
Thoracic Spine Pain in High School Adolescents: A One-Year Longitudinal Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
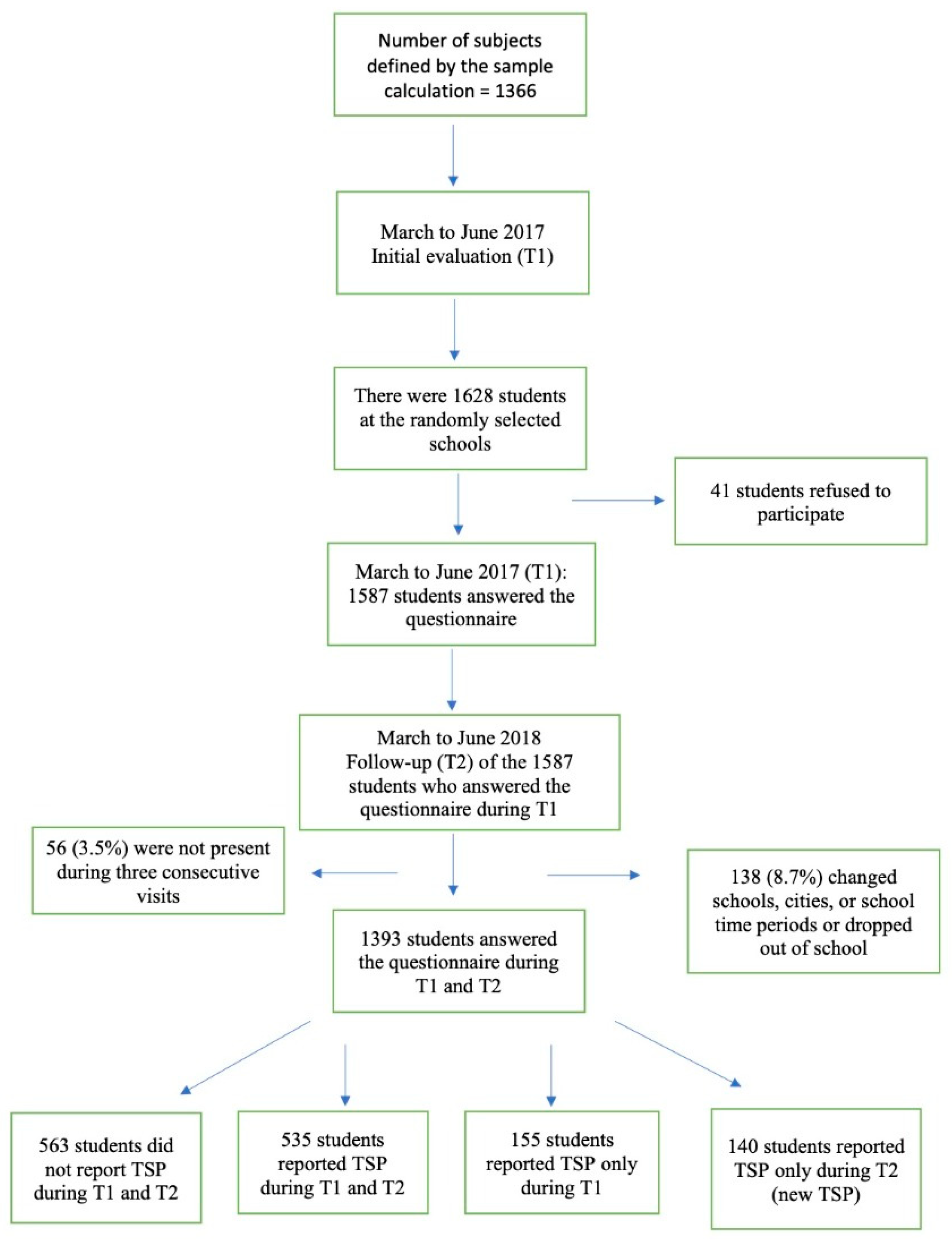
2.1. Design and Population
2.2. Sample Calculation
2.3. Inclusion and Exclusion Criteria
2.4. Variable Description
2.5. Explanatory Variables
2.6. Data Collection Procedure
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, N.L.S.; Mountjoy-Venning, W.C.; Anjomshoa, M.; Banoub, J.A.M.; Yasin, Y.J. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators (2018). Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study (vol 392, pg 1789, 2018). Lancet 2019, 393, E44. [Google Scholar]
- Kjaer, P.; Wedderkopp, N.; Korsholm, L.; Leboeuf-Yde, C. Prevalence and tracking of back pain from childhood to adolescence. BMC Musculoskelet. Disord. 2011, 12, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batley, S.; Aartun, E.; Boyle, E.; Hartvigsen, J.; Stern, P.J.; Hestbæk, L. The association between psychological and social factors and spinal pain in adolescents. Eur. J. Pediatr. 2019, 178, 275–286. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Noll, M.; Wedderkopp, N.; Mendonça, C.R.; Kjaer, P. Motor performance and back pain in children and adolescents: A sys-tematic review and meta-analysis protocol. Syst. Rev. 2020, 9, 212. [Google Scholar] [CrossRef]
- Montgomery, L.R.C.; Kamper, S.J.; Hartvigsen, J.; French, S.D.; Hestbaek, L.; Troelsen, J.; Swain, M.S. Exceeding 2-h sedentary time per day is not associated with moderate to severe spinal pain in 11- to 13-year-olds: A cross-sectional analysis. Eur. J. Pediatr. 2022, 181, 653–659. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Silva, A.G.; Sa-Couto, P.; Queirós, A.; Neto, M.; Rocha, N.P. Pain, pain intensity and pain disability in high school students are differently associated with physical activity, screening hours and sleep. BMC Musculoskelet. Disord. 2017, 18, 194. [Google Scholar] [CrossRef]
- Wirth, B.; Potthoff, T.; Rosser, S.; Humphreys, B.K.; De Bruin, E.D. Physical risk factors for adolescent neck and mid back pain: A systematic review. Chiropr. Man. Ther. 2018, 26, 36. [Google Scholar] [CrossRef] [Green Version]
- Heneghan, N.R.; Rushton, A. Understanding why the thoracic region is the ‘Cinderella’ region of the spine. Man. Ther. 2016, 21, 274–276. [Google Scholar] [CrossRef]
- Joergensen, A.C.; Strandberg-Larsen, K.; Andersen, P.K.; Hestbaek, L.; Andersen, A.-M.N. Spinal pain in pre-adolescence and the relation with screen time and physical activity behavior. BMC Musculoskelet. Disord. 2021, 22, 393. [Google Scholar] [CrossRef]
- Johansson, M.; Jensen Stochkendahl, M.; Hartvigsen, J.; Boyle, E.; Cassidy, J. Incidence and prognosis of mid-back pain in the general population: A systematic review. Eur. J. Pain 2017, 21, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zar, J.H. Biostatistical Analysis, 5th ed.; Prentice-Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- de Vitta, A.; Bento, T.P.F.; Cornelio, G.P.; Perrucini, P.D.D.O.; Felippe, L.A.; de Conti, M.H.S. Incidence and factors associated with low back pain in adolescents: A prospective study. Braz. J. Phys. Ther. 2021, 25, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Barros, E.N.C.; Alexandre, N.M.C. Cross-cultural adaptation of the nordic musculoskeletal questionnaire. Int. Nurs. Rev. 2003, 50, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Hestbaek, L.; Iachine, I.A.; Leboeuf-Yde, C.; Kyvik, K.O.; Manniche, C. Heredity of low back pain in a young population: A classical twin study. Twin Res. Hum. Genet. 2004, 7, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, G.D.; Silva, M.C.; Rombaldi, A.J.; Wrege, E.D.; Siqueira, F.V.; Hallal, P.C. Prevalence and associated factors of back pain in adults from southern Brazil: A population-based study. Braz. J. Phys. Ther. 2011, 15, 31–36. [Google Scholar] [CrossRef]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [Green Version]
- Shan, Z.; Deng, G.; Li, J.; Li, Y.; Zhang, Y.; Zhao, Q. Correlational Analysis of neck/shoulder Pain and Low Back Pain with the Use of Digital Products, Physical Activity and Psychological Status among Adolescents in Shanghai. PLoS ONE 2013, 8, e78109. [Google Scholar] [CrossRef]
- Chinapaw, M.J.; Mokkink, L.B.; van Poppel, M.N.; van Mechelen, W.; Terwee, C.B. Physical activity questionnaires for youth: A systematic review of measurement properties. Sports Med. 2010, 40, 539–563. [Google Scholar] [CrossRef]
- Guedes, D.P.; Lopes, C.C.; Guedes, J.E.R.P.; Stanganelli, L.C. Reproducibility and validity of the Baecke questionnaire for assessing of the habitual physical activity in adolescents. Rev. Port. Cien. Desp. 2006, 6, 265–274. [Google Scholar]
- Fleitlich-Bilyk, B.; Goodman, R. Prevalence of Child and Adolescent Psychiatric Disorders in Southeast Brazil. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 727–734. [Google Scholar] [CrossRef]
- Cury, C.R.; Golfeto, J.H. Strengths and difficulties questionnaire (SDQ): A study of school children in Ribeirão Preto. Rev. Bras. Psiquiatr. 2003, 25, 139–145. [Google Scholar] [CrossRef]
- Szpalski, M.; Gunzburg, R.; Balagué, F.; Nordin, M.; Mélot, C. A 2-year prospective longitudinal study on low back pain in primary school children. Eur. Spine J. 2002, 11, 459–464. [Google Scholar]
- Briggs, A.M.; Smith, A.J.; Straker, L.M.; Bragge, P. Thoracic spine pain in the general population: Prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet. Disord. 2009, 10, 77. [Google Scholar] [CrossRef] [Green Version]
- Aartun, E.; Hartvigsen, J.; Wedderkopp, N.; Hestbaek, L. Spinal pain in adolescents: Prevalence, incidence, and course: A school-based two-year prospective cohort study in 1300 Danes aged 11–13. BMC Musculoskelet. Disord. 2014, 15, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savedra, M.C.; Tesler, M.D.; Ward, J.D.; Wegner, C. How adolescents describe pain. J. Adolesc. Health Care 1988, 9, 315–320. [Google Scholar] [CrossRef]
- Goodman, J.E.; McGrath, P. The epidemiology of pain in children and adolescents: A review. Pain 1991, 46, 247–264. [Google Scholar] [CrossRef]
- Meucci, R.D.; Linhares, A.O.; Olmedo, D.W.; Cousin, S.E.; Duarte, V.M.; Almeida, C.J. Low back pain among adolescents in the semiarid region: Results of a population census in the city of Caracol, State of Piauí, Brazil. Cien. Saude. Colet. 2018, 23, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Torgén, M.; Swerup, C. Individual factors and physical work load in relation to sensory thresholds in a middle-aged general population sample. Eur. J. Appl. Physiol. 2002, 86, 418–427. [Google Scholar] [CrossRef]
- Ben Ayed, H.; Yaich, S.; Trigui, M.; Ben Hmida, M.; Ben Jemaa, M.; Ammar, A.; Jedidi, J.; Karray, R.; Feki, H.; Mejdoub, Y.; et al. Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J. Res. Health Sci. 2019, 19, e00440. [Google Scholar] [PubMed]
- Trevelyan, F.C.; Legg, S.J. Risk factors associated with back pain in New Zealand school children. Ergonomics 2011, 54, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.; Karoly, P. Fear-avoidance model of chronic pain: The next generation. Clin. J. Pain. 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Hubscher, M.; Moseley, G.L.; Kamper, S.J.; Traeger, A.C.; Mansell, G.; McAuley, J.H. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain 2015, 156, 988–997. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [Green Version]
- Domoff, S.E.; Borgen, A.L.; Foley, R.P.; Maffett, A. Excessive use of mobile devices and children’s physical health. Hum. Behav. Emerg. Technol. 2019, 1, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Berolo, S.; Wells, R.P.; Amick, B.C., III. Musculoskeletal symptoms among mobile hand-held device users and their relationship to device use: A preliminary study in a Canadian university population. Appl. Ergon. 2011, 42, 371–378. [Google Scholar] [CrossRef]
- Xie, Y.; Szeto, G.; Dai, J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Appl. Ergon. 2017, 59, 132–142. [Google Scholar] [CrossRef]
- Eitivipart, A.C.; Viriyarojanakul, S.; Redhead, L. Musculoskeletal disorder and pain associated with smartphone use: A systematic review of biomechanical evidence. Hong Kong Physiother. J. 2018, 38, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Roquelaure, Y.; Bodin, J.; Ha, C.; Le Marec, F.; Fouquet, N.; Ramond-Roquin, A.; Goldberg, M.; Descatha, A.; Petit, A.; Imbernon, E. Incidence and Risk Factors for Thoracic Spine Pain in the Working Population: The French Pays de la Loire Study. Arthritis Care Res. 2014, 66, 1695–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stallknecht, S.E.; Strandberg-Larsen, K.; Hestbæk, L.; Andersen, A.-M.N. Spinal pain and co-occurrence with stress and general well-being among young adolescents: A study within the Danish National Birth Cohort. Eur. J. Pediatr. 2017, 176, 807–814. [Google Scholar] [CrossRef] [PubMed]
- de Vitta, A.; Campos, L.D.; Bento, T.; Felippe, L.A.; Maciel, N.M.; Perrucini, P. Thoracic Spine Pain and Factors Associated in High School Students. Pain Manag. Nurs. 2022, 23, 517–523. [Google Scholar] [CrossRef]
- da Rosa, B.N.; Noll, M.; Candotti, C.T.; Loss, J.F. Risk Factors for Back Pain among Southern Brazilian School Children: A 6-Year Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 8322. [Google Scholar] [CrossRef] [PubMed]
- Miñana-Signes, V.; Monfort-Pañego, M.; Morant, J.; Noll, M. Cross-Cultural Adaptation and Reliability of the Back Pain and Body Posture Evaluation Instrument (BackPEI) to the Spanish Adolescent Population. Int. J. Environ. Res. Public Health 2021, 18, 854. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Candotti, C.T.; Rosa, B.N.D.; Vieira, A.; Loss, J.F. Back pain and its risk factors in Brazilian adolescents: A longitudinal study. Br. J. Pain 2021, 15, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Bento, T.P.F.; dos Santos Genebra, C.V.; Maciel, N.M.; Cornelio, G.P.; Simeão, S.F.A.P.; de Vitta, A. Low back pain and some associated factors: Is there any difference between genders? Braz. J. Phys. Ther. 2020, 24, 79–87. [Google Scholar] [CrossRef]
- Santos, E.D.S.; Bernardes, J.M.; Noll, M.; Gómez-Salgado, J.; Ruiz-Frutos, C.; Dias, A. Prevalence of Low Back Pain and Associated Risks in School-Age Children. Pain Manag. Nurs. 2021, 22, 459–464. [Google Scholar] [CrossRef]


{kind=link}
| TV habits | |
| During a normal school week, do you watch TV? | Yes/no |
| How many times per week do you watch TV? | 1 or 2 times, 3 or 4 times, 5 times, >5 times |
| How many hours per day do you watch TV? | Less than 1 h, 2 h, 3 h, 4 h, 5 h, >5 h |
| Computer use | |
| Do you use a computer? | Yes/no |
| What type of computer do you use? | Desktop/laptop |
| What is the height of your PC screen? | Eyes above the midpoint of the screen, approximately in the middle point of the screen, below the midpoint of the screen |
| How many times per week do you use a computer? | 1 or 2 times, 3 or 4 times, 5 times, >5 times |
| How many hours per day do you use a computer? | Less than 1 h, 2 h, 3 h, 4 h, 5 h, >5 h |
| What is the eye-to-screen distance while using your computer? | <20 cm, 20–25 cm, 25–30 cm, >30 cm |
| Cell phone use | |
| Do you use a cell phone? | Yes/no |
| What posture do you have while using the mobile phone? | Standing, sitting, lying down, semi-lying down |
| Average daily time spent using the cell phone? | <1 h, 2–3 h, 3–4 h, >4 h |
| What is the eye-to-screen distance during the use of the cell phone? | <10 cm, 10–15 cm, 15–20 cm, >20 cm |
| Tablet use | |
| Do you use a tablet? | Yes/no |
| What posture do you have while using the tablet? | Standing, sitting, lying down, semi-lying down |
| Average daily time spent using the tablet? | <1 h, 2–3 h, 3–4 h, >4 h |
| What is the eye-to-screen distance while using the tablet? | <10 cm, 10–15 cm, 15–20 cm, >20 cm |
| Factors | Baseline (T1) | Follow-Up (T2) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Age | ||||
| 14 years or younger | 216 | 15.1 | 216 | 15.1 |
| 15–18 years | 1.177 | 84.5 | 1177 | 84.5 |
| Sex | ||||
| Male | 693 | 49.7 | 693 | 49.7 |
| Female | 700 | 50.3 | 700 | 50.3 |
| Skin color | ||||
| White | 690 | 49.5 | 690 | 49.5 |
| Black | 130 | 9.3 | 130 | 9.3 |
| Brown | 530 | 38.0 | 530 | 38.0 |
| Yellow | 43 | 3.1 | 43 | 3.1 |
| Physical activity | ||||
| Active | 369 | 26.5 | 357 | 25.6 |
| Moderately active | 646 | 46.3 | 684 | 49.1 |
| Sedentary | 378 | 27.2 | 352 | 25.3 |
| Mental health | ||||
| Normal | 800 | 57.5 | 763 | 54.8 |
| Borderline | 301 | 21.6 | 324 | 23.2 |
| Clinical | 292 | 20.9 | 306 | 22.0 |
| Watch TV | ||||
| No | 163 | 11.7 | 185 | 13.3 |
| Yes | 1230 | 88.3 | 1208 | 86.7 |
| TV use/week | ||||
| ≤2 times | 321 | 26.1 | 372 | 30.7 |
| ≥3 times | 909 | 73.9 | 836 | 69.3 |
| TV hours/day | ||||
| ≤2 h | 645 | 52.4 | 682 | 56.5 |
| ≥3 h | 585 | 47.6 | 526 | 43.5 |
| Use PC | ||||
| No | 264 | 19.0 | 354 | 25.4 |
| Yes | 1129 | 81.0 | 1039 | 74.6 |
| Computer type | ||||
| Desktop | 529 | 46.8 | 501 | 48.2 |
| Laptop | 600 | 53.2 | 538 | 51.8 |
| PC screen height | ||||
| Eyes aligned with the top of the screen | 291 | 25.7 | 268 | 25.7 |
| Eyes below the top of the screen | 838 | 74.3 | 771 | 74.3 |
| Distance from the eye to the PC screen | ||||
| ≤30 cm | 788 | 69.7 | 710 | 68.3 |
| ≥30 cm | 341 | 30.3 | 329 | 31.7 |
| PC use/week | ||||
| ≤2 times | 418 | 37.1 | 565 | 54.3 |
| ≥3 times | 711 | 69.9 | 474 | 45.6 |
| PC hours/day | ||||
| ≤2 h | 512 | 45.3 | 471 | 45.3 |
| ≥3 h | 671 | 59.4 | 568 | 54.6 |
| Cell phone use | ||||
| No | 34 | 2.4 | 44 | 3.1 |
| Yes | 1359 | 97.6 | 1349 | 96.9 |
| Posture during cell phone use * | ||||
| Standing | ||||
| No | 884 | 65.1 | 773 | 57.3 |
| Yes | 475 | 34.9 | 576 | 42.7 |
| Sitting | ||||
| No | 642 | 47.2 | 528 | 39.1 |
| Yes | 717 | 52.8 | 821 | 60.9 |
| Lying prone | ||||
| No | 563 | 41.4 | 464 | 34.4 |
| Yes | 796 | 58.6 | 885 | 65.6 |
| Semi-lying | ||||
| No | 898 | 66.0 | 802 | 59.4 |
| Yes | 461 | 34.0 | 547 | 40.6 |
| Cell phone hours/day | ||||
| ≤2 h | 301 | 22.1 | 305 | 22.6 |
| ≥3 h | 1058 | 77.9 | 1044 | 77.4 |
| Distance from the eye to the cell phone screen | ||||
| ≤20 cm | 1209 | 88.9 | 1169 | 86.6 |
| ≥20 cm | 150 | 11.1 | 180 | 13.4 |
| Tablet use | ||||
| No | 1120 | 80.4 | 1118 | 80.2 |
| Yes | 273 | 19.6 | 205 | 14.8 |
| Posture during tablet use * | ||||
| Standing | ||||
| No | 216 | 79.1 | 140 | 68.2 |
| Yes | 57 | 20.9 | 65 | 31.8 |
| Sitting | ||||
| No | 119 | 43.5 | 72 | 35.1 |
| Yes | 154 | 56.5 | 133 | 64.9 |
| Lying prone | ||||
| No | 148 | 54.2 | 98 | 47.8 |
| Yes | 125 | 45.8 | 107 | 52.2 |
| Semi-lying | ||||
| No | 210 | 76.9 | 139 | 67.8 |
| Yes | 66 | 24.1 | 66 | 32.2 |
| Tablet hours/day | ||||
| ≤2 h | 208 | 76.1 | 161 | 78.5 |
| ≥3 h | 65 | 23.9 | 44 | 21.6 |
| Distance from the eye to the tablet screen | ||||
| ≤20 cm | 221 | 80.9 | 174 | 84.8 |
| ≥20 cm | 52 | 19.1 | 31 | 15.2 |
| Factor | Ongoing TSP | |
|---|---|---|
| p-Value | RR (95% CI) * | |
| Sex | ||
| Male | 0.0001 | 1.00 |
| Female | 2.14 (1.64–2.77) | |
| Age | ||
| 14 years or younger | 0.04 | 1.00 |
| 15–18 years | 1.41 (1.01–2.00) | |
| Cell phone hours/day | ||
| ≤2 h | 0.001 | 1.00 |
| ≥3 h | 1.60 (1.21–2.13) | |
| Tablet hours/day | ||
| ≤2 h | 0.04 | 1.00 |
| ≥3 h | 2.08 (1.01–4.34) | |
| Sitting while using the tablet | ||
| No | 0.04 | 1.00 |
| Yes | 1.93 (1.24–1.93) | |
| Distance of the eye from the cell phone screen | ||
| ≤20 cm | 0.005 | 1.00 |
| ≥20 cm | 1.69 (1.17–2.50) | |
| Distance of the eye from the PC screen | ||
| ≤30 cm | 0.004 | 1.00 |
| ≥30 cm | 1.53 (1.14–2.04) | |
| Semi-lying prone position while using the cell phone | ||
| No | 0.003 | 1.00 |
| Yes | 1.47 (1.14–1.90) | |
| Mental health | ||
| Normal | 1.00 | |
| Borderline | 0.001 | 2.02 (1.48–2.76) |
| Clinical | 0.0001 | 3.07 (2.17–4.34) |
| Factor | Incidence of New TSP | |
|---|---|---|
| p-Value | RR (95% CI) * | |
| Sex | ||
| Male | 0.002 | 1.00 |
| Female | 1.88 (1.26–2.81) | |
| Cell phone hours/day | ||
| ≤2 h | 0.02 | 1.00 |
| ≥3 h | 1.72 (1.08–2.74) | |
| Semi-lying prone position while using cell phone | ||
| No | 0.005 | 1.00 |
| Yes | 1.71 (1.17–2.52) | |
| Semi-lying prone position while using tablet | ||
| No | 0.04 | 1.00 |
| Yes | 2.31 (1.02–5.24) | |
| Mental health | ||
| Normal | 1.00 | |
| Borderline | 0.003 | 2.07 (1.27–3.36) |
| Clinical | 0.0001 | 4.26 (2.63–6.89) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vitta, A.; Noll, M.; Monfort-Pañego, M.; Miñana-Signes, V.; Maciel, N.M. Thoracic Spine Pain in High School Adolescents: A One-Year Longitudinal Study. Healthcare 2023, 11, 196. https://doi.org/10.3390/healthcare11020196
De Vitta A, Noll M, Monfort-Pañego M, Miñana-Signes V, Maciel NM. Thoracic Spine Pain in High School Adolescents: A One-Year Longitudinal Study. Healthcare. 2023; 11(2):196. https://doi.org/10.3390/healthcare11020196
Chicago/Turabian StyleDe Vitta, Alberto, Matias Noll, Manuel Monfort-Pañego, Vicente Miñana-Signes, and Nicoly Machado Maciel. 2023. "Thoracic Spine Pain in High School Adolescents: A One-Year Longitudinal Study" Healthcare 11, no. 2: 196. https://doi.org/10.3390/healthcare11020196