

Diagnosis of Osteoporosis by Quantifying Volumetric Bone Mineral Density of Lumbar Vertebrae Using Abdominal CT Images and Two-Compartment Model

Abstract
:1. Introduction
2. Materials and Methods
2.1. Two-Compartment Model
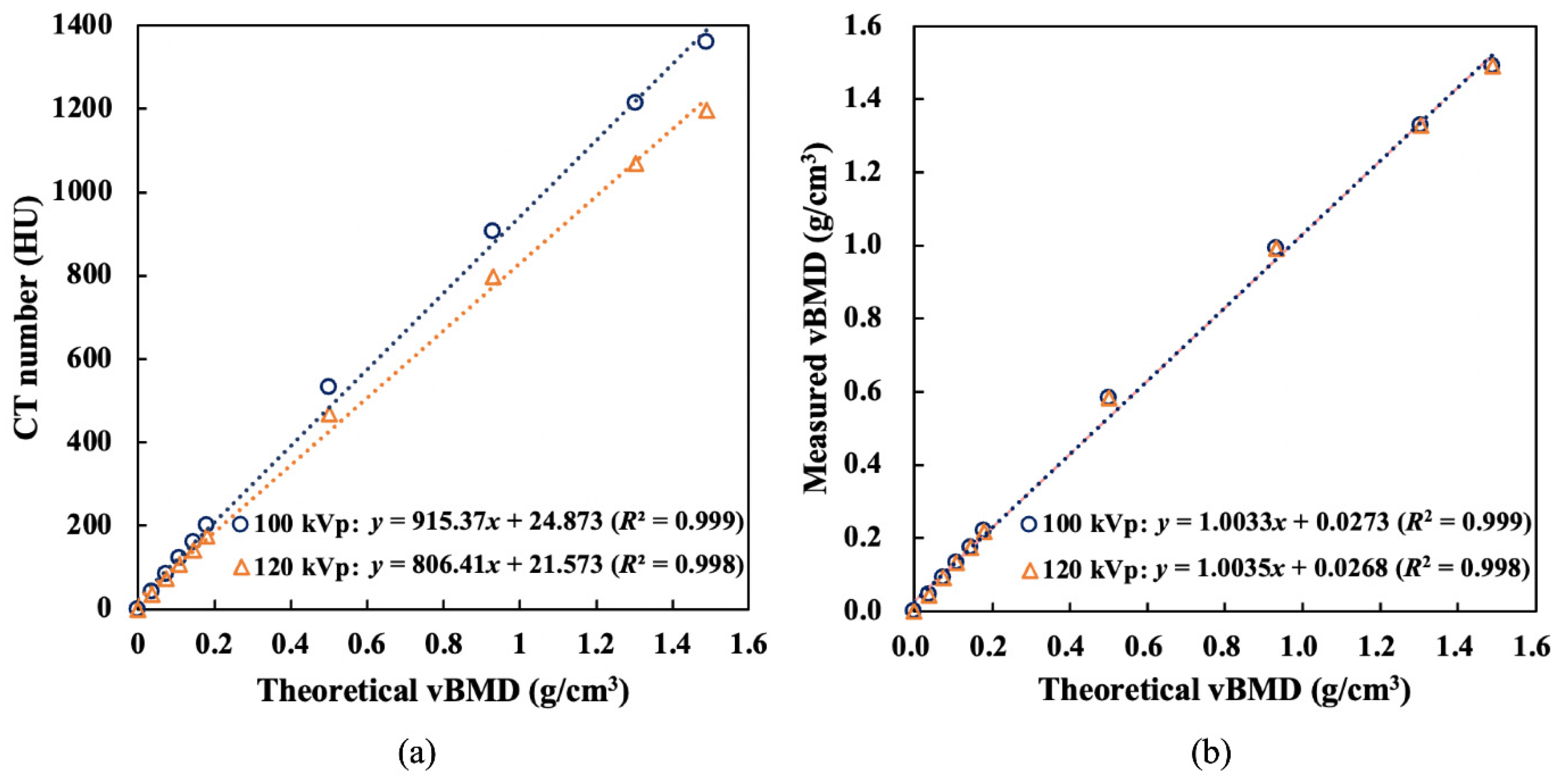
2.2. Phantom Validation for Different Tube Voltages
2.3. Patient Information
2.4. Analysis of DXA Data
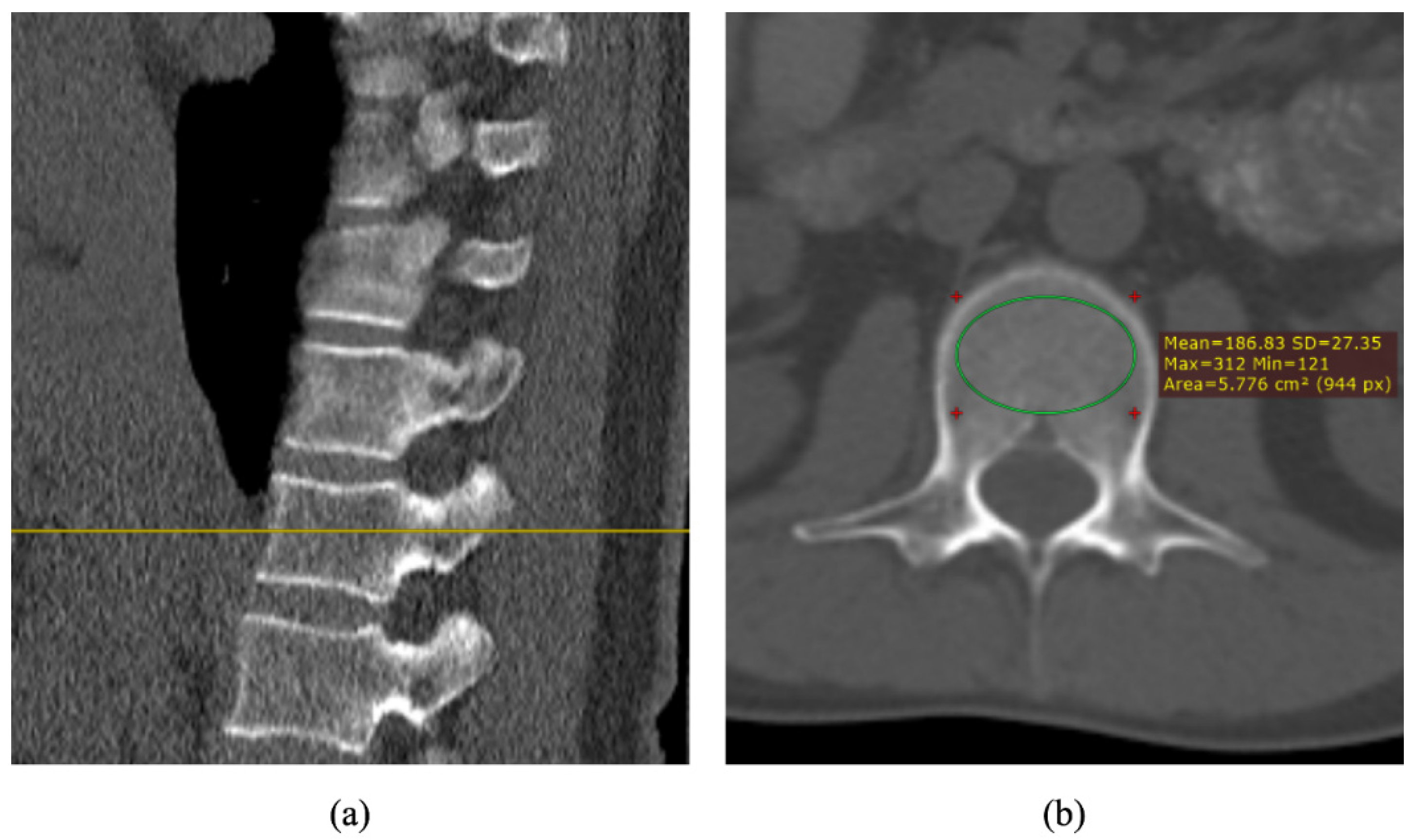
2.5. Analysis of CT Images
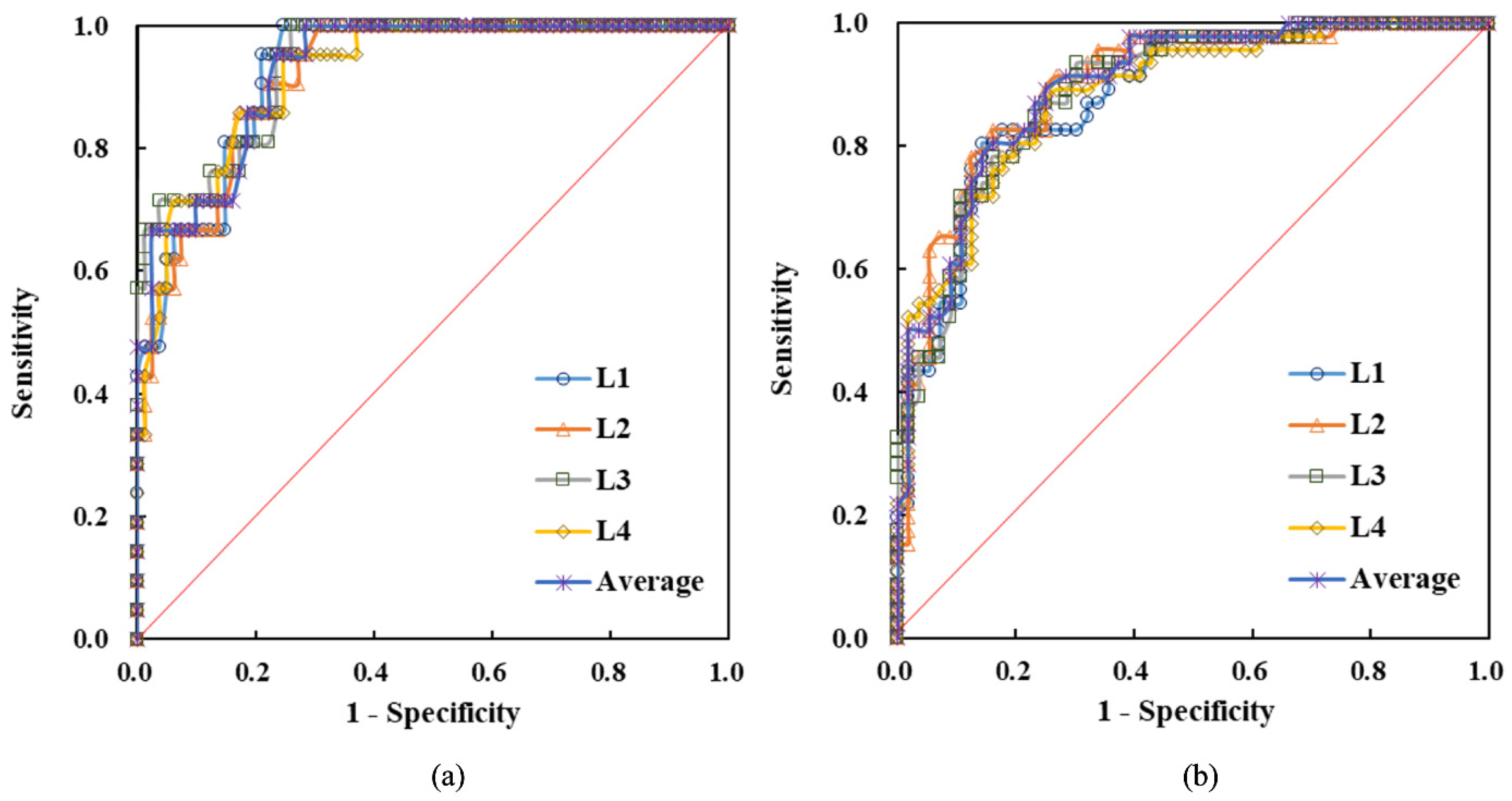
2.6. Receiver-Operating Characteristic Curve
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klotzbuecher, C.M.; Ross, P.D.; Landsman, P.B.; Abbott, T.A.; Berger, M. Patients with Prior Fractures Have an Increased Risk of Future Fractures: A Summary of the Literature and Statistical Synthesis. J. Bone Miner. Res. 2000, 15, 721–739. [Google Scholar] [CrossRef]
- Sözen, T.; Özışık, L.; Başaran, N. An Overview and Management of Osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Melton, L.J.; Chrischilles, E.A.; Cooper, C.; Lane, A.W.; Riggs, B.L. How Many Women Have Osteoporosis? J. Bone Miner. Res. 1992, 7, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J.; Atkinson, E.J.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Bone Density and Fracture Risk in Men. J. Bone Miner. Res. 1998, 13, 1915–1923. [Google Scholar] [CrossRef]
- Messina, C.; Albano, D.; Gitto, S.; Tofanelli, L.; Bazzocchi, A.; Ulivieri, F.M.; Guglielmi, G.; Sconfienza, L.M. Body Composition with Dual Energy X-Ray Absorptiometry: From Basics to New Tools. Quant. Imaging Med. Surg. 2020, 10, 1687–1698. [Google Scholar] [CrossRef] [PubMed]
- Milisic, L.; Vegar-Zubovic, S.; Valjevac, A.; Hasanovic-Vučković, S. Bone Mineral Density Assessment by DXA vs. QCT in Postmenopausal Females with Central Obesity. Curr. Aging Sci. 2020, 13, 153–161. [Google Scholar] [CrossRef]
- Kalkwarf, H.J.; Laor, T.; Bean, J.A. Fracture Risk in Children with a Forearm Injury Is Associated with Volumetric Bone Density and Cortical Area (by Peripheral QCT) and Areal Bone Density (by DXA). Osteoporos. Int. 2011, 22, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, M.; Abbasi-Rad, S.; Keyak, J.H.; Nabil, M.; Asadi, M.; Mobini, N.; Naghdi, P.; Emadi, H.; Saligheh Rad, H.; Shiran, M.B. Liquid Calibration Phantoms in Ultra-Low-Dose QCT for the Assessment of Bone Mineral Density. J. Clin. Densitom. 2020, 23, 108–116. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Pooler, B.D.; Lauder, T.; del Rio, A.M.; Bruce, R.J.; Binkley, N. Opportunistic Screening for Osteoporosis Using Abdominal Computed Tomography Scans Obtained for Other Indications. Ann. Intern. Med. 2013, 158, 588–595. [Google Scholar] [CrossRef]
- Lim, H.K.; Ha, H.I.; Park, S.Y.; Lee, K. Comparison of the Diagnostic Performance of CT Hounsfield Unit Histogram Analysis and Dual-Energy X-Ray Absorptiometry in Predicting Osteoporosis of the Femur. Eur. Radiol. 2018, 29, 1831–1840. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.L.; Wong, K.H.; Law, M.W.; Fang, B.X.; Lau, V.W.; Vardhanabuti, V.V.; Lee, V.K.; Cheng, A.K.; Ho, W.Y.; Lam, W.W. Opportunistic Screening for Osteoporosis in Abdominal Computed Tomography for Chinese Population. Arch. Osteoporos. 2018, 13, 76. [Google Scholar] [CrossRef]
- Perrier-Cornet, J.; Omorou, A.Y.; Fauny, M.; Loeuille, D.; Chary-Valckenaere, I. Opportunistic Screening for Osteoporosis Using Thoraco-Abdomino-Pelvic CT-Scan Assessing the Vertebral Density in Rheumatoid Arthritis Patients. Osteoporos. Int. 2019, 30, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Löffler, M.T.; Jacob, A.; Valentinitsch, A.; Rienmüller, A.; Zimmer, C.; Ryang, Y.M.; Baum, T.; Kirschke, J.S. Improved Prediction of Incident Vertebral Fractures Using Opportunistic QCT Compared to DXA. Eur. Radiol. 2019, 29, 4980–4989. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Triphuridet, N.; Yip, R.; Becker, B.J.; Wang, Y.; Yankelevitz, D.F.; Henschke, C.I. Opportunistic CT Screening of Osteoporosis on Thoracic and Lumbar Spine: A Meta-Analysis. Clin. Imaging 2021, 80, 382–390. [Google Scholar] [CrossRef]
- Liu, Y.L.; Hsu, J.T.; Shih, T.Y.; Luzhbin, D.; Tu, C.Y.; Wu, J. Quantification of Volumetric Bone Mineral Density of Proximal Femurs Using a Two-Compartment Model and Computed Tomography Images. Biomed. Res. Int. 2018, 2018, 6284269. [Google Scholar] [CrossRef]
- Ott, S.M. Cortical or Trabecular Bone: What’s the Difference? Am. J. Nephrol. 2018, 47, 373–375. [Google Scholar] [CrossRef]
- Lin, H.; Peng, S.; Wu, J.; Shih, T.; Chuang, K.; Shih, C. A Novel Two-Compartment Model for Calculating Bone Volume Fractions and Bone Mineral Densities from Computed Tomography Images. IEEE Trans. Med. Imaging 2017, 36, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Pasoto, S.G.; Augusto, K.L.; Alvarenga, J.C.; Takayama, L.; Oliveira, R.M.; Bonfa, E.; Pereira, R.M.R. Cortical Bone Density and Thickness Alterations by High-Resolution Peripheral Quantitative Computed Tomography: Association with Vertebral Fractures in Primary Sjögren’s Syndrome. Rheumatology 2016, 55, 2200–2211. [Google Scholar] [CrossRef]
- Hansen, K.E.; Vallarta-Ast, N.; Krueger, D.; Gangnon, R.; Drezner, M.K.; Binkley, N. Use of the Lowest Vertebral Body T-score to Diagnose Lumbar Osteoporosis in Men: Is “Cherry Picking” Appropriate? J. Clin. Densitom. 2004, 7, 376–381. [Google Scholar] [CrossRef]
- Ardawi, M.S.; Maimany, A.A.; Bahksh, T.M.; Nasrat, H.A.; Milaat, W.A.; Al-Raddadi, R.M. Bone Mineral Density of the Spine and Femur in Healthy Saudis. Osteoporos. Int. 2005, 16, 43–55. [Google Scholar] [CrossRef]
- Shih, C.T.; Wu, J. Converting Computed Tomography Images into Photon Interaction Coefficients by Using Stoichiometric Calibration and Parametric Fit Models. Med. Phys. 2017, 44, 510–521. [Google Scholar] [CrossRef]
- Das, I.J.; Cheng, C.W.; Cao, M.; Johnstone, P.A. Computed Tomography Imaging Parameters for Inhomogeneity Correction in Radiation Treatment Planning. J. Med. Phys. 2016, 41, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Nakao, M.; Ozawa, S.; Yamada, K.; Yogo, K.; Hosono, F.; Hayata, M.; Saito, A.; Miki, K.; Nakashima, T.; Ochi, Y.; et al. Tolerance Levels of CT Number to Electron Density Table for Photon Beam in Radiotherapy Treatment Planning System. J. Appl. Clin. Med. Phys. 2018, 19, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Zou, D.; Li, W.; Deng, C.; Du, G.; Xu, N. The Use of CT Hounsfield Unit Values to Identify the Undiagnosed Spinal Osteoporosis in Patients with Lumbar Degenerative Diseases. Eur. Spine J. 2018, 28, 1758–1766. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Lee, L.J.; del Rio, A.M.; Lauder, T.; Bruce, R.J.; Summers, R.M.; Pooler, B.D.; Binkley, N. Simultaneous Screening for Osteoporosis at CT Colonography: Bone Mineral Density Assessment Using Mdct Attenuation Techniques Compared with the Dxa Reference Standard. J. Bone Miner. Res. 2011, 26, 2194–2203. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.X.; Yu, Q. Primary Osteoporosis in Postmenopausal Women. Chronic Dis. Transl. Med. 2015, 1, 9–13. [Google Scholar] [CrossRef]
- Cui, L.H.; Choi, J.S.; Shin, M.H.; Kweon, S.S.; Park, K.S.; Lee, Y.H.; Nam, H.S.; Jeong, S.K.; Im, J.S. Prevalence of Osteoporosis and Reference Data for Lumbar Spine and Hip Bone Mineral Density in a Korean Population. J. Bone Miner. Metab. 2008, 26, 609–617. [Google Scholar] [CrossRef]
- Emohare, O.; Cagan, A.; Morgan, R.; Davis, R.; Asis, M.; Switzer, J.; Polly, D.W. The Use of Computed Tomography Attenuation to Evaluate Osteoporosis Following Acute Fractures of the Thoracic and Lumbar Vertebra. Geriatr. Orthop. Surg. Rehabil. 2014, 5, 50–55. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Cohort | Test Cohort | |||||
|---|---|---|---|---|---|---|
| Normal | Osteopenia | Osteoporosis | Normal | Osteopenia | Osteoporosis | |
| Gender (F:M) | 23:34 | 16:9 | 22:1 | 17:26 | 12:6 | 11:3 |
| Age (y) | 47.4 ± 11.3 | 55.9 ± 9.9 | 64.6 ± 9.1 | 46.6 ± 10.3 | 52.8 ± 10.1 | 64.6 ± 6.7 |
| BMI (kg/m2) | 23.5 ± 3.4 | 24.2 ± 4.3 | 23.7 ± 2.6 | 24.9 ± 4.4 | 23.9 ± 4.6 | 22.4 ± 4.2 |
| aBMD (g/cm2) | ||||||
| L1 | 1.117 ± 0.110 | 0.936 ± 0.069 | 0.796 ± 0.071 | 1.142 ± 0.127 | 0.901 ± 0.086 | 0.744 ± 0.114 |
| L2 | 1.234 ± 0.121 | 1.025 ± 0.080 | 0.825 ± 0.086 | 1.247 ± 0.145 | 0.952 ± 0.077 | 0.776 ± 0.120 |
| L3 | 1.314 ± 0.128 | 1.096 ± 0.075 | 0.931 ± 0.120 | 1.334 ± 0.159 | 1.048 ± 0.061 | 0.892 ± 0.148 |
| L4 | 1.320 ± 0.153 | 1.127 ± 0.078 | 0.960 ± 0.085 | 1.323 ± 0.169 | 1.068 ± 0.096 | 0.917 ± 0.138 |
| Average | 1.246 ± 0.152 | 1.046 ± 0.105 | 0.879 ± 0.114 | 1.262 ± 0.168 | 0.992 ± 0.105 | 0.832 ± 0.147 |
| T-score | ||||||
| L1 | 0.5 ± 0.9 | −1.2 ± 0.6 | −2.6 ± 0.5 | 0.7 ± 1.1 | −1.3 ± 0.7 | −3.0 ± 1.0 |
| L2 | 0.9 ± 1.0 | −1.0 ± 0.7 | −2.9 ± 0.6 | 1.0 ± 1.2 | −1.5 ± 0.6 | −3.4 ± 1.1 |
| L3 | 1.4 ± 1.1 | −0.5 ± 0.6 | −2.1 ± 0.9 | 1.6 ± 1.3 | −0.8 ± 0.5 | −2.4 ± 1.2 |
| L4 | 1.5 ± 1.2 | −0.3 ± 0.7 | −1.8 ± 0.7 | 1.6 ± 1.4 | −0.6 ± 0.8 | −2.2 ± 1.2 |
| Average | 1.1 ± 1.1 | −0.8 ± 0.8 | −2.3 ± 0.8 | 1.2 ± 1.3 | −1.1 ± 0.7 | −2.8 ± 1.2 |
| Threshold (g/cm3) | AUC | Sensitivity (%) | Specificity (%) | Accuracy (%) | |
|---|---|---|---|---|---|
| Osteoporosis | |||||
| L1 | ≤0.121 | 0.928 | 95.7 | 78.0 | 81.9 |
| L2 | ≤0.103 | 0.921 | 87.0 | 81.7 | 82.9 |
| L3 | ≤0.107 | 0.937 | 87.0 | 76.8 | 79.0 |
| L4 | ≤0.114 | 0.924 | 95.7 | 75.6 | 80.0 |
| Average | ≤0.116 | 0.930 | 95.7 | 75.6 | 80.0 |
| Osteopenia | |||||
| L1 | ≤0.134 | 0.883 | 81.3 | 84.2 | 82.9 |
| L2 | ≤0.125 | 0.901 | 83.3 | 82.5 | 84.6 |
| L3 | ≤0.129 | 0.889 | 83.3 | 75.4 | 79.8 |
| L4 | ≤0.141 | 0.884 | 89.6 | 73.7 | 81.7 |
| Average | ≤0.126 | 0.897 | 81.3 | 82.5 | 82.7 |
| Sensitivity (%) | Specificity (%) | Accuracy (%) | |
|---|---|---|---|
| Osteoporosis | |||
| L1 | 100.0 | 75.4 | 80.0 |
| L2 | 85.7 | 83.6 | 84.0 |
| L3 | 100.0 | 72.1 | 77.3 |
| L4 | 85.7 | 75.4 | 77.3 |
| Average | 100.0 | 73.8 | 78.7 |
| Osteopenia | |||
| L1 | 84.4 | 83.7 | 84.0 |
| L2 | 81.3 | 83.7 | 82.7 |
| L3 | 81.3 | 79.1 | 80.0 |
| L4 | 87.5 | 72.1 | 78.7 |
| Average | 81.3 | 83.7 | 82.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Luzhbin, D.; Shih, T.-Y.; Wu, J. Diagnosis of Osteoporosis by Quantifying Volumetric Bone Mineral Density of Lumbar Vertebrae Using Abdominal CT Images and Two-Compartment Model. Healthcare 2023, 11, 556. https://doi.org/10.3390/healthcare11040556
Hsu P-C, Luzhbin D, Shih T-Y, Wu J. Diagnosis of Osteoporosis by Quantifying Volumetric Bone Mineral Density of Lumbar Vertebrae Using Abdominal CT Images and Two-Compartment Model. Healthcare. 2023; 11(4):556. https://doi.org/10.3390/healthcare11040556
Chicago/Turabian StyleHsu, Po-Chieh, Dmytro Luzhbin, Tia-Yu Shih, and Jay Wu. 2023. "Diagnosis of Osteoporosis by Quantifying Volumetric Bone Mineral Density of Lumbar Vertebrae Using Abdominal CT Images and Two-Compartment Model" Healthcare 11, no. 4: 556. https://doi.org/10.3390/healthcare11040556