
Association between Socioeconomic Status and Healthcare Utilization for Children with Allergic Diseases: Korean National Health and Nutritional Examination Survey (2015–2019)


Abstract
:1. Introduction
2. Materials and Methods
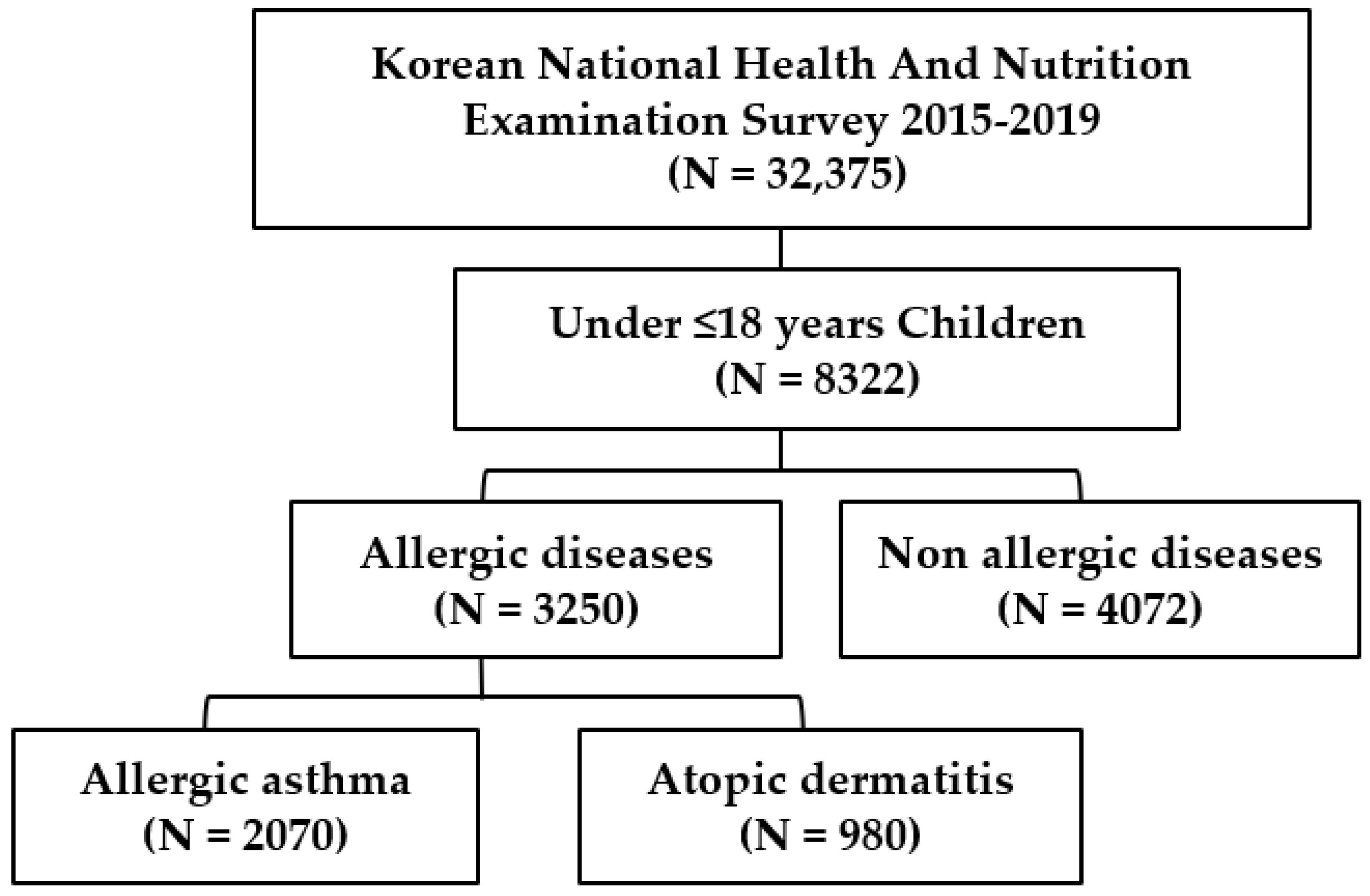
2.1. Data Source and Study Population
2.2. Variables and Measurement
2.2.1. The Dependent Variable
2.2.2. Independent Variable
2.3. Statistical Analysis
3. Results
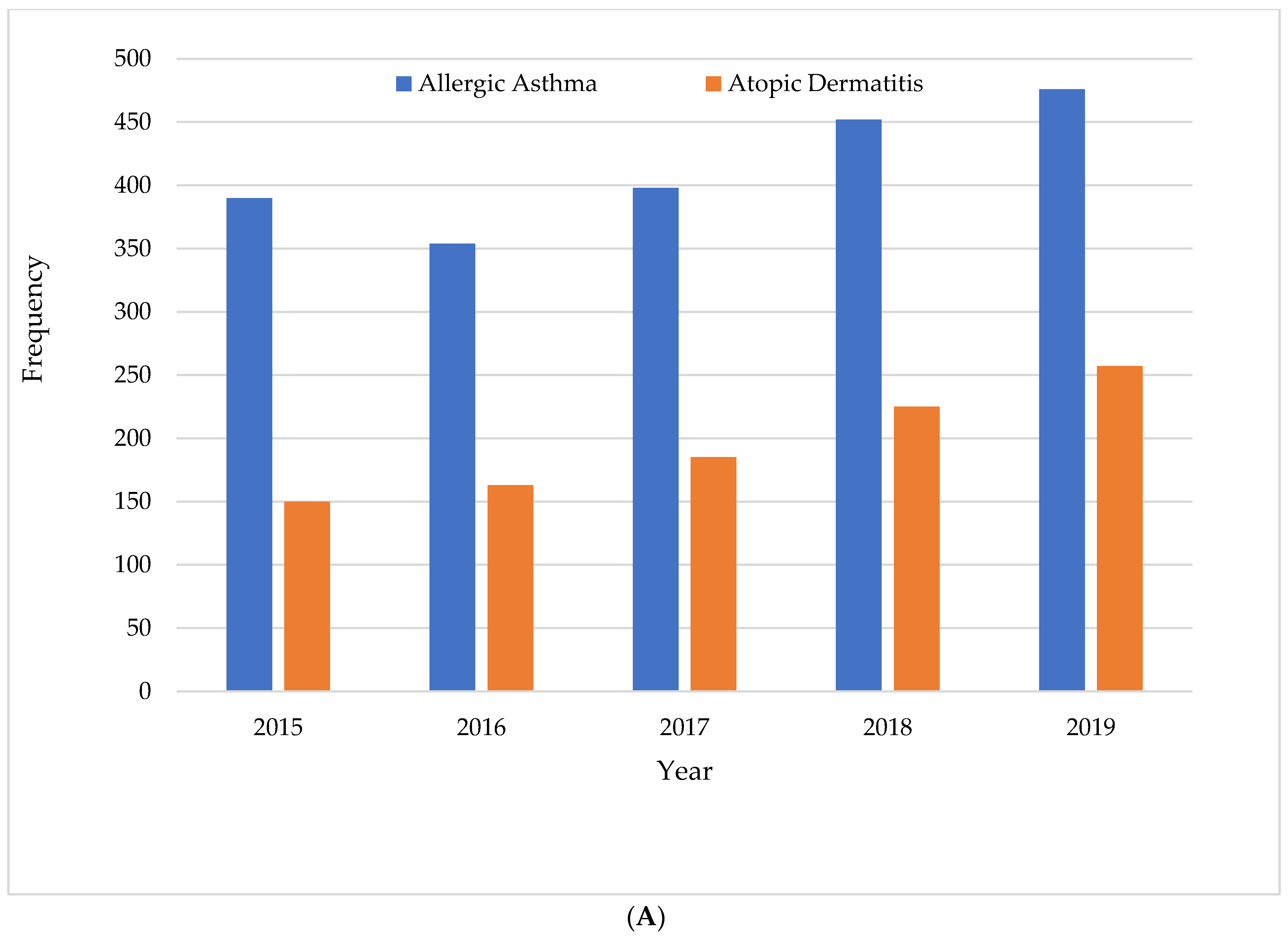
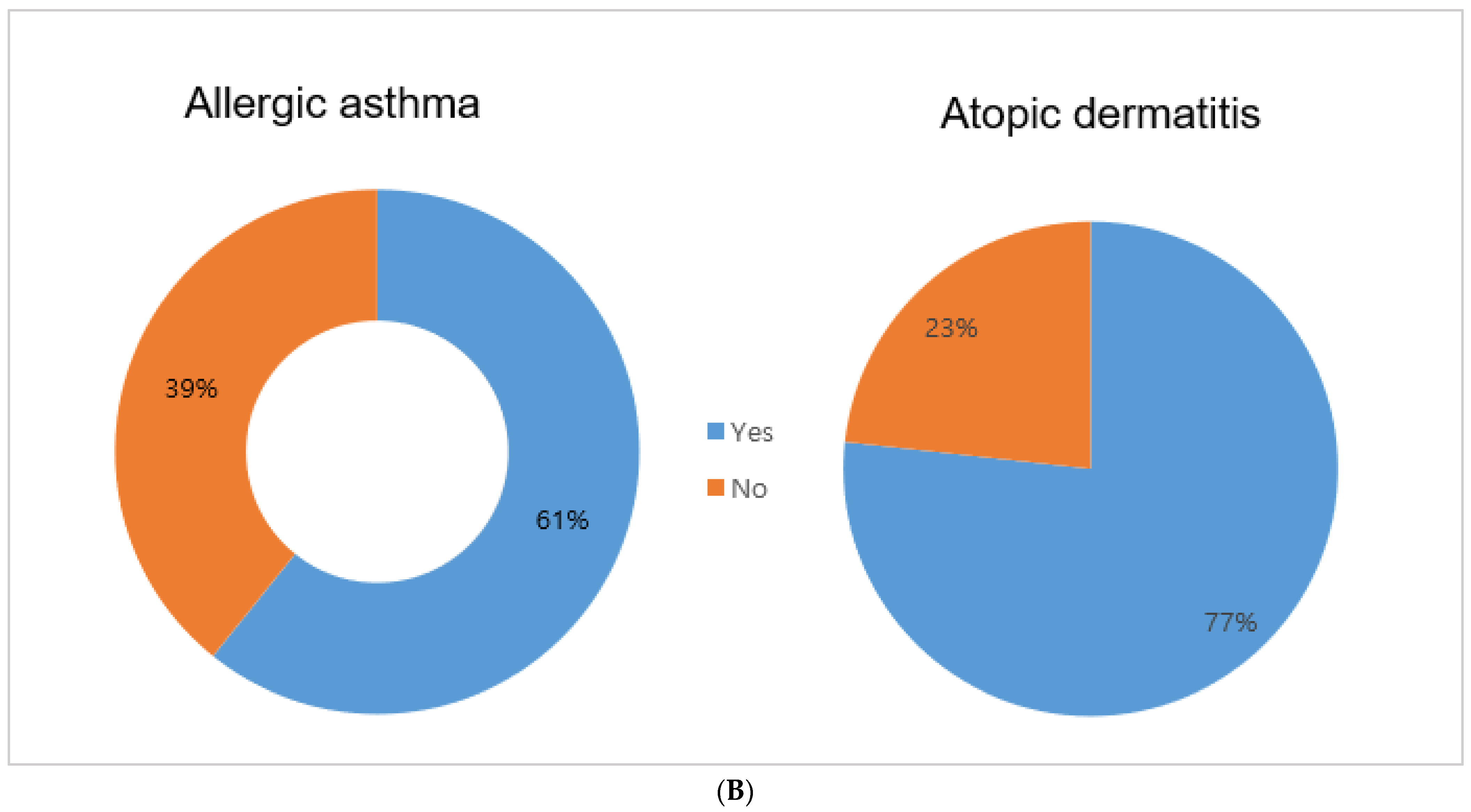
3.1. Study Population and Distribution of Allergic Diseases among Korean Children
3.2. Characteristics of Study Children with Allergic Diseases
3.3. Multivariate Logistic Regression Analysis of Factors Associated with Healthcare Utilization for Children with Allergic Diseases
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pawankar, R. Allergic diseases and asthma: A global public health concern and a call to action. World Allergy Organ. J. 2014, 7, 12. [Google Scholar] [PubMed]
- Sol, I.S.; Kim, Y.H.; Kim, S.Y.; Choi, S.H.; Kim, J.D.; Kim, B.O.; Moon, J.E.; Kim, K.W.; Sohn, M.H. Prescription patterns and burden of pediatric asthma in Korea. Allergy Asthma Immunol. Res. 2019, 11, 280–290. [Google Scholar]
- Song, W.-J.; Wong, G.W. Changing trends and challenges in the management of asthma in Asia. J. Allergy Clin. Immunol. 2017, 140, 1272–1274. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Kim, J.Y.; Kang, M.K.; Yang, M.S.; Park, H.W.; Min, K.U.; Cho, S.H.; Kang, H.R. Allergies are still on the rise? A 6-year nationwide population-based study in Korea. Allergol. Int. 2016, 65, 186–191. [Google Scholar] [PubMed]
- Cho, Y.M.; Kim, C.-B.; Yeon, K.N.; Lee, E.S.; Kim, K.S. Trends in the prevalence of childhood asthma in Seoul Metropolitan City, Korea: The Seoul Atopy Asthma-friendly School Project. J. Prev. Med. Public Health 2018, 51, 275–280. [Google Scholar] [PubMed]
- Ha, J.; Lee, S.W.; Yon, D.K. Ten-year trends and prevalence of asthma, allergic rhinitis, and atopic dermatitis among the Korean population, 2008–2017. Clin. Exp. 2020, 63, 278. [Google Scholar] [CrossRef] [PubMed]
- Beasley, R. Worldwide variation in prevalence of symptoms of asthma, allergic rhino conjunctivitis, and atopic eczema: ISAAC The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet 1998, 351, 1225–1232. [Google Scholar]
- Korea Centers for Disease Control & Prevention. Cheongju (Korea): Korea Centers for Disease Control & Prevention; Coronavirus Disease 19. Available online: http://www.cdc.go.kr/index.es?sid=a2 (accessed on 30 March 2020).
- Kawachi, I. Income inequality and economic residential segregation. J. Epidemiol. Community Health 2002, 56, 165–166. [Google Scholar] [CrossRef]
- Krieger, N.; Williams, D.R.; Moss, N.E. Measuring social class in US public health research: Concepts, methodologies, and guidelines. Annu. Rev. Public Health 1997, 18, 341–378. [Google Scholar] [CrossRef]
- Jacob, C.; Bechtel, B.; Engel, S.; Kardos, P.; Linder, R.; Braun, S.; Greiner, W. Healthcare costs and resource utilization of asthma in Germany: A claims data analysis. Eur. J. Health Econ. 2015, 17, 195–201. [Google Scholar] [CrossRef]
- García-Altés, A.; Ruiz-Muñoz, D.; Colls, C.; Mias, M.; Martín, B.N. Socioeconomic inequalities in health and the use of healthcare services in Catalonia: Analysis of the individual data of 7.5 million residents. J. Epidemiol. Community Health 2018, 72, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Pillas, D.; Marmot, M.; Naicker, K.; Goldblatt, P.; Morrison, J.; Pikhart, H. Social inequalities in early childhood health and development: A European-wide systematic review. Pediatr. Res. 2014, 76, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, H.Y.; Kim, T.H.; Sheen, Y.H.; Lee, S.W.; An, J.; Kim, M.A.; Han, M.Y.; Yon, D.K. Serum heavy metal levels are associated with asthma, allergic rhinitis, atopic dermatitis, allergic multimorbidity, and airflow obstruction. J. Allergy Clin. Immunol. 2019, 7, 2912–2915. [Google Scholar]
- Gershon, A.S.; Dolmage, T.; Stephenson, A.; Jackson, B. Chronic obstructive pulmonary disease, and socioeconomic status: A systematic review. Int. J. Chronic Obstr. Pulm. Dis. 2012, 9, 216–226. [Google Scholar] [CrossRef]
- Laksono, A.D.; Wulandari, R.D.; Soedirham, O. Urban and rural disparities in hospital utilization among Indonesian adults. Iran. J. Public Health 2019, 48, 247–255. [Google Scholar] [PubMed]
- Sipahi, S.; Nacaroğlu, H.T.; Can, D.; Günay, I.; Ünsal-Karkıner, C.; Kamalı, H.; Özdemir, A.; Günay, T. Effect of socioeconomic status on allergic diseases and atopy in school children. Turk. J. Pediatr. 2017, 59, 670–677. [Google Scholar] [CrossRef]
- Carrilero, N.; Dalmau-Bueno, A.; García-Altés, A. Socioeconomic inequalities in 29 childhood diseases: Evidence from a 1,500,000 children population retrospective study. BMC Public Health 2021, 21, 1150. [Google Scholar] [CrossRef]
- Hong, S.-J.; Ahn, K.-M.; Lee, S.-Y.; Kim, K.-E. The prevalences of asthma and allergic diseases in Korean children. Korean J. Pediatr. 2008, 51, 343–350. [Google Scholar]
- Jee, H.M.; Kim, K.W.; Kim, C.S.; Sohn, M.H.; Shin, D.C.; Kim, K.E. Prevalence of asthma, rhinitis and eczema in Korean children using the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaires. Pediatr. Allergy Respir. Dis. 2009, 19, 165–172. [Google Scholar]
- Caubet, J.-C.; Eigenmann, P. Allergic triggers in atopic dermatitis. Immunol. Allergy Clin. N. Am. 2010, 30, 289–307. [Google Scholar] [CrossRef]
- Burrows, B.; Martinez, F.D.; Halonen, M.; Barbee, R.A.; Cline, M.G. Association of asthma with serum IgE levels and skin-test reactivity to allergens. N. Engl. J. Med. 1989, 320, 271–277. [Google Scholar] [CrossRef]
- Kurukulaaratchy, R.J.; Karmaus, W.; Raza, A.; Matthews, S.; Roberts, G.; Arshad, S.H. The influence of gender and atopy on the natural history of rhinitis in the first 18 years of life. Clin. Exp. Allergy 2011, 41, 851–859. [Google Scholar] [CrossRef]
- Wulandari, R.D.; Laksono, A.D.; Prasetyo, Y.B.; Nandini, N. Socioeconomic Disparities in Hospital Utilization Among Female Workers in Indonesia: A Cross-Sectional Study. J. Prim. Care Community Health 2022, 13, 21501319211072679. [Google Scholar] [CrossRef]
- Aligne, C.A.; Auinger, P.; Byrd, R.S.; Weitzman, M. Risk factors for pediatric asthma. Contributions of poverty, race, and urban residence. Am. J. Respir. Crit. Care Med. 2000, 162, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Amre, D.K.; Infante-Rivard, C.; Gautrin, D.; Malo, J.-L. Socioeconomic status, and utilization of health care services among asthmatic children. J. Asthma 2002, 39, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Stingone, J.A.; Claudio, L. Disparities in the use of urgent health care services among asthmatic children. Ann. Allergy Asthma Immunol. 2006, 97, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Kojima, R.; Shinohara, R.; Kushima, M.; Horiuchi, S.; Otawa, S.; Yokomichi, H.; Akiyama, Y.; Ooka, T.; Miyake, K.; Yamagata, Z.; et al. Association between Household Income and Allergy Development in Children: The Japan Environment and Children’s Study. Int. Arch. Allergy Immunol. 2022, 183, 201–209. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Allergic Asthma | Atopic Dermatitis | ||||
|---|---|---|---|---|---|---|
| Yes | Yes | |||||
| N | % | N | % | p | ||
| 2070 | 67.9 | 980 | 32.1 | |||
| Gender | Boys | 961 | 46.4 | 628 | 64.1 | <0.001 |
| Girls | 1109 | 53.6 | 352 | 35.9 | ||
| Age (Years) | Upto 12 | 1802 | 87.1 | 348 | 35.5 | <0.001 |
| Over 13 | 268 | 12.9 | 632 | 64.5 | ||
| Father’s education | Elementary school | 110 | 5.3 | 70 | 7.1 | |
| Middle school | 398 | 19.2 | 200 | 20.4 | 0.352 | |
| High school | 852 | 41.2 | 400 | 40.8 | ||
| University and above | 710 | 34.3 | 310 | 31.6 | ||
| Mother’s education | Elementary school | 140 | 6.8 | 51 | 5.2 | 0.412 |
| Middle school | 608 | 29.4 | 325 | 33.2 | ||
| High school | 742 | 35.8 | 424 | 43.3 | ||
| University and above | 580 | 28.0 | 180 | 18.4 | ||
| Occupation | Yes | 1245 | 60.1 | 911 | 93.0 | <0.001 |
| No | 825 | 39.9 | 69 | 7.0 | ||
| Residence | Urban | 1156 | 55.8 | 689 | 70.3 | <0.001 |
| Rural | 914 | 44.2 | 291 | 29.7 | ||
| Health insurance | NHI | 1125 | 54.3 | 945 | 96.4 | <0.001 |
| Medicare | 945 | 45.7 | 35 | 3.6 | ||
| Household income (SES) | Q1 (Lowest) | 501 | 24.2 | 139 | 14.2 | <0.001 |
| Q2 | 579 | 28.0 | 473 | 48.3 | ||
| Q3 | 610 | 29.5 | 158 | 16.1 | ||
| Q4 (Highest) | 380 | 18.4 | 210 | 21.4 | ||
| Healthcare utilization | Yes | 1258 | 60.8 | 752 | 76.7 | <0.001 |
| No | 812 | 39.2 | 228 | 23.3 | ||
| Variables | Healthcare Utilization (Yes) | |||||
|---|---|---|---|---|---|---|
| Allergic Asthma (n = 1258) | Atopic Dermatitis (n = 752) | |||||
| aOR * | 95% CI | p | aOR * | 95% CI | p | |
| Gender | ||||||
| Boys | Ref | Ref | ||||
| Girls | 1.36 | 1.08–1.71 | 0.018 | 1.38 | 1.24–1.54 | <0.001 |
| Age (Years) | ||||||
| Upto 12 | Ref | Ref | ||||
| Over 13 | 0.55 | 0.32–0.98 | <0.001 | 1.37 | 1.08–1.53 | <0.001 |
| Residence | ||||||
| Urban | Ref | Ref | ||||
| Rural | 0.98 | 0.95–1.02 | 0.335 | 0.74 | 0.41–1.33 | 0.268 |
| Household Income | ||||||
| Q1 (Lowest) | Ref | Ref | ||||
| Q2 | 1.05 | 1.00–1.10 | 0.003 | 1.29 | 1.14–1.46 | <0.0001 |
| Q3 | 1.2 | 1.04–1.38 | 0.021 | 1.37 | 0.58–3.23 | 0.152 |
| Q4 (Highest) | 1.36 | 1.08–1.71 | <0.001 | 1.58 | 1.41–1.76 | <0.001 |
| Health Insurance | ||||||
| NHI | 1.00 | 1.00 | ||||
| Medicare | 0.88 | 0.84–0.93 | <0.001 | 1.11 | 1.01–1.13 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kim, B.; Kim, D.H.; Kim, Y.; Rajaguru, V. Association between Socioeconomic Status and Healthcare Utilization for Children with Allergic Diseases: Korean National Health and Nutritional Examination Survey (2015–2019). Healthcare 2023, 11, 492. https://doi.org/10.3390/healthcare11040492
Kim J, Kim B, Kim DH, Kim Y, Rajaguru V. Association between Socioeconomic Status and Healthcare Utilization for Children with Allergic Diseases: Korean National Health and Nutritional Examination Survey (2015–2019). Healthcare. 2023; 11(4):492. https://doi.org/10.3390/healthcare11040492
Chicago/Turabian StyleKim, Jeoungmi, Bomgyeol Kim, Do Hee Kim, Yejin Kim, and Vasuki Rajaguru. 2023. "Association between Socioeconomic Status and Healthcare Utilization for Children with Allergic Diseases: Korean National Health and Nutritional Examination Survey (2015–2019)" Healthcare 11, no. 4: 492. https://doi.org/10.3390/healthcare11040492