
Muscle Activity Characteristics of the Pronator Teres during Throwing in Baseball Pitchers: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
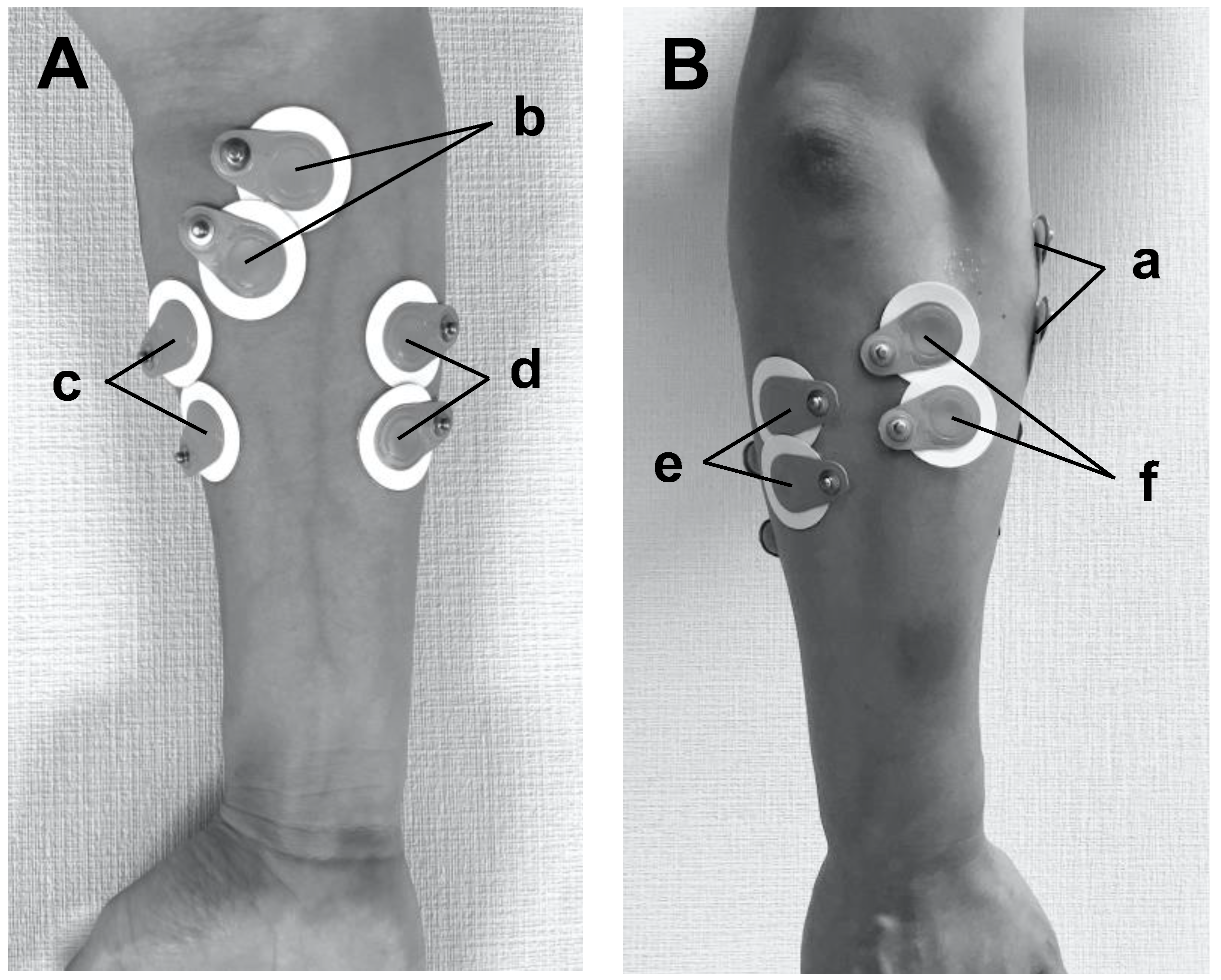
2.3. Instrumentation and Measurement Protocols
2.4. Phases of the Pitching Cycle
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
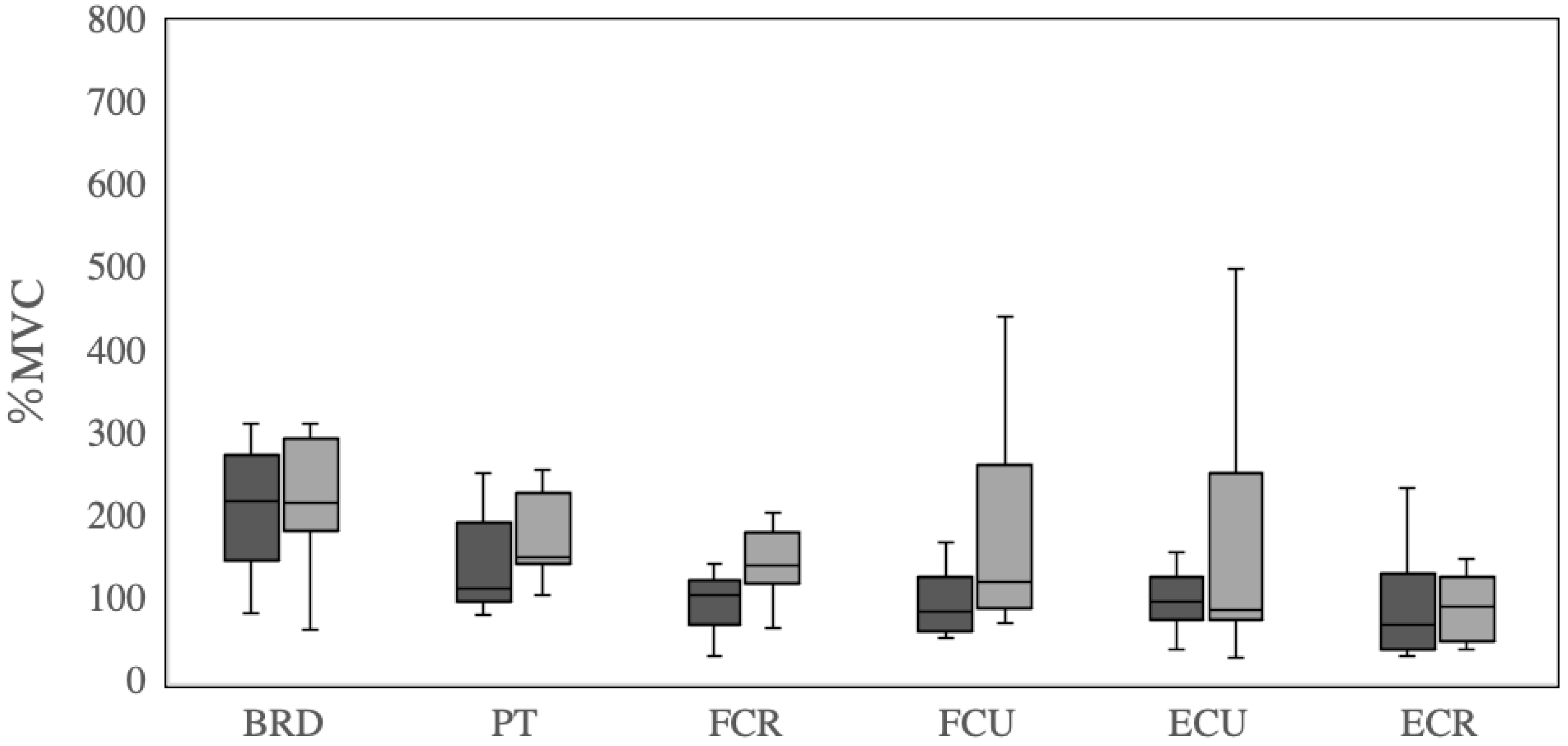
3.1. Average EMG Values
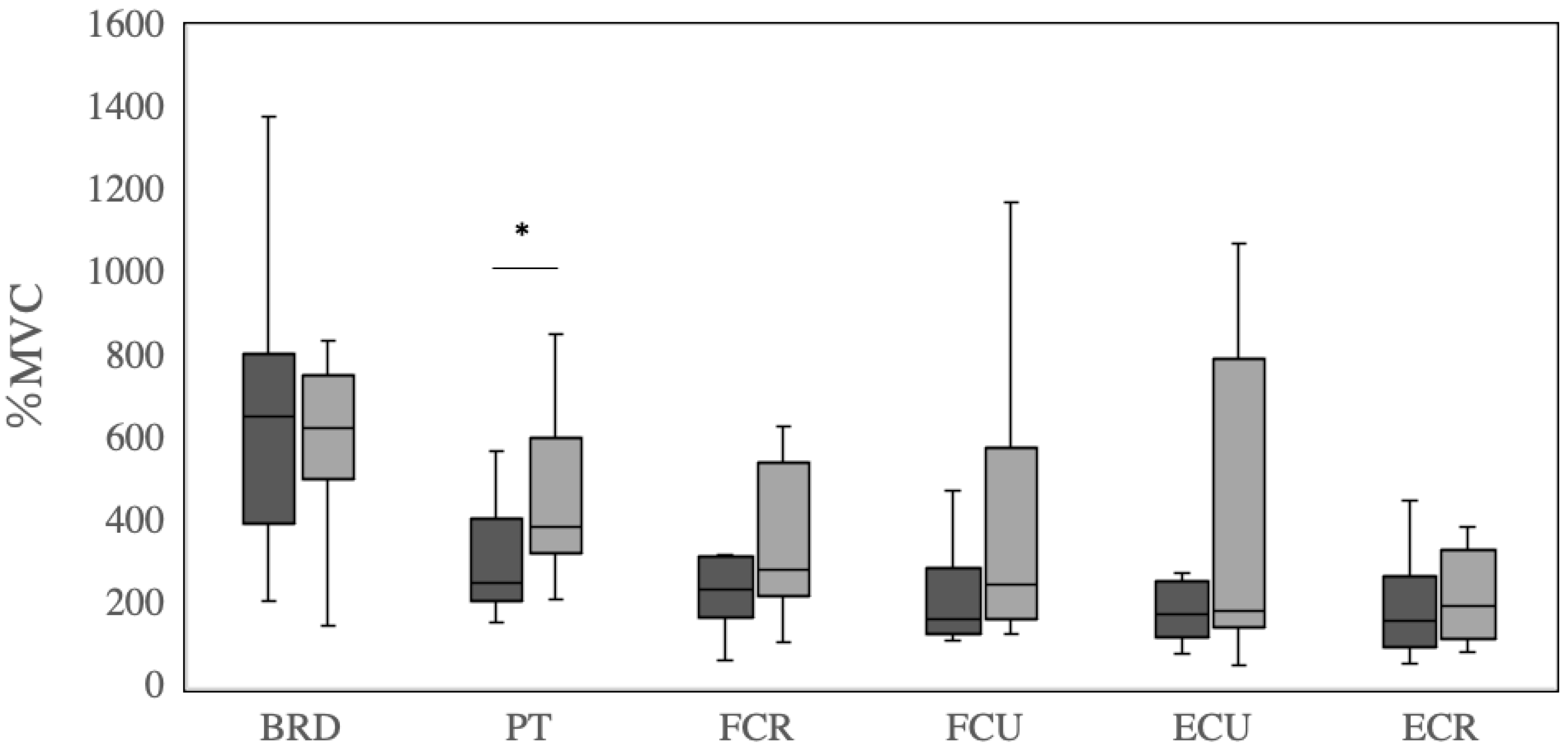
3.2. Peak EMG Values
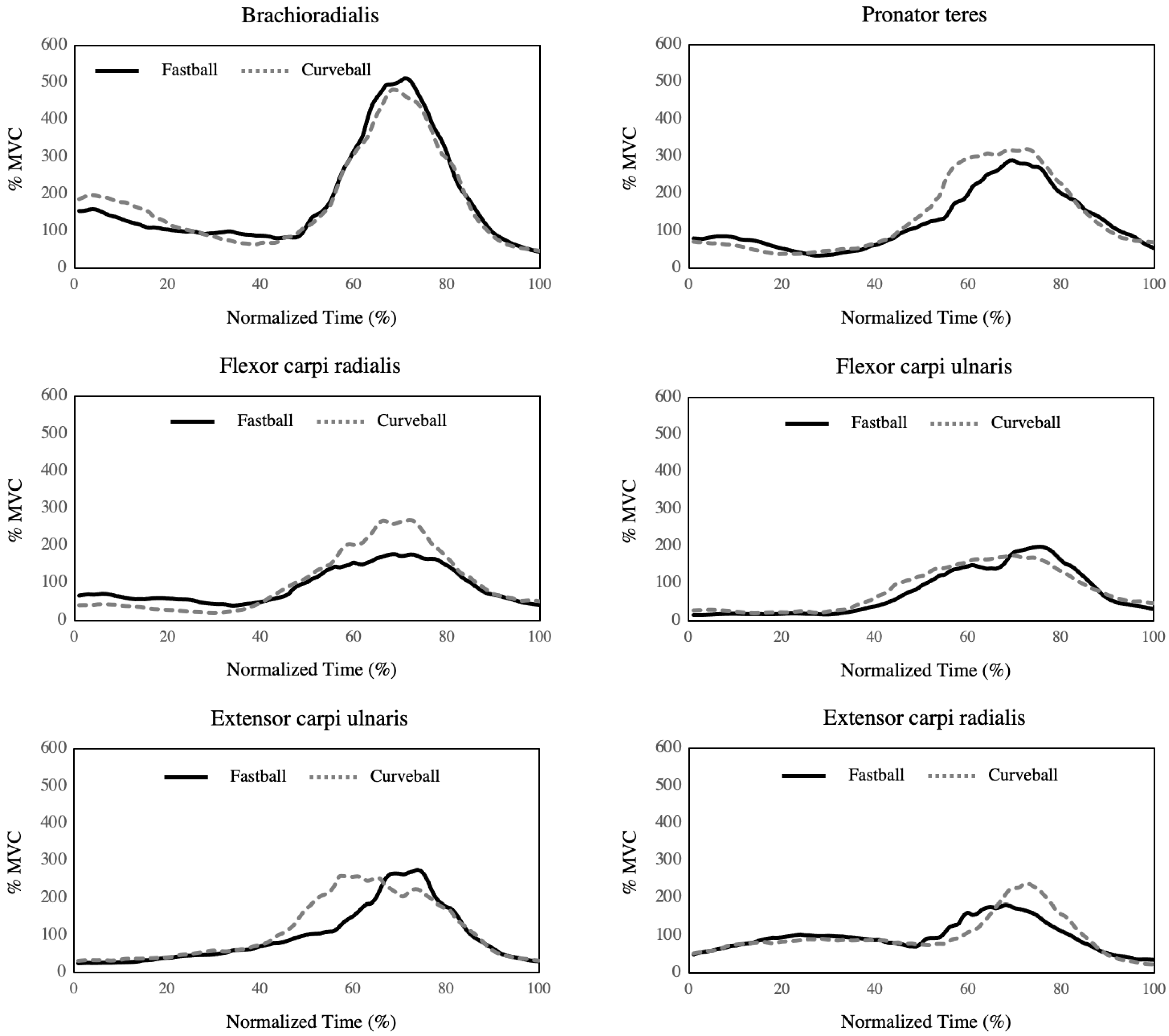
3.3. Time-Series EMG Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Werner, S.L.; Murray, T.A.; Hawkins, R.J.; Gill, T.J. Relationship between throwing mechanics and elbow valgus in professional baseball pitchers. J. Shoulder Elb. Surg. 2002, 11, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Sabick, M.B.; Torry, M.R.; Lawton, R.L.; Hawkins, R.J. Valgus torque in youth baseball pitchers: A biomechanical study. J. Shoulder Elb. Surg. 2004, 13, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Lyman, S.; Fleisig, G.S.; Andrews, J.R.; Osinski, E.D. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am. J. Sports Med. 2002, 30, 463–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, K.; Burton, K.J.; Rodner, C.; Smith, B.; Caputo, A.E. Lateral compression injuries in the pediatric elbow: Panner’s disease and osteochondritis dissecans of the capitellum. J. Am. Acad. Orthop. Surg. 2004, 12, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Osbahr, D.C.; Chalmers, P.N.; Frank, J.S.; Williams, R.J.; Widmann, R.F.; Green, D.W. Acute, avulsion fractures of the medial epicondyle while throwing in youth baseball players: A variant of Little League elbow. J. Shoulder Elb. Surg. 2010, 19, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Tisano, B.K.; Estes, A.R. Overuse Injuries of the Pediatric and Adolescent Throwing Athlete. Med. Sci. Sports Exerc. 2016, 48, 1898–1905. [Google Scholar] [CrossRef] [PubMed]
- Looney, A.M.; Rigor, P.D.; Bodendorfer, B.M. Evaluation and management of elbow injuries in the adolescent overhead athlete. SAGE Open Med. 2021, 9, 205031212110033. [Google Scholar] [CrossRef]
- Smidebush, M.; Stewart, E.; Shapiro, R.; Chander, H.; Knight, A. Mean muscle activation comparison between fastballs and curveballs with respect to the upper and lower extremity. J. Biomech. 2019, 94, 187–192. [Google Scholar] [CrossRef]
- Escamilla, R.F.; Fleisig, G.S.; Groeschner, D.; Akizuki, K. Biomechanical Comparisons Among Fastball, Slider, Curveball, and Changeup Pitch Types and Between Balls and Strikes in Professional Baseball Pitchers. Am. J. Sports Med. 2017, 45, 3358–3367. [Google Scholar] [CrossRef]
- Atwater, A.E. Biomechanics of Overarm Throwing Movements and of Throwing Injuries. Exerc. Sport Sci. Rev. 1979, 7, 43–85. [Google Scholar] [CrossRef]
- Sakurai, S.; Ikegami, Y.; Okamoto, A.; Yabe, K.; Toyoshima, S. A three-dimensional cinematographic analysis of upper limb movement during fastball and curveball baseball pitches. Int. J. Sport. Biomech. 1993, 9, 47–65. [Google Scholar] [CrossRef]
- Solomito, M.J.; Garibay, E.J.; Nissen, C.W. A Biomechanical Analysis of the Association Between Forearm Mechanics and the Elbow Varus Moment in Collegiate Baseball Pitchers. Am. J. Sports Med. 2018, 46, 52–57. [Google Scholar] [CrossRef] [Green Version]
- DiGiovine, N.M.; Jobe, F.W.; Pink, M.; Perry, J. An electromyographic analysis of the upper extremity in pitching. J. Shoulder Elb. Surg. 1992, 1, 15–25. [Google Scholar] [CrossRef]
- Davidson, P.A.; Pink, M.; Perry, J.; Jobe, F.W. Functional anatomy of the flexor pronator muscle group in relation to the medial collateral ligament of the elbow. Am. J. Sports Med. 1995, 23, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Minagawa, H.; Watanabe, H.; Kawasaki, T.; Okada, K. Elasticity of the pronator teres muscle in youth baseball players with elbow injuries: Evaluation using ultrasound strain elastography. J. Shoulder Elb. Surg. 2018, 27, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Seyffarth, H. Primary myoses in the M. pronator teres as cause of lesion of the N. medianus (the pronator syndrome). Acta Psychiatr. Neurol. Scand. Suppl. 1951, 74, 251–254. [Google Scholar]
- Dididze, M.; Tafti, D.; Sherman, A.L. Pronator Teres Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Loomer, R. L. Elbow injuries in athletes. Can. J. Appl. Sport. Sci. 1982, 7, 164–166. [Google Scholar] [PubMed]
- Oliver, G.D.; Plummer, H.; Henning, L.; Saper, M.; Glimer, G.; Brambeck, A.; Andrews, J.R. Effects of a Simulated Game on Upper Extremity Pitching Mechanics and Muscle Activations Among Various Pitch Types in Youth Baseball Pitchers. J. Pediatr. Orthop. 2019, 39, 387–393. [Google Scholar] [CrossRef]
- Farì, G.; Megna, M.; Ranieri, M.; Agostini, F.; Ricci, V.; Bianchi, F.P.; Rizzo, L.; Farì, E.; Tognolo, L.; Bonavolontà, V.; et al. Could the Improvement of Supraspinatus Muscle Activity Speed up Shoulder Pain Rehabilitation Outcomes in Wheelchair Basketball Players? Int. J. Environ. Res. Public Health 2022, 20, 255. [Google Scholar] [CrossRef]
- Farì, G.; Santagati, D.; Macchiarola, D.; Ricci, V.; Di Paolo, S.; Caforio, L.; Invernizzi, M.; Notarnicola, A.; Megna, M.; Ranieri, M. Musculoskeletal pain related to surfing practice: Which role for sports rehabilitation strategies? A cross-sectional study. J. Back. Musculoskelet. Rehabil. 2022, 35, 911–917. [Google Scholar] [CrossRef]
- Fleisig, G.S.; Barrentine, S.W.; Escamilla, R.F.; Andrews, J.R. Biomechanics of overhand throwing with implications for injuries. Sports Med. 1996, 21, 421–437. [Google Scholar] [CrossRef] [PubMed]
- Mayes, M.; Salesky, M.; Lansdown, D.A. Throwing Injury Prevention Strategies with a Whole Kinetic Chain-Focused Approach. Curr. Rev. Musculoskelet. Med. 2022, 15, 53–64. [Google Scholar] [CrossRef]
- Lipinski, C.L.; Donovan, L.; McLoughlin, T.J.; Armstrong, C.W.; Norte, G.E. Surface electromyography of the forearm musculature during an overhead throwing rehabilitation progression program. Phys. Ther. Sport. 2018, 33, 109–116. [Google Scholar] [CrossRef]
- Escamilla, R.F.; Andrews, J.R. Shoulder muscle recruitment patterns and related biomechanics during upper extremity sports. Sports Med. 2009, 39, 569–590. [Google Scholar] [CrossRef]
- Udall, J. H.; Fitzpatrick, M. J.; McGarry, M. H.; Leba, T. B.; Lee, T. Q. Effects of flexor-pronator muscle loading on valgus stability of the elbow with an intact, stretched, and resected medial ulnar collateral ligament. J. Shoulder. Elbow. Surg. 2009, 18, 773–778. [Google Scholar] [CrossRef]
- Javed, O.; Maldonado, K.A.; Ashmyan, R. Anatomy, Shoulder and Upper Limb, Muscles. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Rassier, D.E.; MacIntosh, B.R.; Herzog, W. Length dependence of active force production in skeletal muscle. J. Appl. Physiol. 1999, 86, 1445–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCully, K.K.; Faulkner, J.A. Characteristics of lengthening contractions associated with injury to skeletal muscle fibers. J. Appl. Physiol. 1986, 61, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Fleisig, G.S.; Kingsley, D.S.; Loftice, J.W.; Dinnen, K.P.; Ranganathan, R.; Dun, S.; Escamilla, R.F.; Andrews, J.R. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am. J. Sports Med. 2006, 34, 423–430. [Google Scholar] [CrossRef]
- Jinji, T.; Sakurai, S. Direction of spin axis and spin rate of the pitched baseball. Sport. Biomech. 2006, 5, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Asker, M.; Brooke, H.L.; Waldén, M.; Tranaeus, U.; Johansson, F.; Skillgate, E.; Holm, L.W. Risk factors for, and prevention of, shoulder injuries in overhead sports: A systematic review with best-evidence synthesis. Br. J. Sports Med. 2018, 52, 1312–1319. [Google Scholar] [CrossRef]
- Wasserman, E.B.; Sauers, E.L.; Register-Mihalik, J.K.; Pierpoint, L.A.; Currie, D.W.; Knowles, S.B.; Dompier, T.P.; Comstock, R.D.; Marshall, S.W.; Kerr, Z.Y. The First Decade of Web-Based Sports Injury Surveillance: Descriptive Epidemiology of Injuries in US High School Boys’ Baseball (2005–2006 Through 2013–2014) and National Collegiate Athletic Association Men’s Baseball (2004–2005 Through 2013–2014). J. Athl. Train. 2019, 54, 198–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fastball | Curveball | Mean Difference (95% CI h) | t Value | p Value | Effect SizeCohen”s d | |
|---|---|---|---|---|---|---|
| Mean ± SD g | Mean ± SD g | |||||
| BRD a | 234.8 ± 125.8 | 220.8 ± 74.5 | 14.0 (−67.7–95.6) | 0.39 | 0.71 | 0.12 |
| PT b | 165.4 ± 114.4 | 192.7 ± 91.9 | −27.4 (−71.5–16.8) | −1.40 | 0.20 | −0.42 |
| FCR c | 114.9 ± 76.6 | 148.1 ± 42.5 | 33.2 (−79.6–13.2) | −1.62 | 0.14 | −0.49 |
| FCU d | 114.3 ± 82.9 | 181.0 ± 134.7 | −66.7 (−147.0–13.6) | −1.88 | 0.09 | −0.57 |
| ECU e | 135.7 ± 127.1 | 155.9 ± 144.0 | −20.2 (−169.0–128.6) | −0.31 | 0.77 | −0.09 |
| ECR f | 104.9 ± 90.5 | 111.9 ± 80.1 | −7.0 (−102.0–87.9) | −0.17 | 0.87 | −0.05 |
| Fastball | Curveball | Mean Difference (95% CI h) | t Value | p Value | Effect Size Cohen”s d | |
|---|---|---|---|---|---|---|
| Mean ± SD g | Mean ± SD g | |||||
| BRD a | 658.4 ± 329.3 | 598.1 ± 218.3 | 60.4 (−187.2–307.9) | 0.55 | 0.60 | 0.17 |
| PT b | 340.1 ± 226.2 | 450.4 ± 193.7 | −110.3 (−209.6–−10.9) | −2.51 | 0.03 * | −0.79 |
| FCR c | 260.2 ± 147.3 | 346.0 ± 175.8 | −85.8 (−219.2–47.5) | −1.46 | 0.18 | −0.46 |
| FCU d | 268.6 ± 260.5 | 428.6 ± 429.2 | −160.1 (−422.7–102.6) | −1.38 | 0.20 | −0.47 |
| ECU e | 308.6 ± 438.8 | 380.8 ± 371.8 | −72.2 (−531.1–386.7) | −0.36 | 0.73 | −0.11 |
| ECR f | 233.2 ± 229.1 | 269.3 ± 233.1 | −36.1 (−297.9–225.7) | −0.31 | 0.76 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamura, A.; Saito, M. Muscle Activity Characteristics of the Pronator Teres during Throwing in Baseball Pitchers: A Pilot Study. Healthcare 2023, 11, 618. https://doi.org/10.3390/healthcare11040618
Tamura A, Saito M. Muscle Activity Characteristics of the Pronator Teres during Throwing in Baseball Pitchers: A Pilot Study. Healthcare. 2023; 11(4):618. https://doi.org/10.3390/healthcare11040618
Chicago/Turabian StyleTamura, Akihiro, and Masami Saito. 2023. "Muscle Activity Characteristics of the Pronator Teres during Throwing in Baseball Pitchers: A Pilot Study" Healthcare 11, no. 4: 618. https://doi.org/10.3390/healthcare11040618