 | −0.281 | 0.121 |
| maximum torque angle | 0.286 | −0.33 | 0.81 | 0.375 | 0.188 |
| maximum work / body weight ratio | 0.869 | - | - | 0.06 | 0.052 |
| p-Value | 95%CI | r-Value | Power (1-β) | ||
|---|---|---|---|---|---|
| 60°/s | |||||
| Flexion/Extension ratio | 0.952 | −0.62 | 0.64 | 0.022 | 0.05 |
| maximum torque/body weight ratio | 0.281 | −0.33 | 0.81 | 0.379 | 0.191 |
| maximum torque generation time | 0.967 | −0.64 | 0.62 | −0.015 | 0.05 |
| maximum torque angle | 0.527 | −0.47 | 0.75 | 0.227 | 0.095 |
| maximum work/body weight ratio | 0.159 | −0.21 | 0.85 | 0.481 | 0.301 |
| 120°/s | |||||
| Flexion/Extension ratio | 0.021 * | 0.15 | 0.93 | 0.712 ** | 0.703 |
| maximum torque/body weight ratio | 0.076 | −0.07 | 0.89 | 0.584 | 0.457 |
| maximum torque generation time | 0.843 | −0.67 | 0.58 | −0.072 | 0.054 |
| maximum torque angle | 0.131 | −0.17 | 0.86 | 0.511 | 0.342 |
| maximum work/body weight ratio | 0.073 | −0.06 | 0.89 | 0.59 | 0.468 |
| 180°/s | |||||
| Flexion/Extension ratio | 0.038 * | 0.05 | 0.91 | 0.659 ** | 0.597 |
| maximum torque/body weight ratio | 0.154 | −0.20 | 0.85 | 0.486 | 0.308 |
| maximum torque generation time | 0.424 | −0.78 | 0.42 | −0.285 | 0.124 |
| maximum torque angle | 0.333 | −0.37 | 0.80 | 0.342 | 0.161 |
| maximum work/body weight ratio | 0.181 | −0.24 | 0.84 | 0.46 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamada, Y.; Okubo, Y.; Hattori, H.; Nazuka, T.; Kikuchi, Y.; Akasaka, K. Relationship between Isokinetic Trunk Muscle Strength and Return to Sports Competition after Conservative Therapy in Fresh Cases of Lumbar Spondylolysis: A Retrospective Observational Study. Healthcare 2023, 11, 625. https://doi.org/10.3390/healthcare11040625
Hamada Y, Okubo Y, Hattori H, Nazuka T, Kikuchi Y, Akasaka K. Relationship between Isokinetic Trunk Muscle Strength and Return to Sports Competition after Conservative Therapy in Fresh Cases of Lumbar Spondylolysis: A Retrospective Observational Study. Healthcare. 2023; 11(4):625. https://doi.org/10.3390/healthcare11040625
Chicago/Turabian StyleHamada, Yuji, Yu Okubo, Hiroshi Hattori, Takeshi Nazuka, Yuto Kikuchi, and Kiyokazu Akasaka. 2023. "Relationship between Isokinetic Trunk Muscle Strength and Return to Sports Competition after Conservative Therapy in Fresh Cases of Lumbar Spondylolysis: A Retrospective Observational Study" Healthcare 11, no. 4: 625. https://doi.org/10.3390/healthcare11040625