
Factors Associated with Tuberculosis Outcome in a Hyperendemic City in the North of Brazil

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Scenario
2.3. Selection Criteria and Data Collection
2.4. Statistics Analysis
2.5. Ethics
3. Results
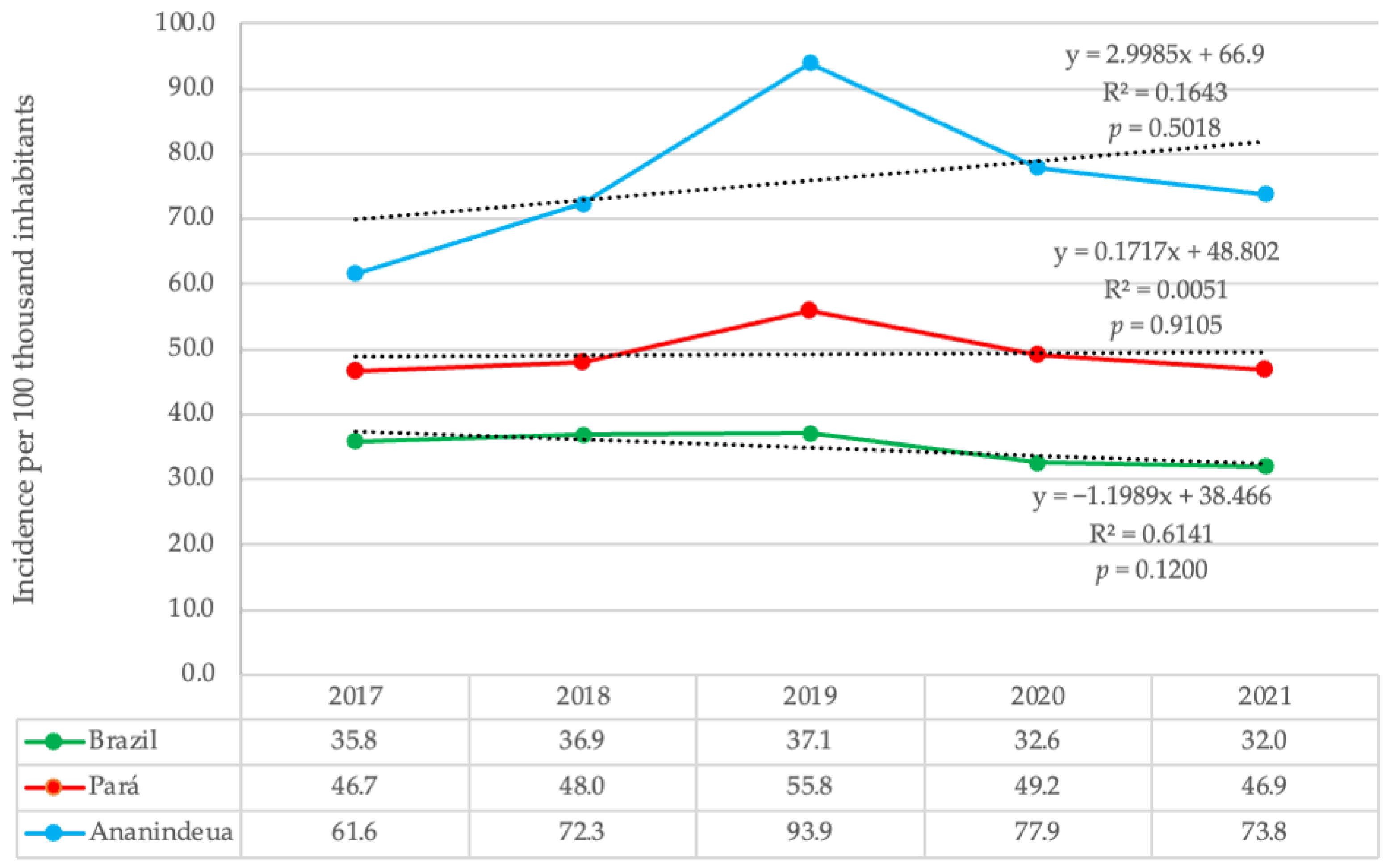
3.1. Number of New Reported Cases of Tuberculosis and Incidence Coefficient in Ananindeua, State of Pará and Brazil
3.2. Tuberculosis Treatment Outcomes Reported in Ananindeua
3.3. Socioeconomic Characteristics of Abandonment Cases and Cure Outcome
3.4. Epidemiological Characteristics of Abandonment Cases and Cure Outcome
3.5. Risk Factors Associated with Treatment Abandonment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brasil, Ministério da Saúde; Secretaria de Vigilância em Saúde; Departamento de Vigilância das Doenças Transmissíveis. Manual de Recomendações para o Controle da Tuberculose no Brasil; Ministério da Saúde: Brasília, Brazil, 2019; pp. 1–364. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/manual_recomendacoes_controle_tuberculose_brasil_2_ed.pdf (accessed on 22 May 2022).
- De Navarro, P.D.; Haddad, J.P.A.; Rabelo, J.V.C.; Silva, C.H.D.L.E.; de Almeida, I.N.; Carvalho, W.D.S.; de Miranda, S.S. The impact of the stratification by degree of clinical severity and abandonment risk of tuberculosis treatment. J. Bras. Pneumol. 2021, 47, e20210018. [Google Scholar] [CrossRef] [PubMed]
- Harling, G.; Neto, A.S.L.; Sousa, G.S.; Machado, M.M.T.; Castro, M.C. Determinants of tuberculosis transmission and treatment abandonment in Fortaleza, Brazil. BMC Public Health 2017, 17, 508. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.L.M.; Amaral, N.A.C.D.; Zacarias, A.C.P.; Ribeiro, L.K.D.N.P. Aspectos sociodemográficos e clínico-epidemiológicos do abandono do tratamento de tuberculose em Pernambuco, Brasil, 2001–2014. Epidemiol. Serviços Saúde 2017, 26, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Sousa, G.J.B.; Maranhão, T.A.; Leitão, T.D.M.J.S.; de Souza, J.T.; Moreira, T.M.M.; Pereira, M.L.D. Prevalência e fatores associados ao abandono do tratamento da tuberculose. Rev. Esc. Enferm. USP 2021, 55, e03767. [Google Scholar] [CrossRef] [PubMed]
- Soeiro, V.M.D.S.; Caldas, A.D.J.M.; Ferreira, T.F. Abandono do tratamento da tuberculose no Brasil, 2012–2018: Tendência e distribuição espaço-temporal. Cien. Saude Colet. 2022, 27, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Pará, Governo do Estado do Pará; Secretaria de Estado de Saúde Pública; Sistema Único de Saúde; Diretoria de Vigilância em Saúde; Departamento de Controle de Doenças Transmissíveis. Coordenação do Programa de Controle da Tuberculose. II Boletim Epidemiológico da Tuberculose. 2022. Available online: http://www.saude.pa.gov.br/a-secretaria/diretorias/dvs/tuberculose/be-tuberculose/ (accessed on 13 June 2022).
- World Health Organization (WHO). Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015—Report by the Secretariat. 2013. Available online: https://apps.who.int/iris/handle/10665/172828 (accessed on 14 May 2021).
- World Health Organization (WHO). The End TB Strategy. 2015. Available online: https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19 (accessed on 14 May 2021).
- Brasil, Ministério da Saúde; Secretaria de Vigilância em Saúde; Departamento de Vigilância das Doenças Transmissíveis. Brasil Livre da Tuberculose: Plano Nacional pelo Fim da Tuberculose como Problema de Saúde Pública; Ministério da Saúde: Brasília, Brazil, 2017; pp. 1–52. Available online: https://www.saude.gov.br/images/pdf/2017/julho/05/af-miolo-plano-nac-tuberculose-29jun17-grafica.pdf (accessed on 27 June 2021).
- Garcez, J.C.D.; Sardinha, D.M.; Conceição, E.C.; Costa, G.F.; Sousa, I.F.R.; Mesquita, C.R.; Carmo, W.C.D.; Rodrigues, Y.C.; Lima, L.N.G.C.; Lima, K.V.B. Surveillance Quality Indicators Highlight the Need for Improving Tuberculosis Diagnostics and Monitoring in a Hyperendemic Area of the Brazilian Amazon Region. Trop. Med. Infect. Dis. 2022, 7, 165. [Google Scholar] [CrossRef] [PubMed]
- Brasil, Ministério da Saúde. Departamento de Informática do Sistema Único de Saúde. Sistema de Informação de Agravos de Notificação—Sinan. Casos de Tuberculose—Desde 2001. 2022. Available online: https://datasus.saude.gov.br/acesso-a-informacao/casos-de-tuberculose-desde-2001-sinan/ (accessed on 27 November 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Malta, M.; Cardoso, L.O.; Bastos, F.I.; Magnanini, M.M.F.; da Silva, C.M.F.P. Iniciativa STROBE: Subsídios para a comunicação de estudos observacionais. Rev. Saude Publica 2010, 44, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Fundação Amazônia de Amparo a Estudos e Pesquisa (FAPESPA). População Total e Estimativas Populacionais, Pará e municipios—2017 a 2021, Anuário Estatístico do Pará 2021. 2021. Available online: https://www.fapespa.pa.gov.br/sistemas/anuario2021/tabelas/demografia/tab-1.1-populacao-total-e-estimativas-populacionais-2017-a-2021.htm (accessed on 6 July 2022).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Diretoria de Pesquisas. Coordenação de População e Indicadores Sociais. Gerência de Estudos e Análises da Dinâmica Demográfica. Projeção da população do Brasil e Unidades da Federação por sexo e idade para o período 2010–2060, 6 April 2020. Available online: https://www.ibge.gov.br/estatisticas/sociais/populacao/9109-projecao-da-populacao.html?=&t=resultados (accessed on 6 July 2022).
- Jain, V.K.; Iyengar, K.P.; Samy, D.A.; Vaishya, R. Tuberculosis in the era of COVID-19 in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1439–1443. [Google Scholar] [CrossRef]
- Maia1, C.M.F.; Martelli, D.R.B.; da Silveira, D.M.M.L.; Oliveira, E.A.; Júnior, H.M. Tuberculosis in Brazil: The impact of the COVID-19 pandemic. J. Bras. Pneumol. 2022, 48, e20220082. [Google Scholar] [CrossRef] [PubMed]
- Brasil, Ministério da Saúde; Departamento de Doenças, Condições Crônicas e Infecções Sexualmente Transmissíveis. Sistema de informação de tratamento especiais da tuberculose (Site-TB): Casos confirmados TB-DR, 1 November 2022. Available online: http://sitetb.saude.gov.br (accessed on 19 November 2022).
- Brasil, Ministério da Saúde; Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Sistema de Informação de Tratamento Especiais da Tuberculose (Site-TB), 4 May 2022. Available online: https://www.gov.br/aids/pt-br/indicadores-epidemiologicos/sistemas-de-informacao/sitetb (accessed on 19 November 2022).
- Dorman, S.E. Diagnosis of HIV-associated tuberculosis. Curr. Opin. HIV AIDS 2018, 13, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Meintjes, G.; Brust, J.C.M.; Nuttall, J.; Maartens, G. Management of active tuberculosis in adults with HIV. Lancet HIV 2019, 6, e463–e474. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, A.; Beena, P.; Devnikar, A.V.; Mali, S. A systemic review on tuberculosis. Indian J. Tuberc. 2020, 67, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Scholze, A.R. Análise Espacial e Temporal da Tuberculose Entre Pessoas em uso Crônico de Álcool, Tabaco e ou Drogas Ilícitas no Estado do Paraná. Ph.D. Thesis, Universidade de São Paulo, Ribeirão Preto, Brazil, 2021. Available online: https://www.teses.usp.br/teses/disponiveis/22/22133/tde-22032022-151416/publico/ALESSANDROROLIMSCHOLZE.pdf (accessed on 10 July 2022).
- Bezerra, W.D.S.P.; Lemos, E.F.; Prado, T.N.D.; Kayano, L.T.; de Souza, S.Z.; Chaves, C.E.V.; Paniago, A.M.M.; de Souza, A.S.; de Oliveira, S.M.D.V.L. Risk Stratification and Factors Associated with Abandonment of Tuberculosis Treatment in a Secondary Referral Unit. Patient Prefer. Adherence 2020, 14, 2389–2397. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.R.L.; Bonfim, R.O.; Siqueira, T.C.; Orfão, N.H. Abandono do tratamento da tuberculose: Uma revisão integrativa. Rev. Enferm. Contemp. 2018, 7, 63–71. [Google Scholar] [CrossRef]
- Sá, A.M.M.; de Aquino Santiago, L.; Santos, N.V.; Monteiro, N.P.; Pinto, P.H.A.; de Lima, A.M.; Iwasaka-Neder, P.L. Reasons for treatment abandonment among tuberculosis patients. Rev. Soc. Bras. Clin. Med. 2017, 15, 155–160. Available online: https://www.sbcm.org.br/revistas/RBCM/RBCM-2017-03.pdf#page=12 (accessed on 9 July 2022).
- Ragan, E.J.; Kleinman, M.B.; Sweigart, B.; Gnatienko, N.; Parry, C.D.; Horsburgh, C.R.; LaValley, M.P.; Myers, B.; Jacobson, K.R. The impact of alcohol use on tuberculosis treatment outcomes: A systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2020, 24, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.E.S.; Helman, B.; Silva, D.C.D.L.E.; de Aquino, C.; de Freitas, P.C.; Santos, R.D.O.; Brito, V.C.D.A.; Garcia, L.P.; Sardinha, L.M.V. Prevalência de consumo abusivo de bebidas alcoólicas na população adulta brasileira: Pesquisa Nacional de Saúde 2013 e 2019. Epidemiologia Serviços Saúde 2022, 31, 1–15. [Google Scholar] [CrossRef]
- Dos Santos, N.P.; Lírio, M.; Passos, L.A.R.; Dias, J.P.; Kritski, A.L.; Galvão-Castro, B.; Grassi, M.F.R. Completeness of tuberculosis reporting forms in five Brazilian capitals with a high incidence of the disease. J. Bras. Pneumol. 2013, 39, 221–225. [Google Scholar] [CrossRef]
- Da Silva, G.D.M.; Bartholomay, P.; Cruz, O.G.; García, L.P. Avaliação da qualidade dos dados, oportunidade e aceitabilidade da vigilância da tuberculose nas microrregiões do Brasil. Cien. Saude Colet. 2017, 22, 3307–3319. [Google Scholar] [CrossRef] [Green Version]
- Brasil, Ministério da Saúde; Secretaria de Vigilância em Saúde; Departamento de Vigilância Epidemiológica. Guia de Vigilância Epidemiológica, 7th ed.; Ministério da Saúde: Brasília, Brazil, 2009; pp. 1–816. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_epidemiologica_7ed.pdf (accessed on 25 September 2022).


{kind=link}
| Year | Ananindeua | Pará | Brazil |
|---|---|---|---|
| 2017 | 318 | 3920 | 74,097 |
| 2018 | 380 | 4099 | 76,923 |
| 2019 | 498 | 4823 | 77,891 |
| 2020 | 417 | 4293 | 68,939 |
| 2021 | 399 | 4133 | 68,271 |
| Total | 2012 | 21,268 | 366,121 |
| Outcome | 2017 | 2018 | 2019 | 2020 | 2021 | Total |
|---|---|---|---|---|---|---|
| Cure | 258 (70.1) | 309 (68.8) | 371 (65.5) | 296 (60.9) | 135 (28.7) | 1369 (58.5) |
| Abandonment | 27 (7.3) | 53 (11.8) | 49 (8.7) | 54 (11.1) | 47 (10.0) | 230 (9.8) |
| Death by TB | 5 (1.4) | 0 (0.0) | 4 (0.7) | 8 (1.6) | 3 (0.6) | 20 (0.9) |
| Death by other reasons | 10 (2.7) | 12 (2.7) | 11 (1.9) | 11 (2.3) | 7 (1.5) | 51 (2.2) |
| Transferences | 28 (7.6) | 56 (12.5) | 61 (10.8) | 30 (6.2) | 23 (4.9) | 198 (8.5) |
| Diagnosis change | 4 (1.1) | 6 (1.3) | 7 (1.2) | 5 (1.0) | 0 (0.0) | 22 (0.9) |
| DR-TB | 2 (0.5) | 4 (0.9) | 4 (0.7) | 0 (0.0) | 1 (0.2) | 11 (0.5) |
| Schema change | 0 (0.0) | 2 (0.4) | 0 (0.0) | 1 (0.2) | 2 (0.4) | 5 (0.2) |
| Primary abandonment | 0 (0.0) | 0 (0.0) | 1 (0.2) | 0 (0.0) | 1 (0.2) | 2 (0.1) |
| Blank | 34 (9.2) | 7 (1.6) | 58 (10.2) | 81 (16.7) | 251 (53.4) | 431 (18.4) |
| Total | 368 | 449 | 566 | 486 | 470 | 2339 |
| Indicators | Cases Number (n = 1599) | Abandonment (n = 230) | Cure (n = 1369) | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Female | 630 (39.4) | 76 (33.0) | 554 (40.5) | 0.0395 a |
| Male | 969 (60.6) | 154 (67.0) | 815 (59.5) | |
| Age | ||||
| ≤19 y.o | 179 (11.2) | 16 (7.0) | 163 (11.9) | 0.0062 a |
| 20 to 59 y.o | 1223 (76.5) | 194 (84.3) | 1029 (75.2) | |
| ≥60 y.o | 181 (11.3) | 17 (7.4) | 164 (12.0) | |
| Ignored | 16 (1.0) | 3 (1.3) | 13 (0.9) | |
| Ethnicity | ||||
| White | 172 (10.8) | 16 (7.0) | 156 (11.4) | <0.0001 b |
| Black | 148 (9.3) | 29 (12.6) | 119 (8.7) | |
| Yellow | 7 (0.4) | 2 (0.9) | 5 (0.4) | |
| Pardo/brown | 1229 (76.9) | 174 (75.7) | 1055 (77.1) | |
| Indigenous | 4 (0.3) | 1 (0.4) | 3 (0.2) | |
| Ignored | 39 (2.4) | 8 (3.5) | 31 (2.3) | |
| Schooling | ||||
| Illiterate | 21 (1.3) | 3 (1.3) | 18 (1.3) | <0.0001 b |
| Primary incomplete | 466 (29.1) | 95 (41.3) | 371 (27.1) | |
| Elementary School complete | 309 (19.3) | 44 (19.1) | 265 (19.4) | |
| High School complete | 365 (22.8) | 26 (11.3) | 339 (24.8) | |
| College degree complete | 68 (4.3) | 2 (0.9) | 66 (4.8) | |
| Ignored | 370 (23.1) | 60 (26.1) | 310 (22.6) | |
| Income Transfer Program | ||||
| Yes | 127 (7.9) | 15 (6.5) | 112 (8.2) | 0.4439 a |
| No | 1384 (86.6) | 204 (88.7) | 1180 (86.2) | |
| Ignored | 88 (5.5) | 11 (4.8) | 77 (5.6) |
| Indicators | Cases Number (n = 1599) | Abandonment (n = 230) | Cure (n = 1369) | p-Value |
|---|---|---|---|---|
| Type of entry/admission | ||||
| New Case | 1389 (86.9) | 186 (80.9) | 1203 (87.9) | <0.0001 a |
| Recurrence | 76 (4.8) | 12 (5.2) | 64 (4.7) | |
| Re-entry after abandonment | 45 (2.8) | 19 (8.3) | 26 (1.9) | |
| Transfer | 86 (5.4) | 12 (5.2) | 74 (5.4) | |
| Don’t know | 3 (0.2) | 1 (0.4) | 2 (0.1) | |
| Disease form | ||||
| Pulmonary | 1427 (89.2) | 214 (93.0) | 1213 (88.6) | 0.0581 a |
| Extrapulmonary (or mixed) | 172 (10.8) | 16 (7.0) | 156 (11.4) | |
| DOT | ||||
| Yes | 229 (14.3) | 18 (7.8) | 211 (15.4) | 0.1735 a |
| No | 1276 (79.8) | 142 (61.7) | 1134 (82.8) | |
| Ignored | 94 (5.9) | 70 (30.4) | 24 (1.8) | |
| Alcoholism | ||||
| Yes | 178 (11.1) | 51 (22.2) | 127 (9.3) | <0.0001 a |
| No | 1382 (86.4) | 171 (74.3) | 1211 (88.5) | |
| Ignored | 39 (2.4) | 8 (3.5) | 31 (2.3) | |
| Smoking | ||||
| Yes | 156 (9.8) | 46 (20.0) | 110 (8.0) | <0.0001 a |
| No | 1417 (88.6) | 178 (77.4) | 1239 (90.5) | |
| Ignored | 26 (1.6) | 6 (2.6) | 20 (1.5) | |
| Illicit Drugs | ||||
| Yes | 105 (6.6) | 38 (16.5) | 67 (4.9) | <0.0001 a |
| No | 1459 (91.2) | 184 (80.0) | 1275 (93.1) | |
| Ignored | 35 (2.2) | 8 (3.5) | 27 (2,0) | |
| HIV | ||||
| Positive | 145 (9.1) | 35 (15.2) | 110 (8.0) | <0.0001 a |
| Negative | 697 (43.6) | 67 (29.1) | 630 (46.0) | |
| Not performed | 757 (47.3) | 128 (55.7) | 629 (45.9) |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Gender (male vs. female) | 1.31 | 0.94–1.83 | 0.107 | |||
| Age (20 to 59 vs. other ages) | 1.57 | 1.04–2.38 | 0.033 | 1.55 | 1.03–2.32 | 0.035 |
| Ethnicity (brown vs. other ethnicities) | 1.02 | 0.69–1.51 | 0.923 | |||
| Type of entry/admission (new case vs. other types of entry) | 0.49 | 0.31–0.78 | 0.002 | |||
| Alcoholism (yes vs. no) | 2.72 | 1.68–4.40 | <0.001 | 1.74 | 1.11–2.72 | 0.016 |
| Smoking (yes vs. no) | 3.33 | 1.73–6.41 | <0.001 | |||
| Illicit Drugs (yes vs. no) | 4.23 | 2.35–7.60 | <0.001 | 2.64 | 1.56–4.46 | <0.001 |
| Year (2018 vs. 2017) | 0.77 | 0.53–1.12 | 0.171 | |||
| Year (2019 vs. 2017) | 1.13 | 0.81–1.57 | 0.482 | |||
| Year (2020 vs. 2017) | 0.82 | 0.59–1.15 | 0.254 | |||
| Year (2021 vs. 2017) | 1.47 | 1.03–2.09 | 0.032 | 1.45 | 1.01–2.08 | 0.043 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, G.F.; Garcez, J.C.D.; Marcos, W.; Ferreira, A.L.d.S.; Andrade, J.A.A.; Rodrigues, Y.C.; Lima, L.N.G.C.; Conceição, E.C.; Lima, K.V.B. Factors Associated with Tuberculosis Outcome in a Hyperendemic City in the North of Brazil. Healthcare 2023, 11, 508. https://doi.org/10.3390/healthcare11040508
Costa GF, Garcez JCD, Marcos W, Ferreira ALdS, Andrade JAA, Rodrigues YC, Lima LNGC, Conceição EC, Lima KVB. Factors Associated with Tuberculosis Outcome in a Hyperendemic City in the North of Brazil. Healthcare. 2023; 11(4):508. https://doi.org/10.3390/healthcare11040508
Chicago/Turabian StyleCosta, Gabriel Fazzi, Juliana Conceição Dias Garcez, Weber Marcos, Ana Lúcia da Silva Ferreira, Jorge Alberto Azevedo Andrade, Yan Corrêa Rodrigues, Luana Nepomuceno Gondim Costa Lima, Emilyn Costa Conceição, and Karla Valéria Batista Lima. 2023. "Factors Associated with Tuberculosis Outcome in a Hyperendemic City in the North of Brazil" Healthcare 11, no. 4: 508. https://doi.org/10.3390/healthcare11040508