
An In-Depth Analysis of Providers and Services of Cancellation in Anesthesia Reveals a Complex Picture after Systemic Analysis

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Overall Cancellation Rates
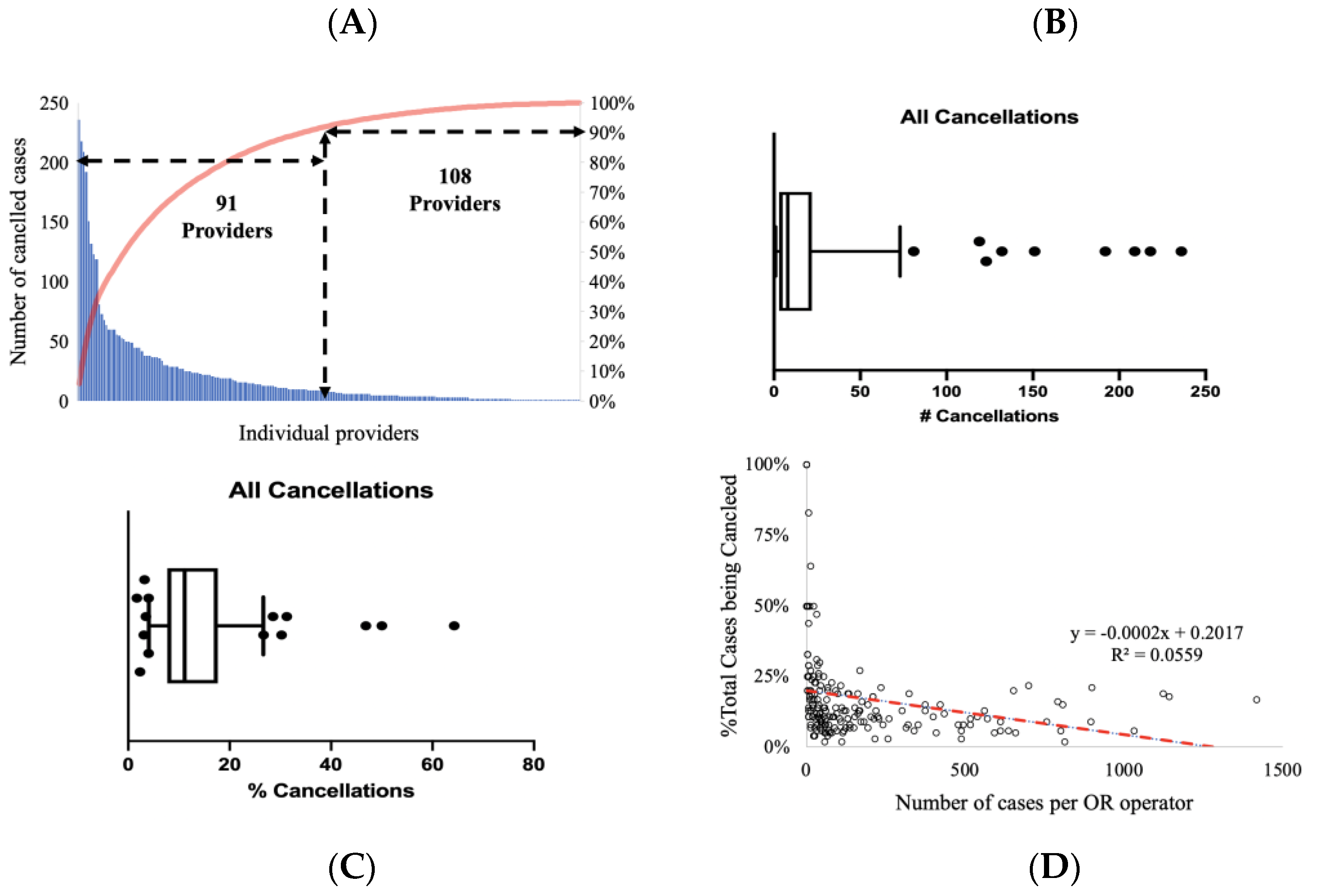
3.2. Analysis of Cancellation per Surgeon
3.3. Analysis of Surgical Cancellation per Service Line
3.4. Analysis of Surgical Cancellation per Time and Place
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ehrenfeld, J.M.; Dexter, F.; Rothman, B.S.; Johnson, A.M.; Epstein, R.H. Case cancellation rates measured by surgical service differ whether based on the Number of cases or the Number of minutes cancelled. Anaesth. Analg. 2013, 117, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, A.; Macpherseon, R. The anaesthetic pre-admission clinic is effective in minimising surgical cancellation rates. Anaesth. Intensive Care 2013, 41, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, B.K.; Yu, Y.Y.; Lin, R.S. Attitudes of the patients and their families towards cancellation of anesthesia and surgery in hypertensive patients. Acta Anaesthesiol. Taiwan. 2004, 42, 9–14. [Google Scholar] [PubMed]
- Yıldız Altun, A.; Özer, A.B.; Aksoku, B.T.; Karatepe, Ü.; Kilinç, M.; Erhan, Ö.L.; Demirel, İ.; Bolat, E. Evaluation of the Reasons for the Cancellation of Elective Procedures at Level 3 University Hospital on the Day of Surgery. J. PeriAnesthesia Nurs. 2020, 35, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Okeke, C.J.; Obi, A.O.; Tijani, K.H.; Eni, U.E.; Okorie, C.O. Cancellation of elective surgical cases in a Nigerian teaching hospital: Frequency and reasons. Niger. J. Clin. Pract. 2020, 23, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Sanjay, P.; Dodds, A.; Miller, E.; Arumugam, P.J.; Woodward, A. Cancelled elective operations: An observational study from a district general hospital. J. Health Organ. Manag. 2007, 21, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Sarang, B.; Bhandoria, G.; Patil, P.; Gadgil, A.; Bains, L.; Khajanchi, M.; Kizhakke Veetil, D.; Dutta, R.; Shah, P.; Bhandarkar, P.; et al. Assessing the Rates and Reasons of Elective Surgical Cancellations on the Day of Surgery: A Multicentre Study from Urban Indian Hospitals. World J. Surg. 2021, 46, 382–390. [Google Scholar] [CrossRef]
- Cho, H.S.; Lee, Y.S.; Lee, S.G.; Kim, J.M.; Kim, T.H. Reasons for Surgery Cancellation in a General Hospital: A 10-year Study. Int. J. Environ. Res. Public Health 2018, 16, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roxbury, C.R.; Shah, J.; Tang, D.; Kshettry, V.R.; Recinos, P.F.; Woodard, T.D.; Taylor, M.; Sindwani, R. Analysis of 24-hour surgical cancellations in an academic rhinology and skull base surgery practice. Int. Forum Allergy Rhinol. 2019, 9, 298–304. [Google Scholar] [CrossRef]
- Wong, D.J.N.; Harris, S.K.; Moonesinghe, S.R. Cancelled operations: A 7-day cohort study of planned adult inpatient surgery in 245 UK National Health Service hospitals. Br. J. Anaesth. 2018, 121, 730–738. [Google Scholar] [CrossRef]
- Desta, M.; Manaye, A.; Tefera, A.; Worku, A.; Wale, A.; Mebrat, A.; Gobena, N. Incidence and causes of cancellations of elective operation on the intended day of surgery at a tertiary referral academic medical center in Ethiopia. Patient Saf. Surg. 2018, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Prin, M.; Eaton, J.; Mtalimanja, O.; Charles, A. High Elective Surgery Cancellation Rate in Malawi Primarily Due to Infrastructural Limitations. World J. Surg. 2018, 42, 1597–1602. [Google Scholar] [CrossRef]
- Abeeleh, M.A.; Tareef, T.M.; Hani, A.B.; Albsoul, N.; Samarah, O.Q.; ElMohtaseb, M.S.; Alshehabat, M.; Ismail, Z.B.; Alnoubani, O.; Obeidat, S.S.; et al. Reasons for operation cancellations at a teaching hospital: Prioritizing areas of improvement. Ann. Surg. Treat. Res. 2017, 93, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.J.; McAvoy, J.; Dweik, D.; Ferrigno, M.; Macario, A.; Haisjackl, M. Cancellation of Elective Cases in a Recently Opened, Tertiary/Quaternary-Level Hospital in the Middle East. Anesth. Analg. 2017, 125, 268–271. [Google Scholar] [CrossRef]
- Appavu, S.T.; Al-Shekaili, S.M.; Al-Sharif, A.M.; Elawdy, M.M. The Burden of Surgical Cancellations and No-Shows: Quality management study from a large regional hospital in Oman. Sultan Qaboos Univ. Med. J. 2016, 16, e298–e302. [Google Scholar] [CrossRef] [PubMed]
- Fayed, A.; Elkouny, A.; Zoughaibi, N.; Wahabi, H.A. Elective surgery cancelation on day of surgery: An endless dilemma. Saudi J. Anaesth. 2016, 10, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.K.; Adeola, J.O.; Beutler, S.S.; Urman, R.D. Postoperative Pain Management in Enhanced Recovery Pathways. J Pain Res. 2022, 15, 123–135. [Google Scholar] [CrossRef]
- Dhafar, K.O.; Ulmalki, M.A.; Felemban, M.A.; Mahfouz, M.E.; Baljoon, M.J.; Gazzaz, Z.J.; Baig, M.; Hamish, N.H.; AlThobaiti, S.A.; Al-Hothali, F.T. Cancellation of operations in Saudi Arabian hospitals: Frequency, reasons and suggestions for improvements. Pak. J. Med. Sci. 2015, 31, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- McKendrick, D.R.; Cumming, G.P.; Lee, A.J. A 5-year observational study of cancellations in the operating room: Does the introduction of preoperative preparation have an impact? Saudi J. Anaesth. 2014, 8 (Suppl. S1), S8–S14. [Google Scholar] [CrossRef] [PubMed]
- Sahraoui, A.; Elarref, M. Bed crisis and elective surgery late cancellations: An approach using the theory of constraints. Qatar Med. J. 2014, 2014, 1–11. [Google Scholar] [CrossRef]
- Laisi, J.; Tohmo, H.; Keränen, U. Surgery cancelation on the day of surgery in same-day admission in a Finnish hospital. Scand. J. Surg. 2013, 102, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Dexter, F.; Shi, P.; Epstein, R.H. Descriptive study of case scheduling and cancellations within 1 week of the day of surgery. Anesth. Analg. 2012, 115, 1188–1195. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Gandhi, R. Reasons for cancellation of operation on the day of intended surgery in a multidisciplinary 500 bedded hospital. J. Anaesthesiol. Clin. Pharmacol. 2012, 28, 66–69. [Google Scholar] [CrossRef]
- Ezike, H.; Ajuzieogu, V.; Amucheazi, A. Reasons for elective surgery cancellation in a referral hospital. Ann. Med. Health Sci. Res. 2011, 1, 197–202. [Google Scholar] [PubMed]
- Schuster, M.; Neumann, C.; Neumann, K.; Braun, J.; Geldner, G.; Martin, J.; Spies, C.; Bauer, M. The effect of hospital size and surgical service on case cancellation in elective surgery: Results from a prospective multicenter study. Anesth. Analg. 2011, 113, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Sung, W.C.; Chou, A.H.; Liao, C.C.; Yang, M.W.; Chang, C.J. Operation cancellation at Chang Gung Memorial Hospital. Chang Gung Med. J. 2010, 33, 568–575. [Google Scholar] [PubMed]
- González-Arévalo, A.; Gómez-Arnau, J.I.; delaCruz, F.J.; Marzal, J.M.; Ramírez, S.; Corral, E.M.; García-del-Valle, S. Causes for cancellation of elective surgical procedures in a Spanish general hospital. Anaesthesia 2009, 64, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Mehran, N.; Ojalvo, I.; Myers, J.S.; Razeghinejad, R.; Lee, D.; Kolomeyer, N.N. Surgical Cancellations in Glaucoma Practice: Causes, Delays, and Effect on Patient Care and Revenue. Ophthalmol. Glaucoma 2021, 4, 427–432. [Google Scholar] [CrossRef]
- Conley, C.; Facchin, M.; Gu, Q.; Mukerji, S.; Cohen, R.; O’Brien, S.; Nurhussien, L.; Ferrari, L. The virtual pediatric perioperative home, experience at a major metropolitan safety net hospital. Paediatr. Anaesth. 2021, 31, 686–694. [Google Scholar] [CrossRef]
- Coudane, H.; Benfrech, E.; Lecoq, C.; Zabee, L.; Tracol, P.; Danan, J.L.; Bruno, P.Y.; Lighezzolo Alnot, J. No-go decision: A newly identified adverse event in orthopaedic surgery—Causes and medico-legal implications. Orthop. Traumatol. Surg. Res. 2018, 104, 519–522. [Google Scholar] [CrossRef]
- Epstein, R.H.; Dexter, F. Rescheduling of previously cancelled surgical cases does not increase variability in operating room workload when cases are scheduled based on maximizing efficiency of use of operating room time. Anesth. Analg. 2013, 117, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Hori, Y.; Nakayama, A.; Sakamoto, A. Surgery cancellations after entering the operating room. JA Clin. Rep. 2016, 2, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzsimons, M.G.; Dilley, J.D.; Moser, C.; Walker, J.D. Analysis of 43 Intraoperative Cardiac Surgery Case Cancellations. J. Cardiothorac. Vasc. Anesth. 2016, 30, 19–22. [Google Scholar] [CrossRef]
- Lau, H.K.; Chen, T.H.; Liou, C.M.; Chou, M.C.; Hung, W.T. Retrospective analysis of surgery postponed or cancelled in the operating room. J. Clin. Anesth. 2010, 22, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Petrone, B.; Fakhoury, J.; Matai, P.; Bitterman, A.; Cohn, R.M.; Lutsky, L. Predicting Elective Orthopaedic Sports Medicine Surgical Cancellations Based on Patient Demographics. Arthrosc. Sports Med. Rehabil. 2020, 2, e83–e89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, A.L.; Chiew, C.J.; Wang, S.; Abdullah, H.R.; Lam, S.S.; Ong, M.E.H.; Tan, H.K.; Wong, T.H. Risk factors and reasons for cancellation within 24 h of scheduled elective surgery in an academic medical centre: A cohort study. Int. J. Surg. 2019, 66, 72–78. [Google Scholar] [CrossRef]
- de Lorenzo-Pinto, A.; Ortega-Navarro, C.; Ribed, A.; Giménez-Manzorro, Á.; Ibáñez-García, S.; de Miguel-Guijarro, Á.; Ginel-Feito, M.D.; Herranz, A.; Sanjurjo-Sáez, M. Cancellations of elective surgical procedures due to inadequate management of chronic medications. J. Clin. Pharm. Ther. 2019, 44, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Dexter, F.; Maxbauer, T.; Stout, C.; Archbold, L.; Epstein, R.H. Relative influence on total cancelled operating room time from patients who are inpatients or outpatients preoperatively. Anesth. Analg. 2014, 118, 1072–1080. [Google Scholar] [CrossRef]
- Ahmed, T.; Khan, M.; Khan, F.A. Cancellation of surgery in patients attending the preoperative anaesthesia assessment clinic: A prospective audit. J. Pak. Med. Assoc. 2009, 59, 547–550. [Google Scholar]
- Bamashmus, M.; Haider, T.; Al-Kershy, R. Why is cataract surgery canceled? A retrospective evaluation. Eur. J. Ophthalmol. 2010, 20, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Woods, A.W.; Wylie, P. Cancellation of elective abdominal aortic aneurysms due to lack of ICU beds. Anaesthesia 1997, 52, 1115–1116. [Google Scholar] [PubMed]
- Tzabar, Y. Cancellation of major surgery due to lack of ITU beds. Anaesthesia 1998, 53, 407. [Google Scholar] [PubMed]
- Liu, L.; Ni, Y.; Beck, A.F.; Brokamp, C.; Ramphul, R.C.; Highfield, L.D.; Kanjia, M.K.; Pratap, J.N. Understanding Pediatric Surgery Cancellation: Geospatial Analysis. J. Med. Int. Res. 2021, 23, e26231. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Chen, K.W.; Chen, K.B.; Poon, K.S.; Liu, S.K. Case review analysis of operating room decisions to cancel surgery. BMC Surg. 2014, 14, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Ni, Y.; Zhang, N.; Nick Pratap, J. Mining patient-specific and contextual data with machine learning technologies to predict cancellation of children′s surgery. Int. J. Med. Inform. 2019, 129, 234–241. [Google Scholar] [CrossRef]
- Dexter, F.; Marcon, E.; Epstein, R.H.; Ledolter, J. Validation of statistical methods to compare cancellation rates on the day of surgery. Anesth. Analg. 2005, 101, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Sato, M.; Ida, M.; Naito, Y.; Kawaguchi, M. The incidence and reasons for canceled surgical cases in an academic medical center: A retrospective analysis before and after the development of a preoperative anesthesia clinic. J. Anesth. 2020, 34, 892–897. [Google Scholar] [CrossRef]
- Dexter, F.; Wachtel, R.E. Strategies for net cost reductions with the expanded role and expertise of anesthesiologists in the perioperative surgical home. Anesth. Analg. 2014, 118, 1062–1071. [Google Scholar] [CrossRef]
- Vazirani, S.; Lankarani-Fard, A.; Liang, L.J.; Stelzner, M.; Asch, S.M. Perioperative processes and outcomes after implementation of a hospitalist-run preoperative clinic. J. Hosp. Med. 2012, 7, 697–701. [Google Scholar] [CrossRef]
- Wong, G.T.; Sun, N.C. Providing perioperative care for patients with hip fractures. Osteoporos. Int. 2010, 21 (Suppl. S4), S547–S553. [Google Scholar] [CrossRef] [Green Version]
- Farasatkish, R.; Aghdaii, N.; Azarfarin, R.; Yazdanian, F. Can preoperative anesthesia consultation clinic help to reduce operating room cancellation rate of cardiac surgery on the day of surgery? Middle East J. Anaesthesiol. 2009, 20, 93–96. [Google Scholar] [PubMed]
- Peterson, K.; McCleery, E.; Anderson, J.; Waldrip, K.; Helfand, M. Evidence Brief: Comparative Effectiveness of Appointment Recall Reminder Procedures for Follow-Up Appointments; Department of Veterans Affairs: Washington, DC, USA, 2015; PMID: 27606388. [Google Scholar]
- Bellini, V.; Guzzon, M.; Bigliardi, B.; Mordonini, M.; Filippelli, S.; Bignami, E. Artificial Intelligence: A New Tool in Operating Room Management. Role of Machine Learning Models in Operating Room Optimization. J. Med. Syst. 2019, 44, 20. [Google Scholar] [CrossRef] [PubMed]
- Swanson, H.L.; Scheb, D.M. The role of the anesthesia care coordinator in preadmission testing. AORN J. 1996, 64, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Rai, M.R.; Pandit, J.J. Day of surgery cancellations after nurse-led pre-assessment in an elective surgical centre: The first 2 years. Anaesthesia 2003, 58, 692–699. [Google Scholar] [CrossRef]
- Osman, T.; Lew, E.; Lum, E.P.; van Galen, L.; Dabas, R.; Sng, B.L.; Car, J. PreAnaesThesia computerized health (PATCH) assessment: Development and validation. BMC Anesthesiol. 2020, 20, 286. [Google Scholar] [CrossRef]
- Liu, S.; Lu, X.; Jiang, M.; Li, W.; Li, A.; Fang, F.; Cang, J. Preoperative assessment clinics and case cancellations: A prospective study from a large medical center in China. Ann. Transl. Med. 2021, 9, 1501. [Google Scholar] [CrossRef]
- Vogelsang, H.; Herzog-Niescery, J.; Botteck, N.M.; Hasse, F.; Peszko, A.; Weber, T.P.; Gude, P. Improvement in pre-operative risk assessment in adults undergoing noncardiac surgery by a process-oriented score: A prospective single-centre study. Eur. J. Anaesthesiol. 2020, 37, 629–635. [Google Scholar] [CrossRef]
- Greig, P.R.; Higham, H.E.; Darbyshire, J.L.; Vincent, C. Go/no-go decision in anaesthesia: Wide variation in risk tolerance amongst anaesthetists. Br. J. Anaesth. 2017, 118, 740–746. [Google Scholar] [CrossRef] [Green Version]
- Wijeysundera, D.N.; Austin, P.C.; Beattie, W.S.; Hux, J.E.; Laupacis, A. A population-based study of anesthesia consultation before major noncardiac surgery. Arch. Intern. Med. 2009, 169, 595–602. [Google Scholar] [CrossRef]
- Schretlen, S.; Hoefsmit, P.; Kats, S.; van Merode, G.; Maessen, J.; Zandbergen, R. Reducing surgical cancellations: A successful application of Lean Six Sigma in healthcare. BMJ Open Qual. 2021, 10, e001342. [Google Scholar] [CrossRef]
- Verheij, R.A.; Curcin, V.; Delaney, B.C.; McGilchrist, M.M. Possible Sources of Bias in Primary Care Electronic Health Record Data Use and Reuse. J. Med. Int. Res. 2018, 20, e185. [Google Scholar] [CrossRef] [PubMed]
- Hospitals, A. Fast Facts on US Hospitals. December 2016. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwi2upKRqeX8AhVfkWMGHbNzAHEQFnoECA4QAQ&url=https%3A%2F%2Fwww.aha.org%2Fsystem%2Ffiles%2F2018-02%2F2018-aha-hospital-fast-facts.pdf&usg=AOvVaw3o6F2ZF1ewGZB7oOiPFRZQ (accessed on 15 February 2022).
- Zheng, K.; Gao, J.; Ngiam, K.Y.; Chin Ooi, B.; James Yip, W.L. Resolving the Bias in Electronic Medical Records. In KDD2017, Proceedings of the 23rd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Halifax, NS, Canada, 13–17 August 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 2171–2180. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | Reason | Additional Info | N; % Total | ||||
|---|---|---|---|---|---|---|---|
| Cancelled before patient reaching hospital | Patient-Related | Patient no show day of surgery | 455 (10.9%) | ||||
| Patient canceled | 552 (13.3%) | ||||||
| No ride/weather/traffic | 76 (1.8%) | ||||||
| The patient did not follow instructions | Did not take medications $Not adhering to pre-operative fasting$Poor bowel prep$No adequate pre-surgical workup | 108 (2.6%) | |||||
| Miscellanea | A patient seeking second opinion $Patient family refused $Patient positive for drugs/alcohol | 27 (0.6%) | |||||
| Clinical | Patient illness | Medical complication (diabetes, anticoagulation, blood pressure, other)$Cancelled for medical reasons$Abnormal tests | 207 (5.0%) | ||||
| Medical clearance and further med/surgical evaluation | 163 (3.9%) | ||||||
| No longer indicated | 203 (4.9%) | ||||||
| Misc (patient condition improved, patient expired) | 46 (1.1%) | ||||||
| Administrative | Date change | 773 (18.6%) | |||||
| Scheduling error | 134 (3.2%) | ||||||
| Canceled by administrator | 111 (2.7%) | ||||||
| Miscellanea | Change of location$Faculty availability$Routine schedule rearrangement$Financial/authorization issues$The patient did not receive prep products or instructions$Others | 146 (3.5%) | |||||
| Other | Canceled for non-medical reasons$Surgeon misc. cancellation$Equipment not available | 44 (1.1%) | |||||
| Total number of cancellations before patients reach pre-op | 3045 (73.1%) | ||||||
| Total number of cancellations with patients in the pre-operative preparation area | 636 (15.3%) | ||||||
| Total number of cancellations with patients in the operating room | 68 (1.6%) | ||||||
| Totalnumber of cancellations | 3749 (90%) | ||||||
| Duplicate record or log created in error | 416 (10%) | ||||||
| Total cancellations | 4165 (100%) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laudanski, K.; Wain, J.; Pizzini, M.-A. An In-Depth Analysis of Providers and Services of Cancellation in Anesthesia Reveals a Complex Picture after Systemic Analysis. Healthcare 2023, 11, 357. https://doi.org/10.3390/healthcare11030357
Laudanski K, Wain J, Pizzini M-A. An In-Depth Analysis of Providers and Services of Cancellation in Anesthesia Reveals a Complex Picture after Systemic Analysis. Healthcare. 2023; 11(3):357. https://doi.org/10.3390/healthcare11030357
Chicago/Turabian StyleLaudanski, Krzysztof, Justin Wain, and Mark-Alan Pizzini. 2023. "An In-Depth Analysis of Providers and Services of Cancellation in Anesthesia Reveals a Complex Picture after Systemic Analysis" Healthcare 11, no. 3: 357. https://doi.org/10.3390/healthcare11030357