
Establishing Responsiveness and Minimal Clinically Important Difference of Quebec Back Pain Disability Scale (Hindi Version) in Chronic Low Back Pain Patients Undergoing Multimodal Physical Therapy
 , , ,
, , ,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
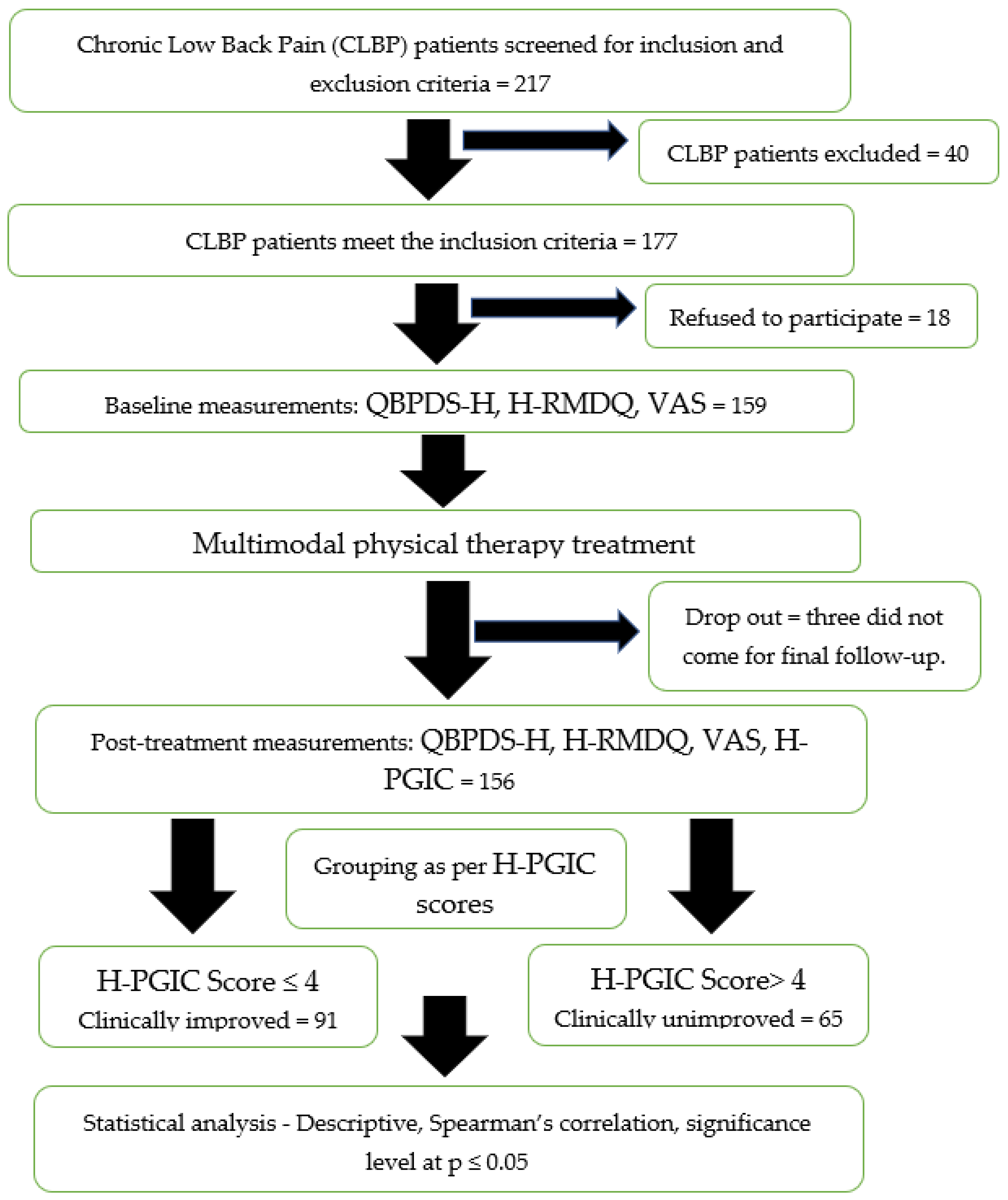
2.1. Design and Participants
2.2. Study Protocol
2.3. Questionnaires
2.4. Data Analysis
3. Results
4. Discussion
4.1. Clinical Significance
4.2. Limitations and Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paolucci, T.; Attanasi, C.; Cecchini, W.; Marazzi, A.; Capobianco, S.V.; Santilli, V. Chronic low back pain and postural rehabilitation exercise: A literature review. J. Pain Res. 2018, 12, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfliet, A.; Ickmans, K.; Huysmans, E.; Coppieters, I.; Willaert, W.; Van Bogaert, W.; Rheel, E.; Bilterys, T.; Van Wilgen, P.; Nijs, J. Best Evidence Rehabilitation for Chronic Pain Part 3: Low Back Pain. J. Clin. Med. 2019, 8, 1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipton, E.A. Physical Therapy Approaches in the Treatment of Low Back Pain. Pain. Ther. 2018, 7, 127–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, A. Evidence base and future research directions in the management of low back pain. World J. Orthop. 2016, 7, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Chang, C.H. Heterogeneity of Treatment Effect: Estimating How the Effects of Interventions Vary Across Individuals. JAMA 2021, 326, 2312–2313. [Google Scholar] [CrossRef]
- Beurskens, A.J.H.M.; de Vet, H.C.W.; Köke, A.J.A. Responsiveness of functional status in low back pain: A comparison of different instruments. Pain 1996, 65, 71–76. [Google Scholar] [CrossRef]
- Janwantanakul, P.; Sihawong, R.; Sitthipornvorakul, E.; Paksaichol, A. A screening tool for non-specificnon-specific low back pain with disability in office workers: A 1-year prospective cohort study. BMC Musculoskelet. Disord. 2015, 16, 298. [Google Scholar] [CrossRef] [Green Version]
- Deyo, R.A.; Dworkin, S.F.; Amtmann, D.; Andersson, G.; Borenstein, D.; Carragee, E.; Carrino, J.; Chou, R.; Cook, K.; Delitto, A.; et al. Report of the N.I.H. Task Force on Research Standards for Chronic Low Back Pain. Phys. Ther. 2015, 95, e1–e18. [Google Scholar] [CrossRef]
- Sihawong, R.; Sitthipornvorakul, E.; Paksaichol, A.; Janwantanakul, P. Predictors for chronic neck and low back pain in office workers: A 1-year prospective cohort study. J. Occup. Health 2016, 58, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Katajapuu, N.; Heinonen, A.; Saltychev, M. Minimal clinically important difference and minimal detectable change of the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) amongst patients with chronic musculoskeletal pain. Clin. Rehabil. 2020, 34, 1506–1511. [Google Scholar] [CrossRef]
- Müller, U.; Röder, C.; Greenough, C.G. Back related outcome assessment instruments. Eur. Spine J. 2006, 15 (Suppl. S1), S25–S31. [Google Scholar] [CrossRef] [Green Version]
- Longtin, C.; Décary, S.; Cook, C.E.; Martel, M.O.; Lafrenaye, S.; Carlesso, L.C.; Naye, F.; Tousignant-Laflamme, Y. Optimizing management of low back pain through the pain and disability drivers management model: A feasibility trial. PLoS ONE 2021, 16, e0245689. [Google Scholar] [CrossRef]
- Last, A.R.; Hulbert, K. Chronic low back pain: Evaluation and management. Am. Fam. Physician 2009, 79, 1067–1074. [Google Scholar] [CrossRef] [Green Version]
- Jacob, T.; Baras, M.; Zeev, A.; Epstein, L. Low back pain: Reliability of a set of pain measurement tools. Arch. Phys. Med. Rehabil. 2001, 82, 735–742. [Google Scholar] [CrossRef]
- Monticone, M.; Baiardi, P.; Vanti, C.; Ferrari, S.; Pillastrini, P.; Mugnai, R.; Foti, C. Responsiveness of the Oswestry Disability Index and the Roland Morris Disability Questionnaire in Italian subjects with sub-acute and chronic low back pain. Eur. Spine J. 2012, 21, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Kopec, J.A.; Esdaile, J.M.; Abrahamowicz, M.; Abenhaim, L.; Wood-Dauphinee, S.; Lamping, D.; Williams, J.I. The Quebec Back Pain Disability Scale. Measurement properties. Spine (Phila Pa 1976) 1995, 20, 341–352. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine (Phila Pa 1976) 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [Green Version]
- Holt, A.E.; Shaw, N.J.; Shetty, A.; Greenough, C.G. The reliability of the Low Back Outcome Score for back pain. Spine (Phila Pa 1976) 2002, 27, 206–210. [Google Scholar] [CrossRef]
- Zaidi, S.; Verma, S.; Moiz, J.A.; Hussain, M.E. Transcultural adaptation and validation of Hindi version of Quebec Back Pain Disability Scale. Disabil. Rehabil. 2018, 40, 2938–2945. [Google Scholar] [CrossRef]
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for assessing responsiveness: A critical review and recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Guyatt, G.; Walter, S.; Norman, G. Measuring change over time: Assessing the usefulness of evaluative instruments. J. Chronic Dis. 1987 1987, 40, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.D.; Hadorn, D. Responsiveness to change: An aspect of validity, not a separate dimension. Qual. Life Res. 1992, 1, 73–75. [Google Scholar] [CrossRef]
- The International Association for the Study of Pain (IASP) Task Force on Multimodal Pain Treatment Defines Terms for Chronic Pain Care. The IASP Council. 14 December 2017. Available online: https://www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=6981 (accessed on 5 March 2020).
- Demoulin, C.; Ostelo, R.; Knottnerus, J.A.; Smeets, R.J.E.M. Quebec Back Pain Disability Scale was responsive and showed reasonable interpretability after a multidisciplinary treatment. J. Clin. Epidemiol. 2010, 63, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Stratford, P.W.; Binkley, J.; Solomon, P.; Finch, E.; Gill, C.; Moreland, J. Defining the Minimum Level of Detectable Change for the Roland-Morris Questionnaire. Phys. Ther. 1996, 76, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Sharma, R.; Ghai, B.; Kumar, V.; Makkar, J.K.; Jain, A. Cross-cultural Adaptation and Validation of Hindi Version of Roland Morris Disability Questionnaire for Chronic Low Back Pain in Indian Population. Spine (Phila Pa 1976) 2023, 48, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Cruz, E.B.; Fernandes, R.; Carnide, F.; Vieira, A.; Moniz, S.; Nunes, F. Cross-cultural adaptation and validation of the Quebec Back Pain Disability Scale to European Portuguese language. Spine (Phila Pa 1976) 2013, 38, E1491–E1497. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: A clarification of its content. BMC Med. Res. Methodol. 2010, 10, 22. [Google Scholar] [CrossRef] [Green Version]
- Vieira, A.C.; Moniz, S.; Fernandes, R.; Carnide, F.; Cruz, E.B. Responsiveness and interpretability of the Portuguese version of the Quebec Back Pain Disability Scale in patients with chronic low back pain. Spine (Phila Pa 1976) 2014, 39, E346–E352. [Google Scholar] [CrossRef]
- de Vet, H.C.; Terwee, C.B.; Ostelo, R.W.; Beckerman, H.; Knol, D.L.; Bouter, L.M. Minimal changes in health status questionnaires: Distinction between minimally detectable change and minimally important change. Health Qual. Life Outcomes 2006, 4, 54. [Google Scholar] [CrossRef] [Green Version]
- Pereira, M.; Cruz, E.B.; Domingues, L.; Duarte, S.; Carnide, F.; Fernandes, R. Responsiveness and Interpretability of the Portuguese Version of the Neck Disability Index in Patients with Chronic Neck Pain Undergoing Physiotherapy. Spine 2015, 40, E1180–E1186. [Google Scholar] [CrossRef]
- Monticone, M.; Frigau, L.; Mola, F.; Rocca, B.; Franchignoni, F.; Simone Vullo, S.; Foti, C.; Chiarotto, A. The Italian version of the Quebec Back Pain Disability Scale: Cross-cultural adaptation, reliability and validity in patients with chronic low back pain. Eur. Spine J. 2020, 29, 530–539. [Google Scholar] [CrossRef]
- Karadağ, A.; Canbaş, M. Evaluation of the correlation between the Istanbul Low Back Pain Disability Index, Back Pain Functional Scale and other back pain disability scales in Turkish patients with low back pain. J. Back Musculoskelet. Rehabil. 2022, 35, 771–775. [Google Scholar] [CrossRef]
- Speksnijder, C.M.; Koppenaal, T.; Knottnerus, J.A.; Spigt, M.; Staal, J.B.; Terwee, C.B. Measurement Properties of the Quebec Back Pain Disability Scale in Patients with Nonspecific Low Back Pain: Systematic Review. Phys. Ther. 2016, 96, 1816–1831. [Google Scholar] [CrossRef] [Green Version]
- Pires, D.; Cruz, E.; Canhão, H.; Nunes, C. Minimum important change values for pain and disability: Which is the best to identify a meaningful response in patients with chronic nonspecific low back pain? Physiother. Theory Pract. 2022, 38, 1499–1507. [Google Scholar] [CrossRef]
- Monticone, M.; Arippa, F.; Foti, C.; Franchignoni, F. Responsiveness and Minimal Important Change of the Quebec Back Pain Disability Scale in Italian patients with chronic low back pain undergoing multidisciplinary rehabilitation. Eur. J. Phys. Rehabil. Med. 2022, 58, 435–441. [Google Scholar] [CrossRef]
- Cleland, J.; Gillani, R.; Bienen, E.J.; Sadosky, A. Assessing Dimensionality and Responsiveness of Outcomes Measures for Patients with Low Back Pain. Pain Pract. 2011, 11, 57–69. [Google Scholar] [CrossRef]
- Lauridsen, H.H.; Hartvigsen, J.; Manniche, C.; Korsholm, L.; Grunnet-Nilsson, N. Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC Musculoskelet Disord. 2006, 7, 82. [Google Scholar] [CrossRef] [Green Version]
- Coelho, R.A.; Siqueira, F.B.; Ferreira, P.H.; Ferreira, M.L. Responsiveness of the Brazilian-Portuguese version of the Oswestry Disability Index in subjects with low back pain. Eur. Spine J. 2008, 17, 1101–1106. [Google Scholar] [CrossRef] [Green Version]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and Pain Scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef]
- van der Roer, N.; Ostelo, R.W.J.G.; Bekkering, G.E.; van Tulder, M.W.; de Vet, H.C.W. Minimal Clinically Important Change for Pain Intensity, Functional Status, and General Health Status in Patients with Nonspecific Low Back Pain. Spine 2006, 31, 578–582. [Google Scholar] [CrossRef]
- Fritz, J.M.; Irrgang, J.J. A Comparison of a Modified Oswestry Low Back Pain Disability Questionnaire and the Quebec Back Pain Disability Scale. Phys. Ther. 2001, 81, 776–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, M.; Keating, J.L. A Comparison of Five Low Back Disability Questionnaires: Reliability and Responsiveness. Phys. Ther. 2002, 82, 8–24. [Google Scholar] [CrossRef] [PubMed]
- Ostelo, R.W.; Deyo, R.A.; Stratford, P.; Waddell, G.; Croft, P.; Von Korff, M.; Bouter, L.M.; de Vet, H.C. Interpreting change scores for pain and functional status in low back pain: Towards international consensus regarding minimal important change. Spine (Phila Pa 1976) 2008, 33, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Clinically Unimproved Group Mean (S.D.) (n = 65) | Clinically Improved Group Mean (S.D.) (n = 91) | t | p-Value |
|---|---|---|---|---|
| Age (years) | 44.16 (11.8) | 43.28 (10.7) | 0.424 | 0.672 |
| Weight (kg) | 70.16 (12.6) | 72.01 (8.4) | 0.421 | 0.675 |
| Height (cm) | 162.29 (10.3) | 163.10 (7.3) | 0.901 | 0.371 |
| BMI (kg/m2) | 26.45 (2.6) | 27.07 (2.4) | 1.299 | 0.197 |
| QBPDS-H pre | 36.06 (17.6) | 38.46 (13.8) | 0.703 | 0.482 |
| Variable | Group | Baseline | Post-Intervention | p-Value |
|---|---|---|---|---|
| QBPDS-H | Clinically unimproved (n = 65) | 36.06 (17.6) | 33.45 (18.9) | 0.169 |
| Clinically improved (n = 91) | 38.46 (13.8) | 26.01 (11.5) | <0.001 * |
| QBPDS-H 1 | Mean (S.D.) (n = 65) | ICC2,1 2 | SEM 3 | MDC 95% 4 |
|---|---|---|---|---|
| Pre | 36.06 (17.6) | 0.92 | 4.94 | 13.68 |
| Post | 33.45 (18.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, I.; Sharma, A.; Zaidi, S.; Alshahrani, M.S.; Gautam, A.P.; Raizah, A.; Reddy, R.S.; Verma, S.; Tanwar, T.; Hussain, M.E.; et al. Establishing Responsiveness and Minimal Clinically Important Difference of Quebec Back Pain Disability Scale (Hindi Version) in Chronic Low Back Pain Patients Undergoing Multimodal Physical Therapy. Healthcare 2023, 11, 621. https://doi.org/10.3390/healthcare11040621
Ahmad I, Sharma A, Zaidi S, Alshahrani MS, Gautam AP, Raizah A, Reddy RS, Verma S, Tanwar T, Hussain ME, et al. Establishing Responsiveness and Minimal Clinically Important Difference of Quebec Back Pain Disability Scale (Hindi Version) in Chronic Low Back Pain Patients Undergoing Multimodal Physical Therapy. Healthcare. 2023; 11(4):621. https://doi.org/10.3390/healthcare11040621
Chicago/Turabian StyleAhmad, Irshad, Akhil Sharma, Sahar Zaidi, Mastour Saeed Alshahrani, Ajay Prashad Gautam, Abdullah Raizah, Ravi Shankar Reddy, Shalini Verma, Tarushi Tanwar, Mohammad Ejaz Hussain, and et al. 2023. "Establishing Responsiveness and Minimal Clinically Important Difference of Quebec Back Pain Disability Scale (Hindi Version) in Chronic Low Back Pain Patients Undergoing Multimodal Physical Therapy" Healthcare 11, no. 4: 621. https://doi.org/10.3390/healthcare11040621