
Effects of a Mindfulness and Physical Activity Programme on Anxiety, Depression and Stress Levels in People with Mental Health Problems in a Prison: A Controlled Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Method
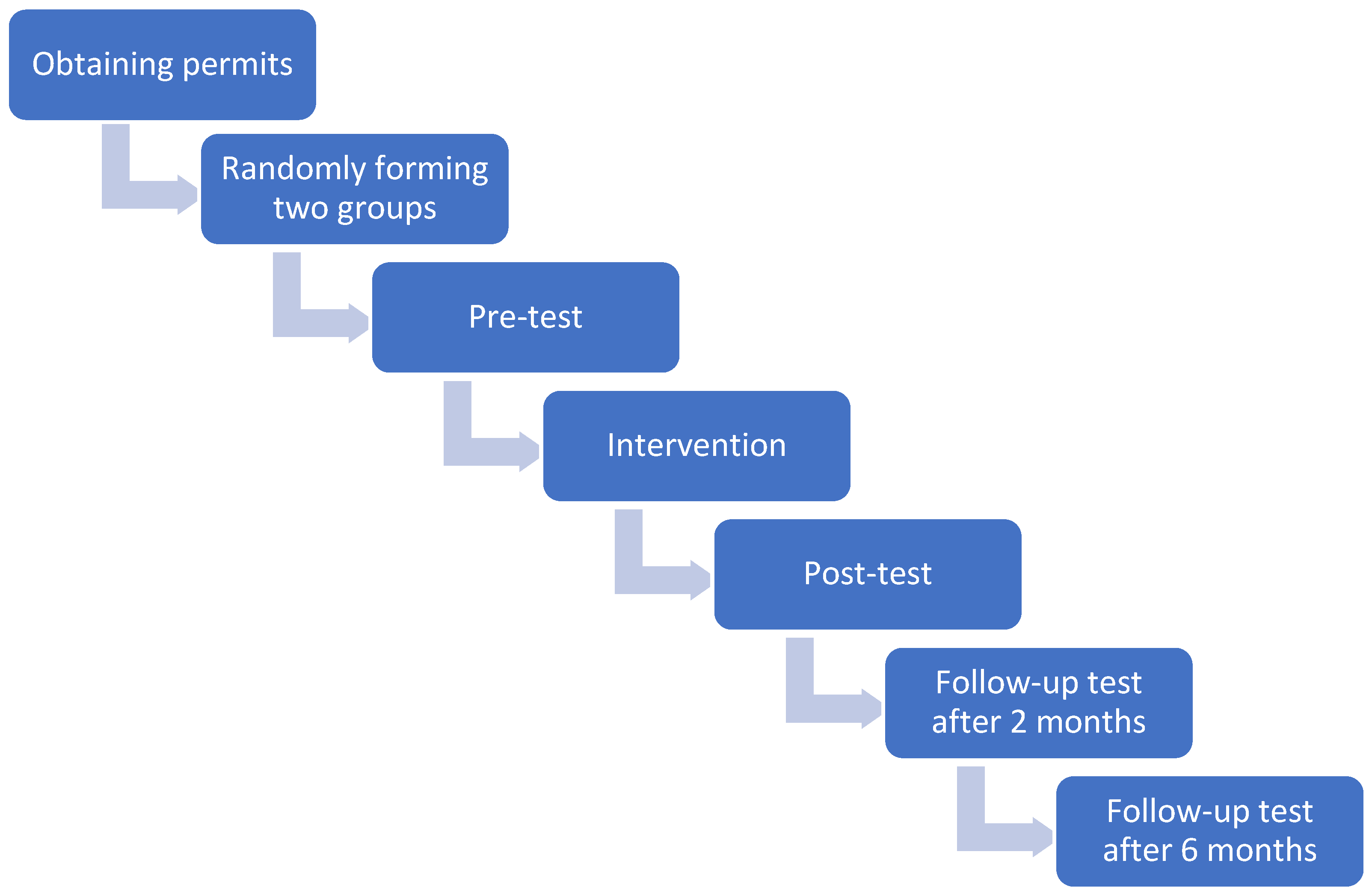
2.1. Design
2.2. Participants
- Belonging to the PIAMI programme of the El Acebuche prison in Almería.
- Availability of the inmate throughout the study, i.e., not being close to release.
- Not presenting behavioural reports for inappropriate behaviour (internal prison measure for the enjoyment of unofficial activities), i.e., being among the inmates with the best behaviour.
- Understanding of the language.
2.3. Instruments
2.4. Procedure
2.5. Sport Group
2.6. Mindfulness Group
2.7. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.H.-W.; Lui, D.; Chan, H.; Sum, K.; Cheung, A.; Yip, H.; Yu, C.H. Effects of mindfulness-based intervention programs on sleep among people with common mental disorders: A systematic review and meta-analysis. World J. Psychiatry 2022, 12, 636–650. [Google Scholar] [CrossRef] [PubMed]
- Khoury, B.; Lecomte, T.; Gaudiano, B.A.; Paquin, K. Mindfulness interventions for psychosis: A meta-analysis. Schizophr. Res. 2013, 150, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Louise, S.; Fitzpatrick, M.; Strauss, C.; Rossell, S.L.; Thomas, N. Mindfulness- and acceptance-based interventions for psychosis: Our current understanding and a meta-analysis. Schizophr. Res. 2018, 192, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Langer, I.; Cangas, A.J.; Salcedo, E.; Fuentes, B. Applying Mindfulness Therapy in a Group of Psychotic Individuals: A Controlled Study. Behav. Cogn. Psychother. 2012, 40, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Buckaloo, B.J.; Krug, K.S.; Nelson, K.B. Exercise and the Low-Security Inmate: Changes in Depression, Stress, and Anxiety. Prison J. 2009, 89, 328–343. [Google Scholar] [CrossRef]
- Li, Y.; Wen, Z.; He, Y.; Huang, J. Mental health status among prison officers in the process of enforcing the law during COVID-19 epidemic: A cross-sectional survey from China. BMC Psychiatry 2022, 22, 33. [Google Scholar] [CrossRef] [PubMed]
- Pereda Azofra, A. El deporte como medio de rehabilitación y reinserción social. Rev. Electrónica Derecho Univ. Rioja. 2016, 14, 257–294. [Google Scholar] [CrossRef]
- Auty, K.M.; Cope, A.; Liebling, A. A Systematic Review and Meta-Analysis of Yoga and Mindfulness Meditation in Prison: Effects on Psychological Well-Being and Behavioural Functioning. Int. J. Offender Ther. Comp. Criminol. 2017, 61, 689–710. [Google Scholar] [CrossRef]
- García-Jarillo, M.; Caravaca-Sánchez, F.; Sánchez-Alcaraz, C.; Luna, A. Psychosocial stressors perceived in the process of social reintegration and compliance time remaining in prison sentence. Rev. Española Sanid. Penit. 2016, 18, 49–95. Available online: https://web.archive.org/web/20200323024408id_/http://scielo.isciii.es/pdf/sanipe/v18n2/03_original2.pd (accessed on 10 November 2022).
- Worley, R.M.; Lambert, E.G.; Worley, V.B. Can’t Shake the Prison Guard Blues: Examining the Effects of Work Stress, Job Satisfaction, Boundary Violations, and the Mistreatment of Inmates on the Depressive Symptomatology of Correctional Officers. Crim. Justice Rev. 2022. [Google Scholar] [CrossRef]
- Delgado Salazar, C.; Mateus Aguliera, E.; Rincón Bolivar, L.; Villamil Parra, W. Efectos del ejercicio físico sobre la depresión y la ansiedad. Rev. Colomb. Rehabil. 2019, 18, 128–145. [Google Scholar] [CrossRef]
- Salazar, C.F.D.; Aguliera, E.T.M.; Bolivar, L.A.R.; Parra, W.A.V. Reduced trauma symptoms and perceived stress in male prison innates through the Transcendental Meditation program: A randomized controlled trial. Perm. J. 2016, 20, 43–47. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Mendoza, I.; Olivas-Ugarte, L.O.; De La Cruz-Valdiviano, C. Escalas abreviadas de Depresión, Ansiedad y Estrés (DASS-21): Validez, fiabilidad y equidad en adolescentes peruanos. Rev. Psicol. Clínica Niños Adolesc. 2021, 8, 24–30. [Google Scholar] [CrossRef]
- Mullor, D.; Cangas, A.J.; Gallego, J.; Aguilar-Parra, J.M.; Rosado, A.; López, A. A longitudinal study about the impact of an inclusive sports program in people with a diagnosis of schizophrenia. Psychosis 2019, 11, 75–84. [Google Scholar] [CrossRef]
- Kabat- Zinn, J. Full catastrophe living. In Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Hayes, S.C.; McCurry, S.M.; Afari, N.; Wilson, K. Acceptance and commitment therapy (ACT). In A Manual for the TREATMENT of Emotional Avoidance; Context Press: Reno, NV, USA, 1991. [Google Scholar]
- Wilson, K.G.; Luciano, C. Terapia de Aceptación y Compromiso: Un Tratamiento Conductual Orientado a Los Valores; Pirámide: Madrid, New Mexico, 2002. [Google Scholar]
- Ahmad, F.; El Morr, C.; Ritvo, P.; Othman, N.; Moineddin, R.; MVC Team. An eight-week, web-based mindfulness virtual community intervention for students’ mental health: Randomized controlled trial. JMIR Ment. Health 2020, 7, e15520. [Google Scholar] [CrossRef]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef]
- Rosenthal, R. Meta-Analytic Procedures for Social Research; SAGE Publications: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Lyons, T.; Womack, V.Y.; Cantrell, W.D.; Kenemore, T. Mindfulness-Based Relapse Prevention in a Jail Drug Treatment Program. Subst. Use Misuse 2019, 54, 57–64. [Google Scholar] [CrossRef]
- Zdemir, A.A.; Kavak Budak, F. The effects of mindfulness-based stress reduction training on hope, psychological well-being, and functional recovery in patients with schizophrenia. Clin. Nurs. Res. 2022, 31, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Barnert, E.S.; Himelstein, S.; Herbert, S.; Garcia-Romeu, A.; Chamberlain, L.J. Exploring an intensive meditation intervention for incarcerated youth. Child Adolesc. Ment. Heath 2014, 19, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Le, T.N.; Proulx, J. Feasibility of mindfulness-based intervention for incarcerated mixed-ethnic Native Hawaiian/Pacific Islander youth. Asian Am. J. Psychol. 2015, 6, 181–189. [Google Scholar] [CrossRef]
- Carmo, C.; Iacob, V.; Brás, M.; Fernandes, J. Effects of a Mindfulness-Based Intervention on Male Portuguese Prisoners. Int. J. Offender Ther. Comp. Criminol. 2022. [Google Scholar] [CrossRef]
- OECD. Health at a Glance; OECD Publishing: Paris, France, 2019. [Google Scholar]
- World Health Organization. Health-Promoting Sports Clubs National Audit Tool (No. WHO/EURO: 2022-5216-44980-64040); World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]


{kind=link}
| Consume | Diagnosis | Age |
|---|---|---|
| Sporadic hashish | Schizophrenia | 47 |
| Hashish | Paranoid Schizophrenia | 42 |
| Alcohol | Schizophrenia | 39 |
| Hashish, cocaine sporadically | Narcissistic Disorder and Suicide Prevention | 24 |
| No consumption | Bipolar Disorder | 53 |
| No consumption | Bipolar Disorder | 38 |
| No consumption | Schizophrenia | 51 |
| No consumption | Schizophrenia | 54 |
| Hashish | Major Depressive Disorder and Antisocial Personality Disorder | 52 |
| No consumption | Delusional Disorder | 46 |
| No consumption | Schizophrenia and Pigmentary Glaucoma | 39 |
| Consume | Diagnosis | Age |
|---|---|---|
| No consumption | Personality disorder not specified | 55 |
| No consumption | Schizophrenia | 41 |
| Hashish, heroin, cocaine | Schizophrenia | 34 |
| No consumption | Schizophrenia | 44 |
| No consumption | Depression | 45 |
| Hashish, heroin, cocaine | Schizophrenia | 40 |
| Ecstasy, hashish, alcohol | Schizophrenia | 20 |
| Cocaine | Schizophrenia | 38 |
| Cocaine | Schizophrenia | 39 |
| No consumption | Schizophrenia | 58 |
| No consumption | Personality disorder not specified | 41 |
| Friedman | Wilcoxon | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| M | Sig. | X2 | Sig. | Z | r | ||||
| Depression | Sport | Pretest | 15.82 | 0.309 | 3.594 | Pre-post | 0.959 | −0.051 | −0.011 |
| Post-test | 14.55 | Pre-segto2 | 0.066 | −1.837 | −0.392 | ||||
| Segto.2 | 7.18 | Pre-segto6 | 0.262 | −1.122 | −0.239 | ||||
| Segto.6 | 12.00 | Post-segto2 | 0.036 | −2.092 | −0.446 | ||||
| Post-segto6 | 0.722 | −0.356 | −0.076 | ||||||
| Segto-segto6 | 0.130 | −1.512 | −0.322 | ||||||
| Mindfulness | Pretest | 16.36 | 0.100 | 6.241 | Pre-post | 0.474 | −0.715 | −0.152 | |
| Post-test | 14.00 | Pre-segto2 | 0.017 | −2.383 | −0.533 | ||||
| Segto.2 | 7.11 | Pre-segto6 | 0.208 | −1.260 | −0.282 | ||||
| Segto.6 | 10.89 | Post-segto2 | 0.080 | −1.752 | −0.392 | ||||
| Post-segto6 | 0.593 | −0.534 | −0.119 | ||||||
| Segto-segto6 | 0.084 | −1.725 | −0.407 | ||||||
| Anxiety | Sport | Pretest | 10.73 | 0.067 | 7.160 | Pre-post | 0.411 | −0.821 | −0.175 |
| Post-test | 14.36 | Pre-segto2 | 0.229 | −1.202 | −0.256 | ||||
| Segto.2 | 7.64 | Pre-segto6 | 0.246 | −1.159 | −0.247 | ||||
| Segto.6 | 13.09 | Post-segto2 | 0.013 | −2.492 | −0.531 | ||||
| Post-segto6 | 0.959 | −0.051 | −0.011 | ||||||
| Segto-segto6 | 0.008 | −2.670 | −0.569 | ||||||
| Mindfulness | Pretest | 13.78 | 0.230 | 4.310 | Pre-post | 0.799 | −0.254 | −0.054 | |
| Post-test | 12.67 | Pre-segto2 | 0.103 | −1.628 | −0.364 | ||||
| Segto.2 | 8.00 | Pre-segto6 | 0.953 | −0.059 | −0.013 | ||||
| Segto.6 | 11.89 | Post-segto2 | 0.036 | −2.094 | −0.468 | ||||
| Post-segto6 | 0.943 | −0.071 | −0.016 | ||||||
| Segto-segto6 | 0.066 | −1.840 | −0.434 | ||||||
| Stress | Sport | Pretest | 11.82 | 0.140 | 5.477 | Pre-post | 0.202 | −1.276 | −0.272 |
| Post-test | 17.45 | Pre-segto2 | 0.284 | −1.071 | −0.228 | ||||
| Segto.2 | 8.64 | Pre-segto6 | 0.372 | −0.892 | −0.190 | ||||
| Segto.6 | 13.18 | Post-segto2 | 0.026 | −2.225 | −0.474 | ||||
| Post-segto6 | 0.477 | −0.711 | −0.152 | ||||||
| Segto-segto6 | 0.099 | −1.647 | −0.351 | ||||||
| Mindfulness | Pretest | 16.44 | 0.032 | 8.793 | Pre-post | 0.009 | −2.609 | −0.556 | |
| Post-test | 9.33 | Pre-segto2 | 0.011 | −2.533 | −0.567 | ||||
| Segto.2 | 7.78 | Pre-segto6 | 0.109 | −1.602 | −0.358 | ||||
| Segto.6 | 10.56 | Post-segto2 | 0.675 | −0.419 | −0.094 | ||||
| Post-segto6 | 0.514 | −0.653 | −0.146 | ||||||
| Segto-segto6 | 0.261 | −1.123 | −0.265 | ||||||
| Depression Pretest | Anxiety Pretest | Stress Pretest | Total Pretest | Depression Post-Test | Anxiety Post-Test | Stress Post-Test | Total Post-Test | |
|---|---|---|---|---|---|---|---|---|
| U Mann–Whitney | 59.50 | 56.00 | 41.00 | 56.50 | 60.00 | 47.00 | 36.00 | 50.50 |
| W from Wilcoxon | 125.50 | 122.00 | 107.00 | 122.50 | 126.00 | 113.00 | 102.00 | 116.50 |
| Z | −0.066 | −0.298 | −1.286 | −0.263 | −0.033 | −0.894 | −0.614 | −0.657 |
| p | 0.947 | 0.766 | 0.199 | 0.792 | 0.974 | 0.372 | 0.106 | 0.511 |
| r | −0.014 | −0.063 | −0.274 | −0.056 | −0.007 | −0.190 | −0.344 | −0.140 |
| Depression Segto.2 | Anxiety Segto.2 | Stress Segto.2 | Total Segto.2 | Depression Segto.6 | Anxiety Segto.6 | Stress Segto.6 | Total Segto.6 | |
|---|---|---|---|---|---|---|---|---|
| U Mann–Whitney | 47.00 | 49.50 | 45.50 | 48.00 | 41.00 | 35.50 | 33.50 | 34.50 |
| W de Wilcoxon | 92.00 | 94.50 | 90.50 | 93.00 | 86.00 | 80.50 | 78.50 | 79.50 |
| Z | −0.192 | 0.000 | −0.305 | −0.114 | −0.655 | −1.085 | −0.236 | −0.142 |
| p | 0.848 | 0.000 | 0.760 | 0.909 | 0.513 | 0.278 | 0.216 | 0.253 |
| r | −0.042 | 0.000 | −0.068 | −0.025 | −0.146 | −0.242 | −0.276 | −0.255 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallego, J.; Cangas, A.J.; Mañas, I.; Aguilar-Parra, J.M.; Langer, Á.I.; Navarro, N.; Lirola, M.-J. Effects of a Mindfulness and Physical Activity Programme on Anxiety, Depression and Stress Levels in People with Mental Health Problems in a Prison: A Controlled Study. Healthcare 2023, 11, 555. https://doi.org/10.3390/healthcare11040555
Gallego J, Cangas AJ, Mañas I, Aguilar-Parra JM, Langer ÁI, Navarro N, Lirola M-J. Effects of a Mindfulness and Physical Activity Programme on Anxiety, Depression and Stress Levels in People with Mental Health Problems in a Prison: A Controlled Study. Healthcare. 2023; 11(4):555. https://doi.org/10.3390/healthcare11040555
Chicago/Turabian StyleGallego, Jose, Adolfo J. Cangas, Israel Mañas, Jose M. Aguilar-Parra, Álvaro I. Langer, Noelia Navarro, and Maria-Jesus Lirola. 2023. "Effects of a Mindfulness and Physical Activity Programme on Anxiety, Depression and Stress Levels in People with Mental Health Problems in a Prison: A Controlled Study" Healthcare 11, no. 4: 555. https://doi.org/10.3390/healthcare11040555