
Towards Non-Invasive and Continuous Blood Pressure Monitoring in Neonatal Intensive Care Using Artificial Intelligence: A Narrative Review


Abstract
:1. Introduction
2. Materials and Methods
3. Results
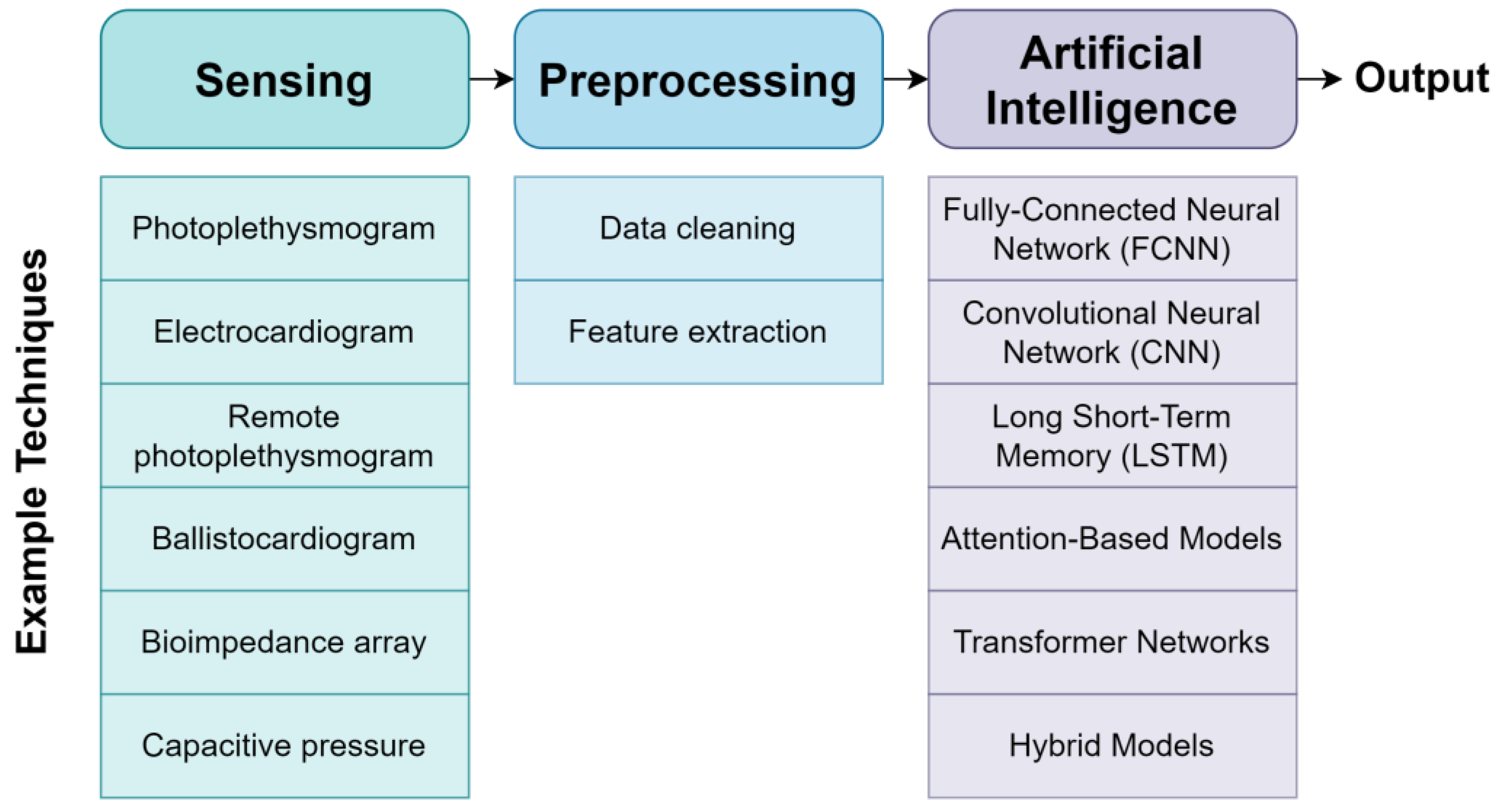
3.1. Architecture for Non-Invasive Blood Pressure Monitoring
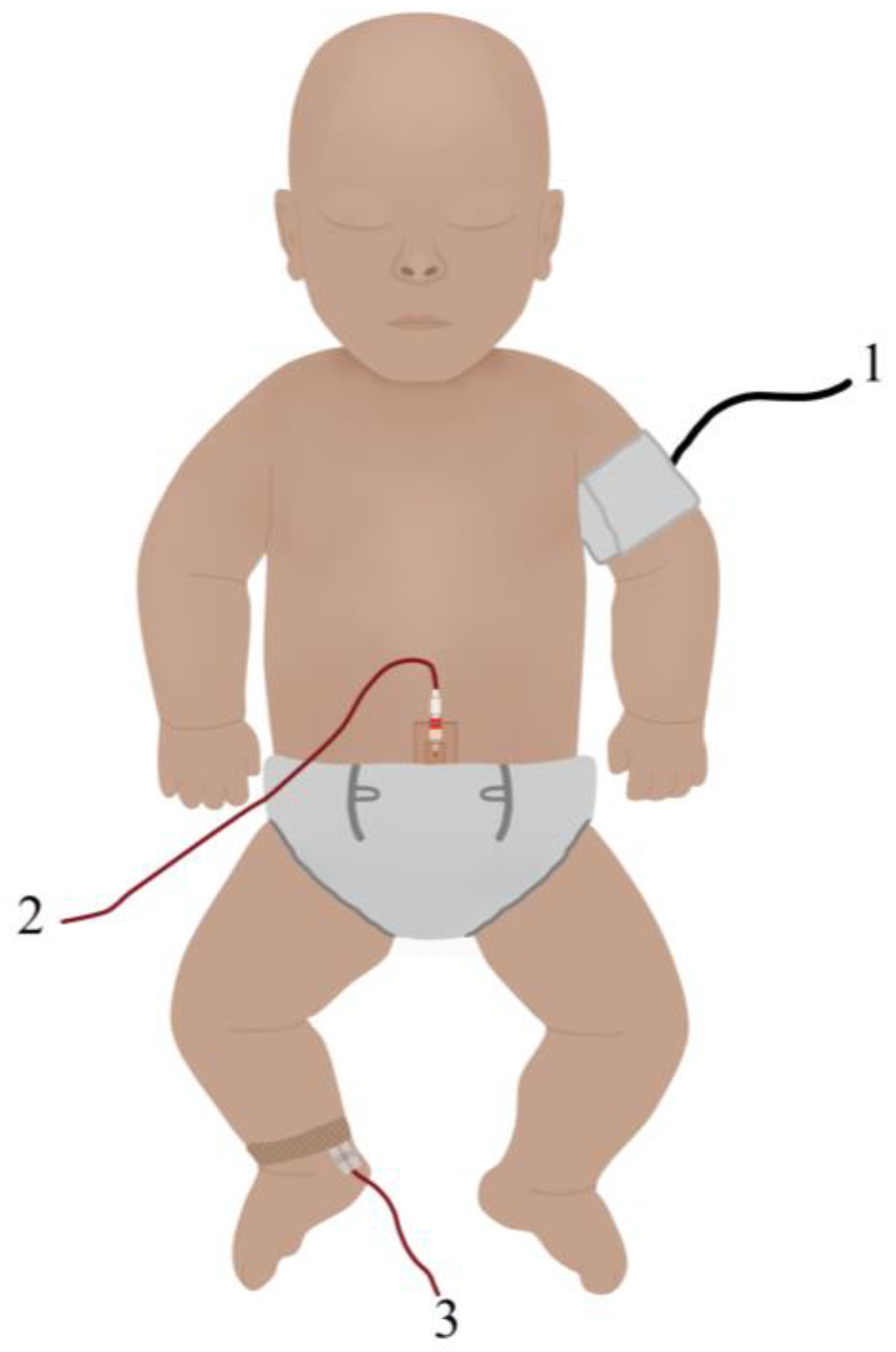
3.1.1. Sensors
3.1.2. Artificial Intelligence
3.1.3. Assessment Metrics
3.2. Non-Invasive Blood Pressure Monitoring in Neonatal Cohorts
3.3. Limitations
4. Opportunities for Translational Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walani, S.R. Global burden of preterm birth. Int. J. Gynecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; Brown, K.; Newnham, J. The Australian Preterm Birth Prevention Alliance. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Sangla, A.; Kandasamy, Y. Effects of prematurity on long-term renal health: A systematic review. BMJ Open 2021, 11, e047770. [Google Scholar] [CrossRef] [PubMed]
- DeMers, D.; Wachs, D. Physiology, Mean Arterial Pressure; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Murphy, E.; Healy, D.B.; Chioma, R.; Dempsey, E.M. Evaluation of the Hypotensive Preterm Infant: Evidence-Based Practice at the Bedside? Children 2023, 10, 519. [Google Scholar] [CrossRef]
- Dasgupta, S.J.; Gill, A.B. Hypotension in the very low birthweight infant: The old, the new, and the uncertain. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F450–F454. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, E.M. What Should We Do about Low Blood Pressure in Preterm Infants. Neonatology 2017, 111, 402–407. [Google Scholar] [CrossRef]
- Nakamura, M.; Umehara, N.; Ishii, K.; Sasahara, J.; Kiyoshi, K.; Ozawa, K.; Tanaka, K.; Tanemoto, T.; Ichizuka, K.; Hasegawa, J.; et al. A poor long-term neurological prognosis is associated with abnormal cord insertion in severe growth-restricted fetuses. J. Perinat. Med. 2018, 46, 1040–1047. [Google Scholar] [CrossRef]
- Dionne, J.M.; Bremner, S.A.; Baygani, S.K.; Batton, B.; Ergenekon, E.; Bhatt-Mehta, V.; Dempsey, E.; Kluckow, M.; Koplowitz, L.P.; Apele-Freimane, D.; et al. Method of Blood Pressure Measurement in Neonates and Infants: A Systematic Review and Analysis. J. Pediatr. 2020, 221, 23–31.e5. [Google Scholar] [CrossRef]
- Wu, J.; Mu, D. Vascular catheter-related complications in newborns. J. Paediatr. Child Health 2012, 48, E91–E95. [Google Scholar] [CrossRef]
- Xu, S.; Rwei, A.Y.; Vwalika, B.; Chisembele, M.P.; Stringer, J.S.A.; Ginsburg, A.S.; Rogers, J.A. Wireless skin sensors for physiological monitoring of infants in low-income and middle-income countries. Lancet Digit. Health 2021, 3, e266–e273. [Google Scholar] [CrossRef]
- Di Biase, M.; Casani, A.; Orfeo, L. Invasive arterial blood pressure in the neonatal intensive care: A valuable tool to manage very ill preterm and term neonates. Ital. J. Pediatr. 2015, 41, A9. [Google Scholar] [CrossRef]
- Baker, S.; Xiang, W.; Atkinson, I. A Hybrid Neural Network for Continuous and Non-invasive Estimation of Blood Pressure from Raw Electrocardiogram and Photoplethysmogram Waveforms. Comput. Methods Programs Biomed. 2021, 207, 106191. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Xiang, W.; Atkinson, I. A computationally efficient CNN-LSTM neural network for estimation of blood pressure from features of electrocardiogram and photoplethysmogram waveforms. Knowl.-Based Syst. 2022, 250, 109151. [Google Scholar] [CrossRef]
- Mousavi, S.S.; Firouzmand, M.; Charmi, M.; Hemmati, M.; Moghadam, M.; Ghorbani, Y. Blood pressure estimation from appropriate and inappropriate PPG signals using A whole-based method. Biomed. Signal Process. Control 2019, 47, 196–206. [Google Scholar] [CrossRef]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of Non-Invasive Blood Pressure Prediction from PPG and rPPG Signals Using Deep Learning. Sensors 2021, 21, 6022. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Tang, K.; Hsu, Y.-C.; Huang, T.; Wang, D.; Li, W.; Savitz, S.I.; Jiang, X.; Shams, S. Non-invasive arterial blood pressure measurement and SpO2 estimation using PPG signal: A deep learning framework. BMC Med. Inform. Decis. Mak. 2023, 23, 131. [Google Scholar] [CrossRef]
- Miao, F.; Wen, B.; Hu, Z.; Fortino, G.; Wang, X.-P.; Liu, Z.-D.; Tang, M.; Li, Y. Continuous Blood Pressure Measurement from One-Channel Electrocardiogram Signal Using Deep-Learning Techniques. Artif. Intell. Med. 2020, 108, 101919. [Google Scholar] [CrossRef] [PubMed]
- Shoeibi, F.; Najafiaghdam, E.; Ebrahimi, A. Nonlinear features of photoplethysmography signals for Non-invasive blood pressure estimation. Biomed. Signal Process. Control 2023, 85, 105067. [Google Scholar] [CrossRef]
- Ibrahim, B.; Jafari, R. Cuffless blood pressure monitoring from a wristband with calibration-free algorithms for sensing location based on bio-impedance sensor array and autoencoder. Sci. Rep. 2022, 12, 319. [Google Scholar] [CrossRef]
- Sel, K.; Osman, D.; Huerta, N.; Edgar, A.; Pettigrew, R.I.; Jafari, R. Continuous cuffless blood pressure monitoring with a wearable ring bioimpedance device. NPJ Digit. Med. 2023, 6, 59. [Google Scholar] [CrossRef]
- Si, S.; Sun, C.; Wang, H.; Wu, H.; Chen, L.; Xia, Y.; Qin, J.; Wu, Y.; Yang, J. Unconstrained blood pressure monitoring based on a neural network–assisted multistage pressure textile sensor. Nano Energy 2023, 115, 108730. [Google Scholar] [CrossRef]
- Sempionatto, J.R.; Lin, M.; Yin, L.; De la Paz, E.; Pei, K.; Sonsa-Ard, T.; Silva, A.N.d.L.; Khorshed, A.A.; Zhang, F.; Tostado, N.; et al. An epidermal patch for the simultaneous monitoring of haemodynamic and metabolic biomarkers. Nat. Biomed. Eng. 2021, 5, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.U.; Rwei, A.Y.; Hourlier-Fargette, A.; Xu, S.; Lee, K.; Dunne, E.C.; Xie, Z.; Liu, C.; Carlini, A.; Kim, D.H.; et al. Skin-interfaced biosensors for advanced wireless physiological monitoring in neonatal and pediatric intensive-care units. Nat. Med. 2020, 26, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuffless Blood Pressure Estimation Algorithms for Continuous Health-Care Monitoring. IEEE Trans. Biomed. Eng. 2017, 64, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.-Z.; Kang, J.M.; Kwon, Y.; Park, S.; Noh, S.; Kim, Y.; Park, J.; Hwang, S.W. Cuff-Less Blood Pressure Estimation Using Pulse Waveform Analysis and Pulse Arrival Time. IEEE J. Biomed. Heal. Inform. 2018, 22, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, I.; Goudarzi, S.; Khodabakhshi, M.B. A novel dynamical approach in continuous cuffless blood pressure estimation based on ECG and PPG signals. Artif. Intell. Med. 2019, 97, 143–151. [Google Scholar] [CrossRef] [PubMed]
- El-Hajj, C.; Kyriacou, P. Deep learning models for cuffless blood pressure monitoring from PPG signals using attention mechanism. Biomed. Signal Process. Control 2021, 65, 102301. [Google Scholar] [CrossRef]
- Rao, A.; Eskandar-Afshari, F.; Weiner, Y.; Billman, E.; McMillin, A.; Sella, N.; Roxlo, T.; Liu, J.; Leong, W.; Helfenbein, E.; et al. Clinical Study of Continuous Non-Invasive Blood Pressure Monitoring in Neonates. Sensors 2023, 23, 3690. [Google Scholar] [CrossRef]
- Joshi, R.; Bierling, B.L.; Long, X.; Weijers, J.; Feijs, L.; Van Pul, C.; Andriessen, P. A Ballistographic Approach for Continuous and Non-Obtrusive Monitoring of Movement in Neonates. IEEE J. Transl. Eng. Health Med. 2018, 6, 2700809. [Google Scholar] [CrossRef]
- Lo, B.P.; Ip, H.; Yang, G.-Z. Transforming Health Care: Body Sensor Networks, Wearables, and the Internet of Things. IEEE Pulse 2016, 7, 4–8. [Google Scholar] [CrossRef]
- Rong, M.; Li, K. A multi-type features fusion neural network for blood pressure prediction based on photoplethysmography. Biomed. Signal Process. Control 2021, 68, 102772. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Xu, Y.; Song, R.; Liu, Y.; Li, C.; Chen, X. Prediction of arterial blood pressure waveforms from photoplethysmogram signals via fully convolutional neural networks. Comput. Biol. Med. 2021, 138, 104877. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Petrie, J.; Littler, W.; De Swiet, M.; Padfield, P.L.; Altman, D.G.; Bland, M.; Coats, A.; Atkins, N. Short report: An outline of the revised british hypertension society protocol for the evaluation of blood pressure measuring devices. J. Hypertens. 1993, 11, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Association for the Advancement of Medical Instrumentation. American National Standard for Electronic or Automated Sphygmomanometers; Association for the Advancement of Medical Instrumentation: Arlington, VA, USA, 1987. [Google Scholar]
- Quan, X.; Liu, J.; Roxlo, T.; Siddharth, S.; Leong, W.; Muir, A.; Cheong, S.-M.; Rao, A. Advances in Non-Invasive Blood Pressure Monitoring. Sensors 2021, 21, 4273. [Google Scholar] [CrossRef] [PubMed]
- Revathi, K.P.; Manikandan, T. A Smart and Secured Approach for Children’s Health Monitoring Using Machine Learning Techniques Enhancing Data Privacy. IETE J. Res. 2023, 69, 1210–1221. [Google Scholar] [CrossRef]
- Kapur, G.; Chen, L.; Xu, Y.; Cashen, K.D.; Clark, J.; Feng, X.; Wu, S.F. Noninvasive Determination of Blood Pressure by Heart Sound Analysis Compared With Intra-Arterial Monitoring in Critically Ill Children—A Pilot Study of a Novel Approach. Pediatr. Crit. Care Med. 2019, 20, 809–816. [Google Scholar] [CrossRef]
- Maqsood, S.; Xu, S.; Tran, S.; Garg, S.; Springer, M.; Karunanithi, M.; Mohawesh, R. A survey: From shallow to deep machine learning approaches for blood pressure estimation using biosensors. Expert Syst. Appl. 2022, 197, 116788. [Google Scholar] [CrossRef]
- Zhao, L.; Liang, C.; Huang, Y.; Zhou, G.; Xiao, Y.; Ji, N.; Zhang, Y.-T.; Zhao, N. Emerging sensing and modeling technologies for wearable and cuffless blood pressure monitoring. NPJ Digit. Med. 2023, 6, 93. [Google Scholar] [CrossRef]
- Boland, R.A.; Davis, P.G.; Dawson, J.A.; Doyle, L.W. Outcomes of infants born at 22–27 weeks’ gestation in Victoria according to outborn/inborn birth status. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F153–F161. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Blood Pressure Monitor Grade | % Measurements with Mean Absolute Error of: | ||
|---|---|---|---|
| ≤5 mmHg | ≤10 mmHg | ≤15 mmHg | |
| A | 60% | 85% | 95% |
| B | 50% | 75% | 90% |
| C | 40% | 65% | 80% |
| D | Worse than C | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baker, S.; Yogavijayan, T.; Kandasamy, Y. Towards Non-Invasive and Continuous Blood Pressure Monitoring in Neonatal Intensive Care Using Artificial Intelligence: A Narrative Review. Healthcare 2023, 11, 3107. https://doi.org/10.3390/healthcare11243107
Baker S, Yogavijayan T, Kandasamy Y. Towards Non-Invasive and Continuous Blood Pressure Monitoring in Neonatal Intensive Care Using Artificial Intelligence: A Narrative Review. Healthcare. 2023; 11(24):3107. https://doi.org/10.3390/healthcare11243107
Chicago/Turabian StyleBaker, Stephanie, Thiviya Yogavijayan, and Yogavijayan Kandasamy. 2023. "Towards Non-Invasive and Continuous Blood Pressure Monitoring in Neonatal Intensive Care Using Artificial Intelligence: A Narrative Review" Healthcare 11, no. 24: 3107. https://doi.org/10.3390/healthcare11243107