
Oral Manifestations in Children Diagnosed with COVID-19: A Narrative Review

 ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
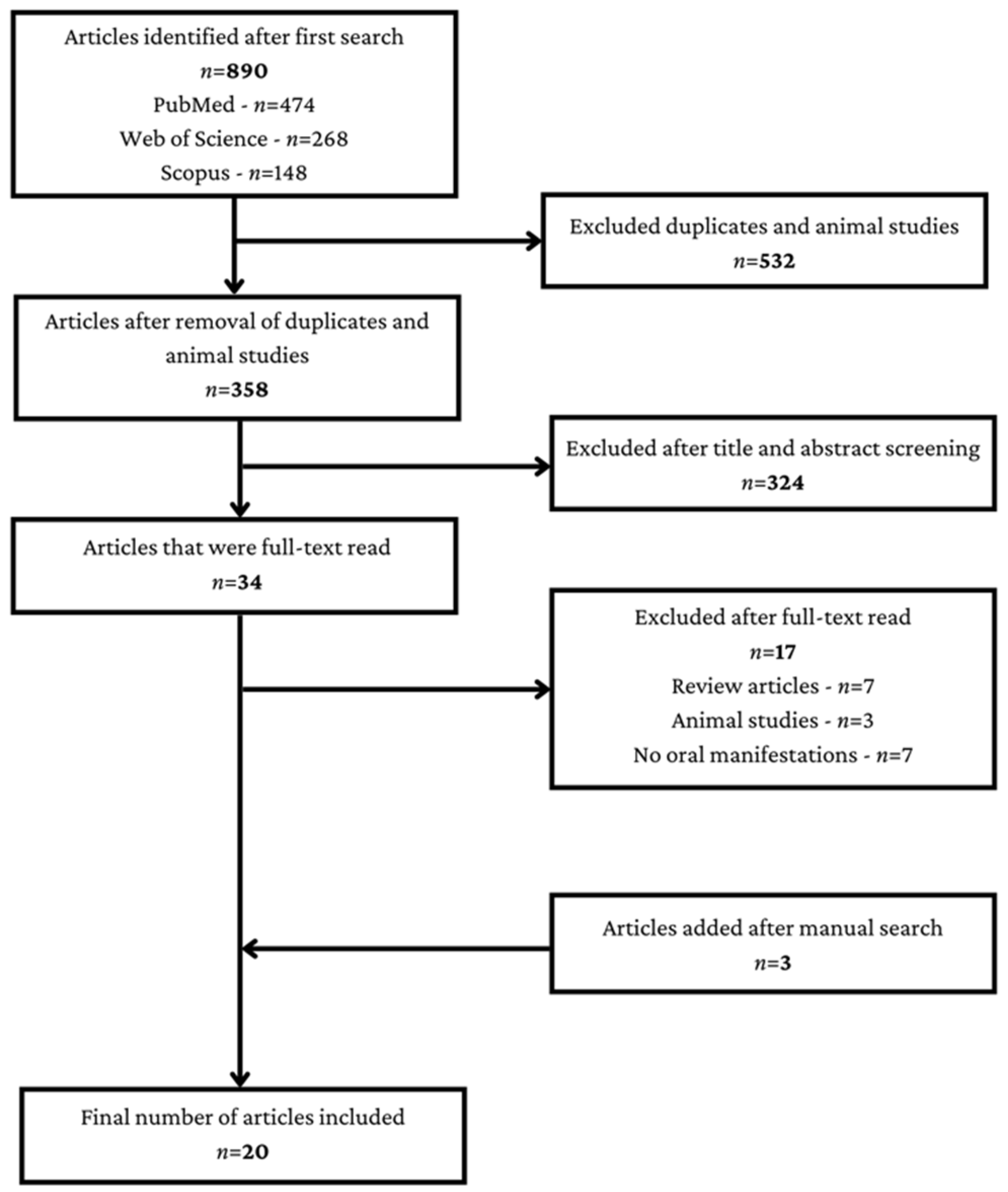
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
3. Narrative Synthesis
3.1. Saliva as a Diagnostic Tool
3.2. Alterations of the Oral Mucosa
3.3. Oral Manifestations in COVID-19 Related Multisystem Inflammatory Syndrome and Kawasaki Disease
3.4. Oral Manifestations in COVID-19 Related Thrombocytopenic Purpura and Erythema Multiforme
3.5. Acute Parotitis
3.6. Oral Harmful Habits during the COVID-19 Pandemic
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aimrane, A.; Laaradia, M.A.; Sereno, D.; Perrin, P.; Draoui, A.; Bougadir, B.; Hadach, M.; Zahir, M.; Fdil, N.; El Hiba, O.; et al. Insight into COVID-19’s epidemiology, pathology, and treatment. Heliyon 2022, 8, e08799. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong, S.E.; Toh, M.P.; Lee, V.J. Presymptomatic Transmission of SARS-CoV-2—Singapore, January 23-March 16, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharroubi, S.; Saleh, F. Are Lockdown Measures Effective Against COVID-19? Front. Public Health 2020, 8, 549692. [Google Scholar] [CrossRef] [PubMed]
- Grech, P.; Grech, R. Covid-19 Restrictive Measures: A Theoretical Exploration of Defiant Attitudes. Issues Ment. Health Nurs. 2021, 42, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Azhar, I.E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health-The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, M.; Corcione, A.; Castellano, F.; Fiori Nastro, F.; Santamaria, F. Coronavirus Disease 2019 in Children. Front. Pediatr. 2021, 9, 668484. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Lozada-Nur, F.; Chainani-Wu, N.; Fortuna, G.; Sroussi, H. Dysgeusia in COVID-19: Possible Mechanisms and Implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 344–346. [Google Scholar] [CrossRef]
- Iranmanesh, B.; Khalili, M.; Amiri, R.; Zartab, H.; Aflatoonian, M. Oral manifestations of COVID-19 disease: A review article. Dermatol. Ther. 2021, 34, e14578. [Google Scholar] [CrossRef] [PubMed]
- Axéll, T. The oral mucosa as a mirror of general health or disease. Scand. J. Dent. Res. 1992, 100, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Guillouet, C.; Riou, M.C.; Duong, L.T.; de La Dure-Molla, M.; Fournier, B.P.J. Oral lesions of viral, bacterial, and fungal diseases in children: A decision tree. Front. Pediatr. 2022, 10, 937808. [Google Scholar] [CrossRef] [PubMed]
- Santosh, A.B.R.; Muddana, K. Viral infections of oral cavity. J. Family Med. Prim. Care 2020, 9, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Arrizabalaga, O.; Otaegui, D.; Vergara, I.; Arrizabalaga, J.; Méndez, E. Open Access of COVID-19-related publications in the first quarter of 2020: A preliminary study based in PubMed. F1000Res. 2020, 9, 649. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- Santos, C.N.; Rezende, K.M.; Oliveira Neto, N.F.; Okay, T.S.; Braz-Silva, P.H.; Bönecker, M. Saliva: An important alternative for screening and monitoring of COVID-19 in children. Braz. Oral Res. 2020, 34, e0125. [Google Scholar] [CrossRef]
- Zhang, C.Z.; Cheng, X.Q.; Li, J.Y.; Zhang, P.; Yi, P.; Xu, X.; Zhou, X.D. Saliva in the diagnosis of diseases. Int. J. Oral Sci. 2016, 8, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Cui, Y.; Yang, M.; Zhu, J.; Zhang, H.; Duan, Z.; Wang, S.; Liao, Z.; Liu, W. Developments in diagnostic applications of saliva in human organ diseases. Med. Nov. Technol. Devices 2022, 13, 100115. [Google Scholar] [CrossRef]
- To, K.K.W.; Chan, K.H.; Ho, J.; Pang, P.K.P.; Ho, D.T.Y.; Chang, A.C.H.; Seng, C.W.; Yip, C.C.Y.; Cheng, V.C.C.; Hung, I.F.N.; et al. Respiratory virus infection among hospitalized adult patients with or without clinically apparent respiratory infection: A prospective cohort study. Clin. Microbiol. Infect. 2019, 25, 1539–1545. [Google Scholar] [CrossRef]
- Muñoz-Prieto, A.; Rubić, I.; Gonzalez-Sanchez, J.C.; Kuleš, J.; Martínez-Subiela, S.; Cerón, J.J.; Bernal, E.; Torres-Cantero, A.; Vicente-Romero, M.R.; Mrljak, V.; et al. Saliva changes in composition associated to COVID-19: A preliminary study. Sci. Rep. 2022, 12, 10879. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Tsang, O.T.; Yip, C.C.; Chan, K.H.; Wu, T.C.; Chan, J.M.; Leung, W.S.; Chik, T.S.; Choi, C.Y.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Martínez, B.; Guzmán-Ortiz, A.L.; Nevárez-Ramírez, A.J.; Parra-Ortega, I.; Olivar-López, V.B.; Ángeles-Floriano, T.; Vilchis-Ordoñez, A.; Quezada, H. Saliva as a promising biofluid for SARS-CoV-2 detection during the early stages of infection. Bol. Med. Hosp. Infant. Mex. 2020, 77, 228–233, English. [Google Scholar] [CrossRef] [PubMed]
- Han, M.S.; Seong, M.W.; Kim, N.; Shin, S.; Cho, S.I.; Park, H.; Kim, T.S.; Park, S.S.; Choi, E.H. Viral RNA Load in Mildly Symptomatic and Asymptomatic Children with COVID-19, Seoul, South Korea. Emerg. Infect. Dis. 2020, 26, 2497–2499. [Google Scholar] [CrossRef]
- Kam, K.Q.; Yung, C.F.; Maiwald, M.; Chong, C.Y.; Soong, H.Y.; Loo, L.H.; Tan, N.W.H.; Li, J.; Nadua, K.D.; Thoon, K.C. Clinical Utility of Buccal Swabs for Severe Acute Respiratory Syndrome Coronavirus 2 Detection in Coronavirus Disease 2019-Infected Children. J. Pediatric Infect. Dis. Soc. 2020, 9, 370–372. [Google Scholar] [CrossRef]
- Moutsopoulos, N.M.; Moutsopoulos, H.M. The oral mucosa: A barrier site participating in tissue-specific and systemic immunity. Oral Dis. 2018, 24, 22–25. [Google Scholar] [CrossRef]
- Kansky, A.A.; Didanovic, V.; Dovsak, T.; Brzak, B.L.; Pelivan, I.; Terlevic, D. Epidemiology of oral mucosal lesions in Slovenia. Radiol. Oncol. 2018, 52, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Bhujel, N.; Zaheer, K.; Singh, R.P. Oral mucosal lesions in patients with COVID-19: A systematic review. Br. J. Oral Maxillofac. Surg. 2021, 59, 1024–1030. [Google Scholar] [CrossRef]
- Amorim Dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; Acevedo, A.C.; De Luca Canto, G.; Sugaya, N.; Santos-Silva, A.R.; Guerra, E.N.S. Oral Manifestations in Patients with COVID-19: A Living Systematic Review. J. Dent. Res. 2021, 100, 141–154. [Google Scholar] [CrossRef]
- Neskovic, I.; Vujkov, S.; Bradic Vasic, M.; Blagojevic, D.; Komsic, J. Oral manifestations of COVID-19 infection in children—A case report. Med. Pregl. 2021, 74, 187–190. [Google Scholar] [CrossRef]
- Aghazadeh, N.; Homayouni, M.; Sartori-Valinotti, J.C. Oral vesicles and acral erythema: Report of a cutaneous manifestation of COVID-19. Int. J. Dermatol. 2020, 59, 1153–1154. [Google Scholar] [CrossRef] [PubMed]
- Cant, A.; Bhujel, N.; Harrison, M. Oral ulceration as presenting feature of paediatric inflammatory multisystem syndrome associated with COVID-19. Br. J. Oral Maxillofac. Surg. 2020, 58, 1058–1059. [Google Scholar] [CrossRef] [PubMed]
- Bowe, S.; O’Connor, C.; Gleeson, C.; Murphy, M. Reactive infectious mucocutaneous eruption in children diagnosed with COVID-19. Pediatr. Dermatol. 2021, 38, 1385–1386. [Google Scholar] [CrossRef] [PubMed]
- Bardellini, E.; Bondioni, M.P.; Amadori, F.; Veneri, F.; Lougaris, V.; Meini, A.; Plebani, A.; Majorana, A. Non-specific oral and cutaneous manifestations of Coronavirus Disease 2019 in children. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e549–e553. [Google Scholar] [CrossRef]
- Patil, S.; Rao, R.S.; Majumdar, B.; Anil, S. Clinical Appearance of Oral Candida Infection and Therapeutic Strategies. Front. Microbiol. 2015, 6, 1391. [Google Scholar] [CrossRef] [Green Version]
- González-Álvarez, L.; García-Pola, M.J.; Garcia-Martin, J.M. Geographic tongue: Predisposing factors, diagnosis and treatment. A systematic review. Rev. Clin. Esp. (Barc). 2018, 218, 481–488, English, Spanish. [Google Scholar] [CrossRef]
- Seerangaiyan, K.; Jüch, F.; Winkel, E.G. Tongue coating: Its characteristics and role in intra-oral halitosis and general health-a review. J. Breath Res. 2018, 12, 034001. [Google Scholar] [CrossRef]
- Dima, M.; Enatescu, I.; Craina, M.; Petre, I.; Iacob, E.R.; Iacob, D. First neonates with severe acute respiratory syndrome coronavirus 2 infection in Romania: Three case reports. Medicine (Baltimore) 2020, 99, e21284. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N. Multisystem Inflammatory Syndrome in Children Related to SARS-CoV-2. Paediatr. Drugs 2021, 23, 119–129. [Google Scholar] [CrossRef]
- Royal College of Paediatrics and Child Health. Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19; Royal College of Paediatrics and Child Health: London, UK, 2020; Available online: https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%20inflammatory%20syndrome-20200501.pdf (accessed on 9 November 2022).
- Centers for Disease Control and Prevention. Information for Healthcare Providers about Multisystem Inflammatory Syndrome in Children (MIS-C). Available online: cdc.gov/mis-c/hcp/ (accessed on 9 November 2022).
- Jiang, L.; Tang, K.; Irfan, O.; Li, X.; Zhang, E.; Bhutta, Z. Epidemiology, Clinical Features, and Outcomes of Multisystem Inflammatory Syndrome in Children (MIS-C) and Adolescents-a Live Systematic Review and Meta-analysis. Curr. Pediatr. Rep. 2022, 10, 19–30. [Google Scholar] [CrossRef]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. Multisystem Inflammatory Syndrome in Children in New York State. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef]
- Lee, E.H.; Kepler, K.L.; Geevarughese, A.; Paneth-Pollak, R.; Dorsinville, M.S.; Ngai, S.; Reilly, K.H. Race/Ethnicity Among Children With COVID-19-Associated Multisystem Inflammatory Syndrome. JAMA Netw. Open 2020, 3, e2030280. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.B.; Gilani, Z.; Godfred-Cato, S.; Belay, E.D.; Feldstein, L.R.; Patel, M.M.; Randolph, A.G.; Newhams, M.; Thomas, D.; Magleby, R.; et al. Incidence of Multisystem Inflammatory Syndrome in Children Among US Persons Infected With SARS-CoV-2. JAMA Netw. Open 2021, 4, e2116420. [Google Scholar] [CrossRef] [PubMed]
- Sobh, A.; Madiha, A.; Abdelrahman, A.M.; Mosa, D.M. COVID-19 diversity: A case of multisystem inflammatory syndrome in children masquerading as juvenile systemic lupus erythematosus. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221131981. [Google Scholar] [CrossRef] [PubMed]
- Al Ameer, H.H.; Al Kadhem, S.M.; Busaleh, F.; Al Khwaitm, S.; Llaguno, M.B.B. Multisystem Inflammatory Syndrome in Children Temporally Related to COVID-19: A Case Report From Saudi Arabia. Cureus 2020, 12, e10589. [Google Scholar] [CrossRef] [PubMed]
- Halepas, S.; Lee, K.C.; Myers, A.; Yoon, R.K.; Chung, W.; Peters, S.M. Oral manifestations of COVID-2019-related multisystem inflammatory syndrome in children: A review of 47 pediatric patients. J. Am. Dent. Assoc. 2021, 152, 202–208. [Google Scholar] [CrossRef]
- Rife, E.; Gedalia, A. Kawasaki Disease: An Update. Curr. Rheumatol. Rep. 2020, 22, 75. [Google Scholar] [CrossRef]
- Greco, A.; De Virgilio, A.; Rizzo, M.I.; Tombolini, M.; Gallo, A.; Fusconi, M.; Ruoppolo, G.; Pagliuca, G.; Martellucci, S.; de Vincentiis, M. Kawasaki disease: An evolving paradigm. Autoimmun. Rev. 2015, 14, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Rowley, A.H. Kawasaki disease: Novel insights into etiology and genetic susceptibility. Annu. Rev. Med. 2011, 62, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Bayers, S.; Shulman, S.T.; Paller, A.S. Kawasaki disease: Part II. Complications and treatment. J. Am. Acad. Dermatol. 2013, 69, 513.e1–8; quiz 521–2. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: Prospective observational study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef] [PubMed]
- Grimaud, M.; Starck, J.; Levy, M.; Marais, C.; Chareyre, J.; Khraiche, D.; Leruez-Ville, M.; Quartier, P.; Léger, P.L.; Geslain, G.; et al. Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children. Ann. Intensive Care. 2020, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, L.Y.; Burns, J.C.; Shulman, S.T.; Bolger, A.F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004, 110, 2747–2771. [Google Scholar] [CrossRef] [Green Version]
- Çakan, M.; Aktay Ayaz, N.; Keskindemirci, G.; Onan, S.H.; Aköz Saydam, F. A Case of Kawasaki Disease With Severe Lip and Oral Mucosa Involvement Complicated With Microstomia and Corrected With Surgery. Arch. Rheumatol. 2017, 33, 238–240. [Google Scholar] [CrossRef] [PubMed]
- Akca, U.K.; Kesici, S.; Ozsurekci, Y.; Aykan, H.H.; Batu, E.D.; Atalay, E.; Demir, S.; Sag, E.; Vuralli, D.; Bayrakci, B.; et al. Kawasaki-like disease in children with COVID-19. Rheumatol. Int. 2020, 40, 2105–2115. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.G.; Mills, M.; Suarez, D.; Hogan, C.A.; Yeh, D.; Segal, J.B.; Nguyen, E.L.; Barsh, G.R.; Maskatia, S.; Mathew, R. COVID-19 and Kawasaki Disease: Novel Virus and Novel Case. Hosp. Pediatr. 2020, 10, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Labé, P.; Ly, A.; Sin, C.; Nasser, M.; Chapelon-Fromont, E.; Ben Saïd, P.; Mahé, E. Erythema multiforme and Kawasaki disease associated with COVID-19 infection in children. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e539–e541. [Google Scholar] [CrossRef]
- Falah, N.U.; Hashmi, S.; Ahmed, Z.; Jaan, A.; Akhtar, A.; Khalid, F.; Farooque, U.; Shera, M.T.; Ali, S.; Javed, A. Kawasaki Disease-Like Features in 10 Pediatric COVID-19 Cases: A Retrospective Study. Cureus 2020, 12, e11035. [Google Scholar] [CrossRef]
- Riad, A.; Boccuzzi, M.; Sagiroglu, D.; Klugar, M.; Krsek, M. Pediatric multisystem inflammatory syndrome temporally associated with SARS-COV-2: Oral manifestations and implications. Int. J. Paediatr. Dent. 2021, 31, 35–36. [Google Scholar] [CrossRef]
- Marinescu, A.R.; Lazureanu, V.E.; Musta, V.F.; Nicolescu, N.D.; Mocanu, A.; Cut, T.G.; Muresan, C.O.; Tudoran, C.; Licker, M.; Laza, R. Severe Thrombocytopenic Purpura Associated with COVID-19 in a Pediatric Patient. Infect. Drug Resist. 2022, 15, 3405–3415. [Google Scholar] [CrossRef]
- Zainal, A.; Salama, A.; Alweis, R. Immune thrombocytopenic purpura. J. Community Hosp. Intern. Med. Perspect. 2019, 9, 59–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohn, J.P.; Steurer, M. Current and evolving treatment strategies in adult immune thrombocytopenia. Memo-Mag. Eur. Med. Oncol. 2018, 11, 241–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, N.; Ghanima, W. Immune Thrombocytopenia. N. Engl. J. Med. 2019, 381, 945–955. [Google Scholar] [CrossRef] [PubMed]
- McCrae, K. Immune thrombocytopenia: No longer ‘idiopathic. CCJM 2011, 78, 358–373. [Google Scholar] [CrossRef] [Green Version]
- Trayes, K.P.; Love, G.; Studdiford, J.S. Erythema Multiforme: Recognition and Management. Am. Fam. Physician 2019, 100, 82–88. [Google Scholar]
- Lamoreux, M.R.; Sternbach, M.R.; Hsu, W.T. Erythema multiforme. Am. Fam. Physician 2006, 74, 1883–1888. [Google Scholar] [PubMed]
- Brook, I. Acute bacterial suppurative parotitis: Microbiology and management. J. Craniofac. Surg. 2003, 14, 37–40. [Google Scholar] [CrossRef]
- Capaccio, P.; Pignataro, L.; Corbellino, M.; Popescu-Dutruit, S.; Torretta, S. Acute Parotitis: A Possible Precocious Clinical Manifestation of SARS-CoV-2 Infection? Otolaryngol. Head Neck Surg. 2020, 163, 182–183. [Google Scholar] [CrossRef]
- Fisher, J.; Monette, D.L.; Patel, K.R.; Kelley, B.P.; Kennedy, M. COVID-19 associated parotitis. Am. J. Emerg. Med. 2021, 39, 254.e1–254.e3. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chetrit, A.; Chekkoury-Idrissi, Y.; Distinguin, L.; Circiu, M.; Saussez, S.; Berradja, N.; Edjlali, M.; Hans, S.; Carlier, R. Parotitis-Like Symptoms Associated with COVID-19, France, March-April 2020. Emerg. Infect. Dis. 2020, 26, 2270–2271. [Google Scholar] [CrossRef]
- Jongyotha, K.; Rana, S. Acute parotitis in an older adult with COVID-19. J. Am. Geriatr. Soc. 2021, 69 (Suppl. 1), S21. [Google Scholar]
- Elbadawi, L.I.; Talley, P.; Rolfes, M.A.; Millman, A.J.; Reisdorf, E.; Kramer, N.A.; Barnes, J.R.; Blanton, L.; Christensen, J.; Cole, S.; et al. Non-mumps Viral Parotitis During the 2014-2015 Influenza Season in the United States. Clin. Infect. Dis. 2018, 67, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Sasithorn, L. COVID-19 Associated Parotitis in a 4-Year-Old Boy. J. Paediatr. Child Health 2022, 58, 1911–1912. [Google Scholar] [CrossRef]
- Brehm, R.; Narayanam, L.; Chon, G. COVID-19-Associated Parotitis in a 10-Week-Old Male. Cureus 2022, 14, e31054. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef]
- Pereira, T.S.; Oliveira, F.; Cardoso, M.C.A.F. Association between harmful oral habits and the structures and functions of the stomatognathic system: Perception of parents/guardians. Codas 2017, 29, e20150301. [Google Scholar] [CrossRef] [Green Version]
- Kamdar, R.J.; Al-Shahrani, I. Damaging oral habits. J. Int. Oral Health 2015, 7, 85–87. [Google Scholar]
- Quashie-Williams, R.; daCosta, O.O.; Isiekwe, M.C. Oral habits, prevalence and effects on occlusion of 4–15 year old school children in Lagos, Nigeria. Niger. Postgrad. Med. J. 2010, 17, 113–117. [Google Scholar]
- Caruso, S.; Nota, A.; Darvizeh, A.; Severino, M.; Gatto, R.; Tecco, S. Poor oral habits and malocclusions after usage of orthodontic pacifiers: An observational study on 3-5 years old children. BMC Pediatr. 2019, 19, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolcakoglu, K.; Yucel, G. Anxiety and harmful oral habits in preschool children during the 2020 first-wave COVID-19 lockdown in Turkey. Dent. Med. Probl. 2021, 58, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, Y.; Liu, Z.H.; Zhao, Y.J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.T. Progression of Mental Health Services during the COVID-19 Outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elaraby, A.; Shahein, M.; Bekhet, A.H.; Perrin, P.B.; Gorgey, A.S. The COVID-19 pandemic impacts all domains of quality of life in Egyptians with spinal cord injury: A retrospective longitudinal study. Spinal Cord 2022, 60, 757–762. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Sanchez-Ramirez, D.C.; Normand, K.; Zhaoyun, Y.; Torres-Castro, R. Long-Term Impact of COVID-19: A Systematic Review of the Literature and Meta-Analysis. Biomedicines 2021, 9, 900. [Google Scholar] [CrossRef]
- Jiang, P.; Klemeš, J.J.; Fan, Y.V.; Fu, X.; Bee, Y.M. More Is Not Enough: A Deeper Understanding of the COVID-19 Impacts on Healthcare, Energy and Environment Is Crucial. Int. J. Environ. Res. Public Health 2021, 18, 684. [Google Scholar] [CrossRef]
- Mouffak, S.; Shubbar, Q.; Saleh, E.; El-Awady, R. Recent advances in management of COVID-19: A review. Biomed. Pharmacother. 2021, 143, 112107. [Google Scholar] [CrossRef]
- Rahmani, A.M.; Mirmahaleh, S.Y.H. Coronavirus disease (COVID-19) prevention and treatment methods and effective parameters: A systematic literature review. Sustain. Cities Soc. 2021, 64, 102568. [Google Scholar] [CrossRef]
- Girum, T.; Lentiro, K.; Geremew, M.; Migora, B.; Shewamare, S.; Shimbre, M.S. Optimal strategies for COVID-19 prevention from global evidence achieved through social distancing, stay at home, travel restriction and lockdown: A systematic review. Arch. Public Health 2021, 79, 150. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moca, A.E.; Juncar, R.I.; Moca, R.T.; Bota, T.; Sabău, D.T.; Juncar, M. Oral Manifestations in Children Diagnosed with COVID-19: A Narrative Review. Healthcare 2023, 11, 288. https://doi.org/10.3390/healthcare11030288
Moca AE, Juncar RI, Moca RT, Bota T, Sabău DT, Juncar M. Oral Manifestations in Children Diagnosed with COVID-19: A Narrative Review. Healthcare. 2023; 11(3):288. https://doi.org/10.3390/healthcare11030288
Chicago/Turabian StyleMoca, Abel Emanuel, Raluca Iulia Juncar, Rahela Tabita Moca, Teofana Bota, Denisa Tabita Sabău, and Mihai Juncar. 2023. "Oral Manifestations in Children Diagnosed with COVID-19: A Narrative Review" Healthcare 11, no. 3: 288. https://doi.org/10.3390/healthcare11030288