
Umbilical Cord Diseases Affecting Obstetric and Perinatal Outcomes

 , , and
, , and 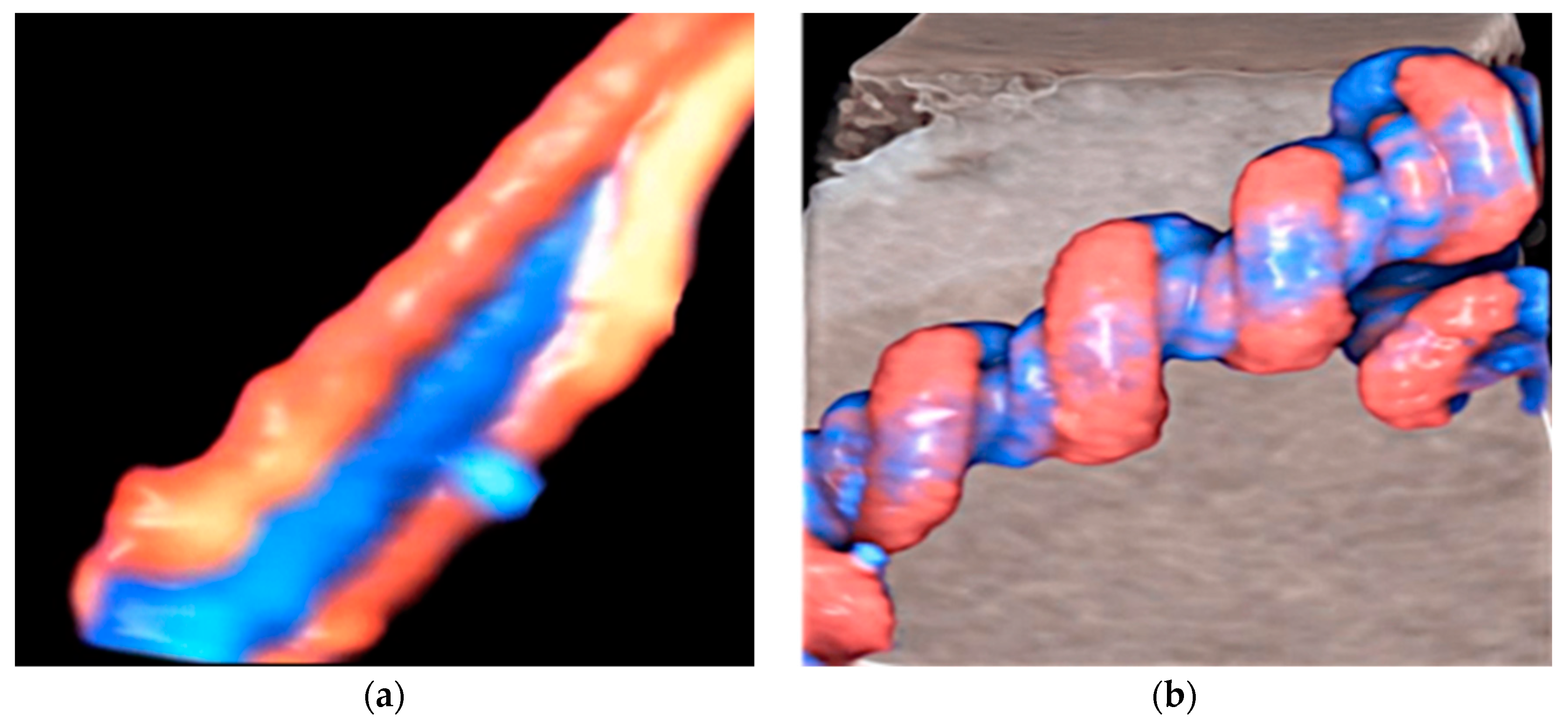{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Umbilical Cord Diseases
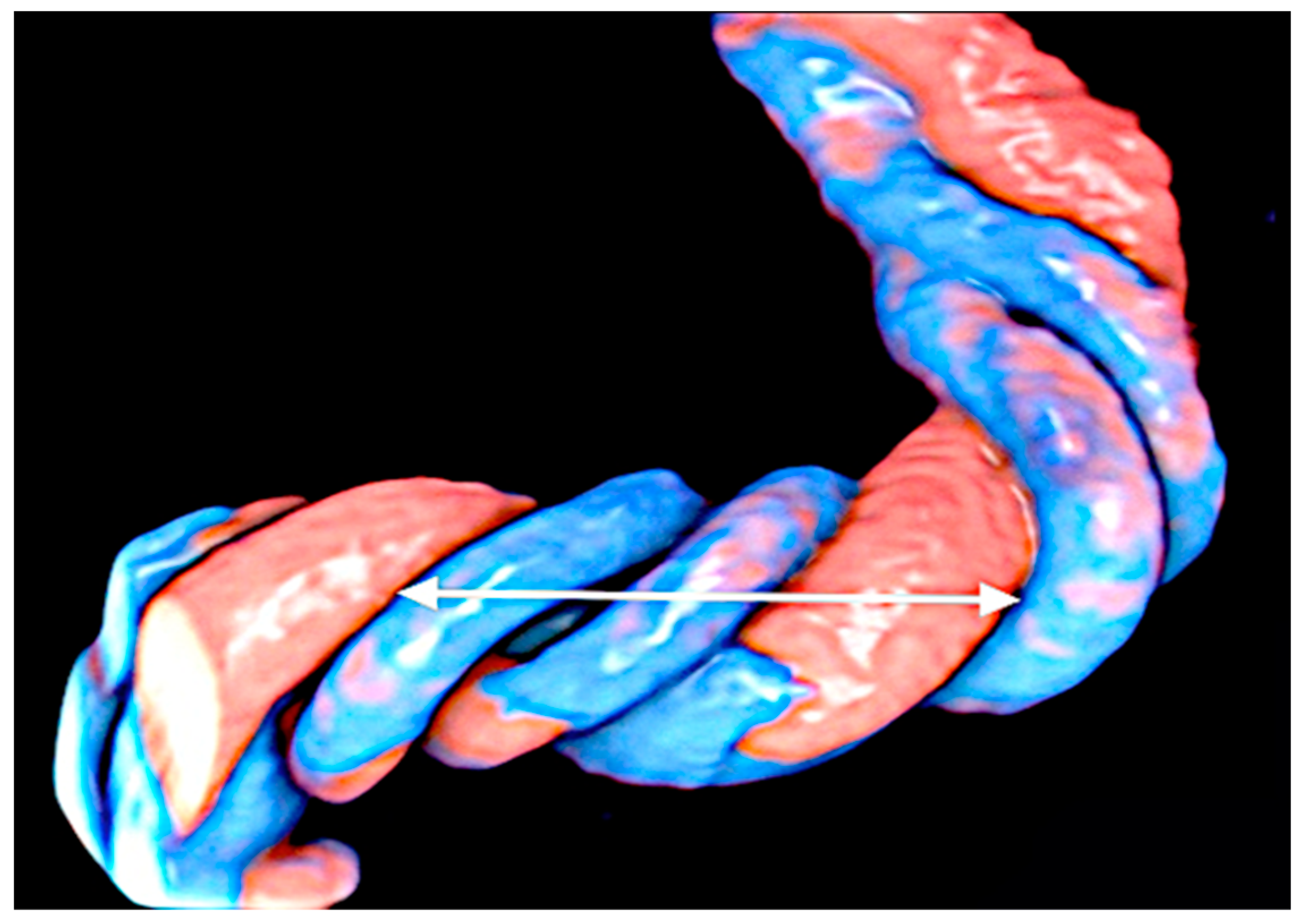
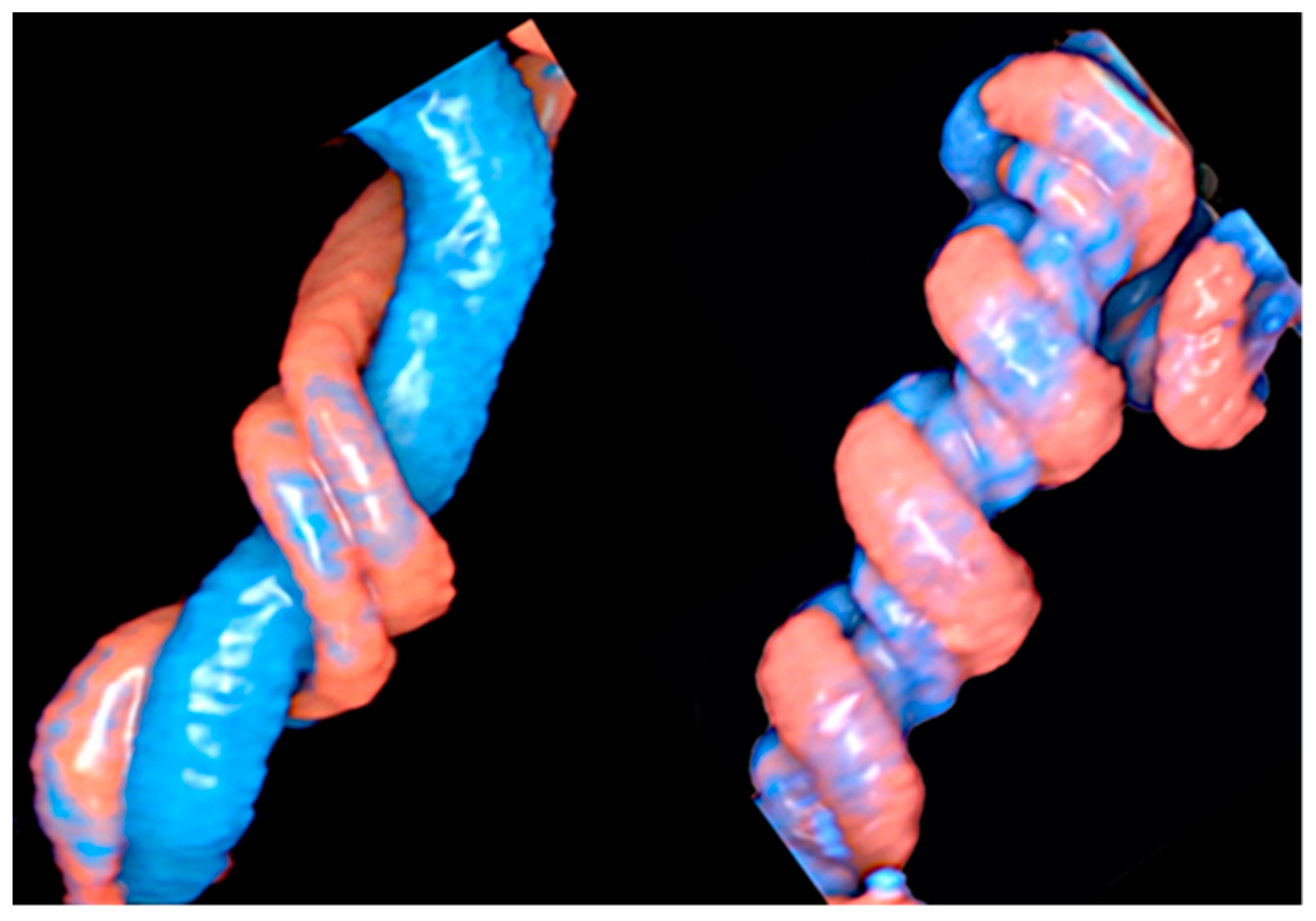
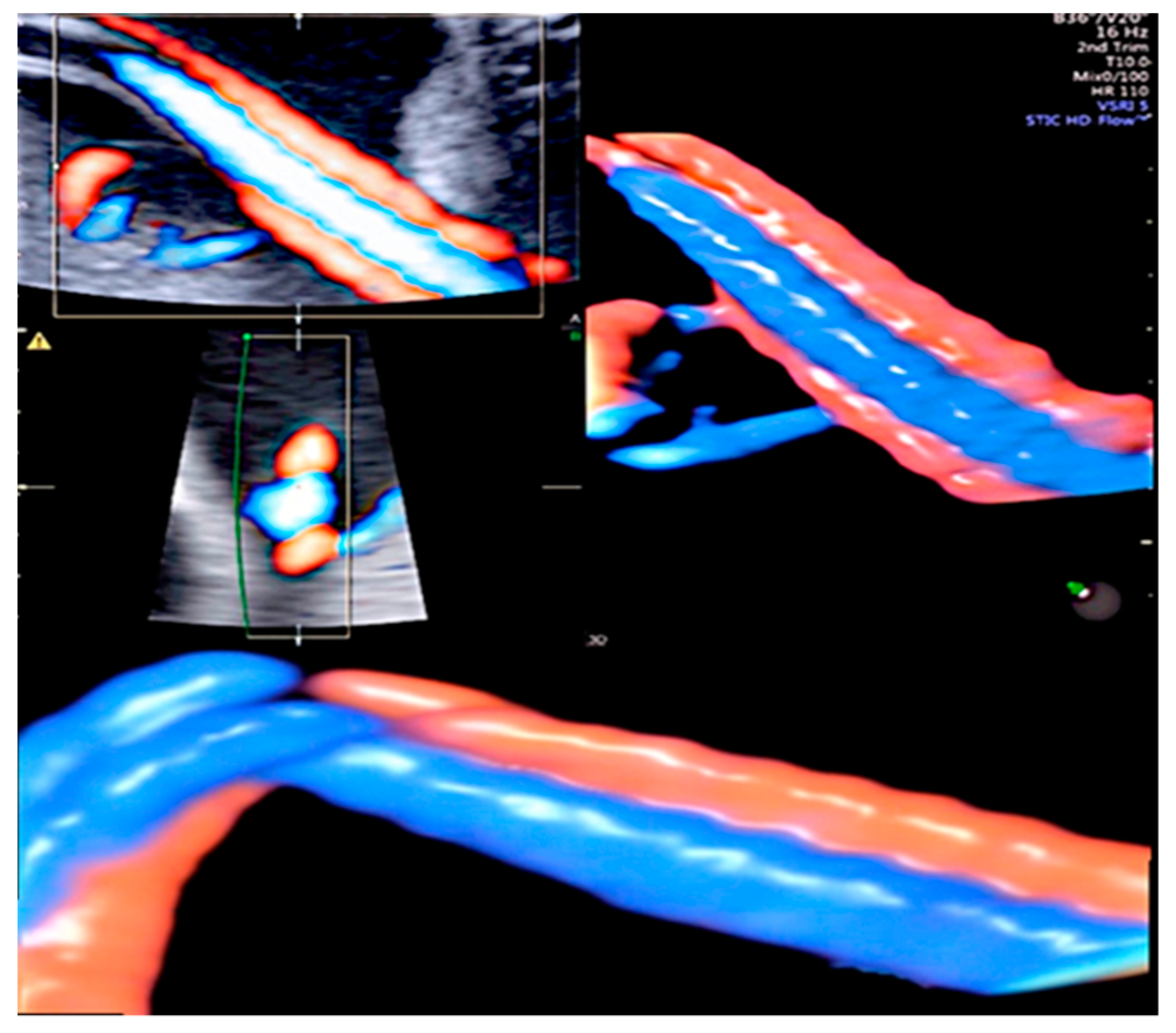
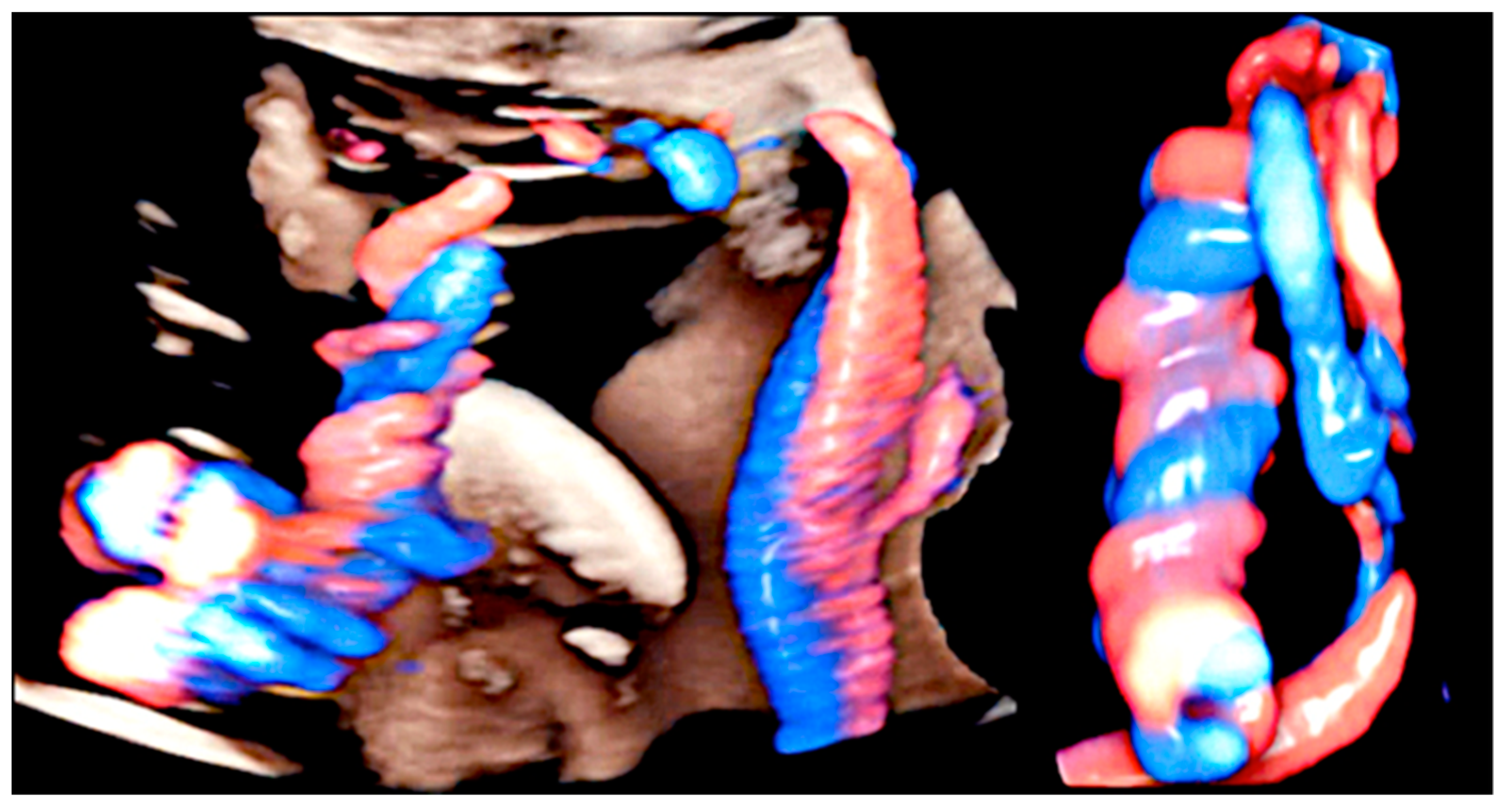
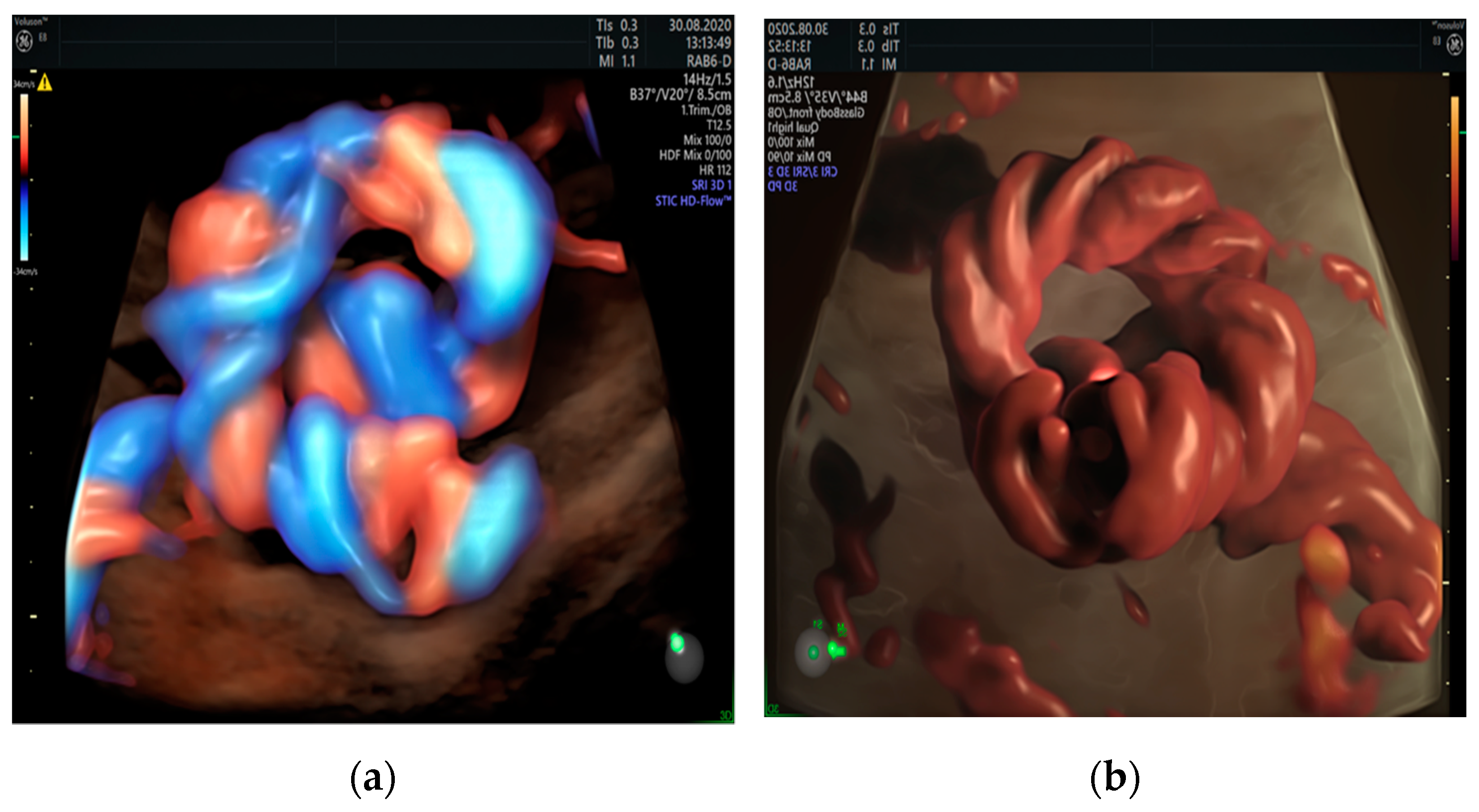
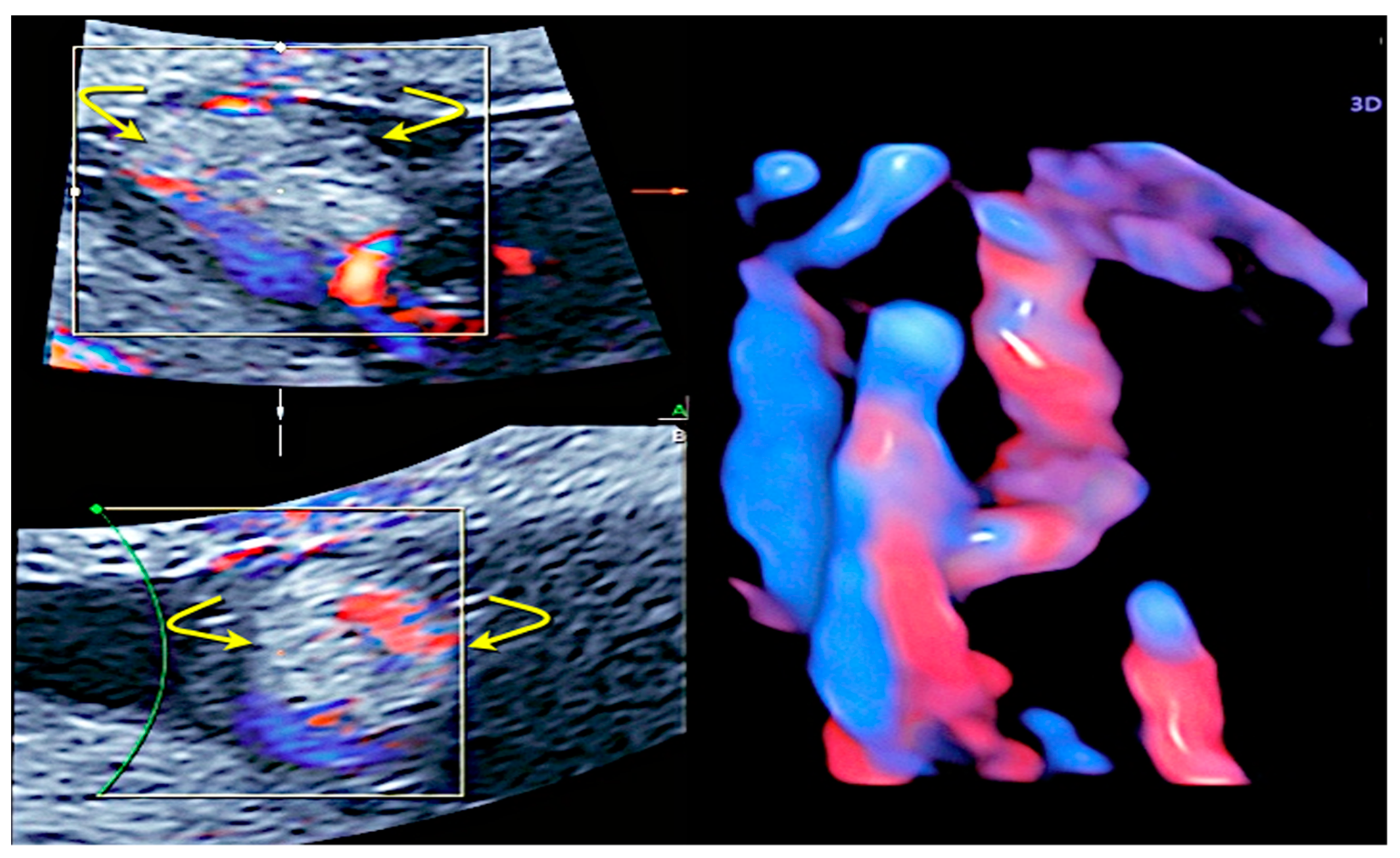
3.1. Cord Coiling
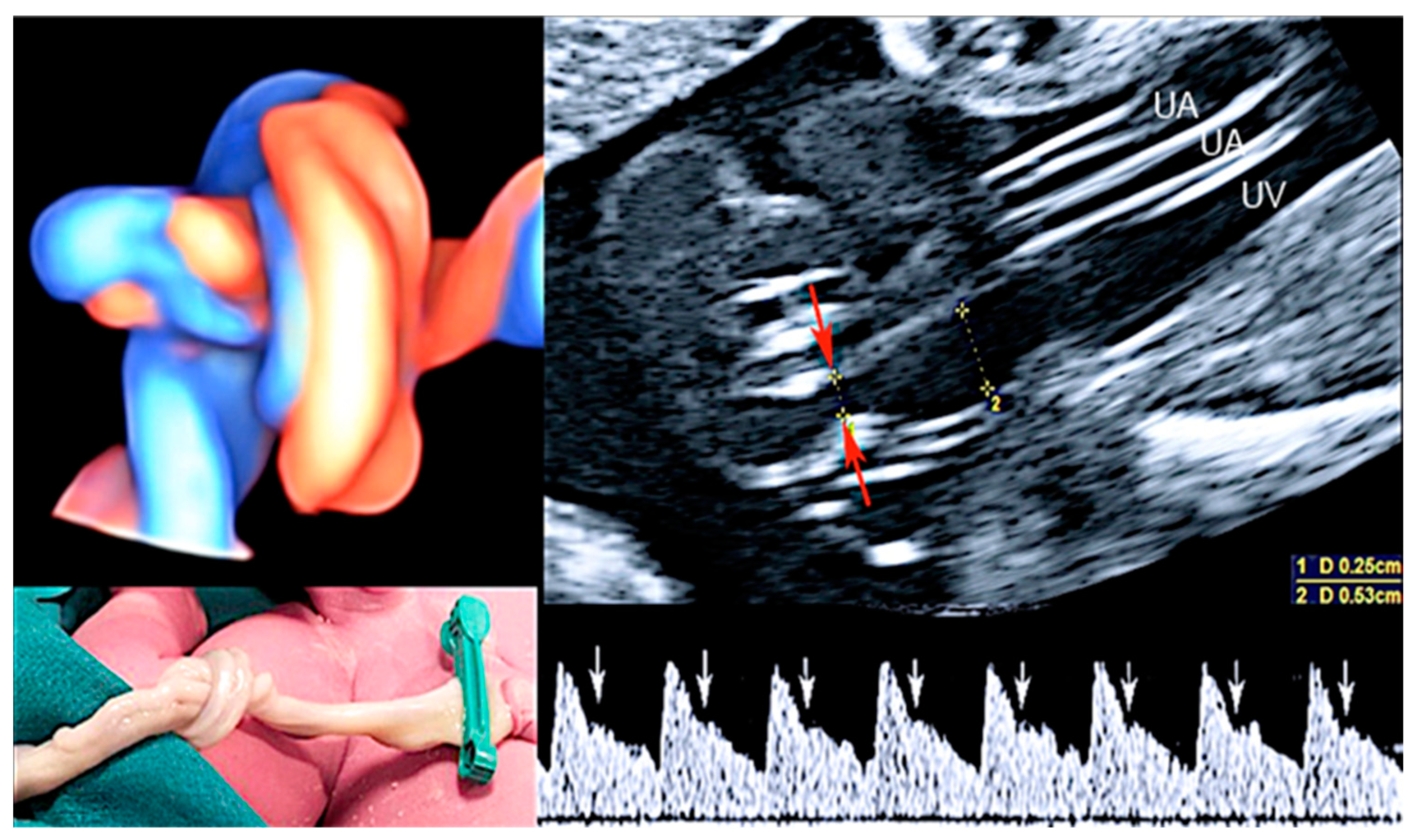
3.2. True Umbilical Cord Knot
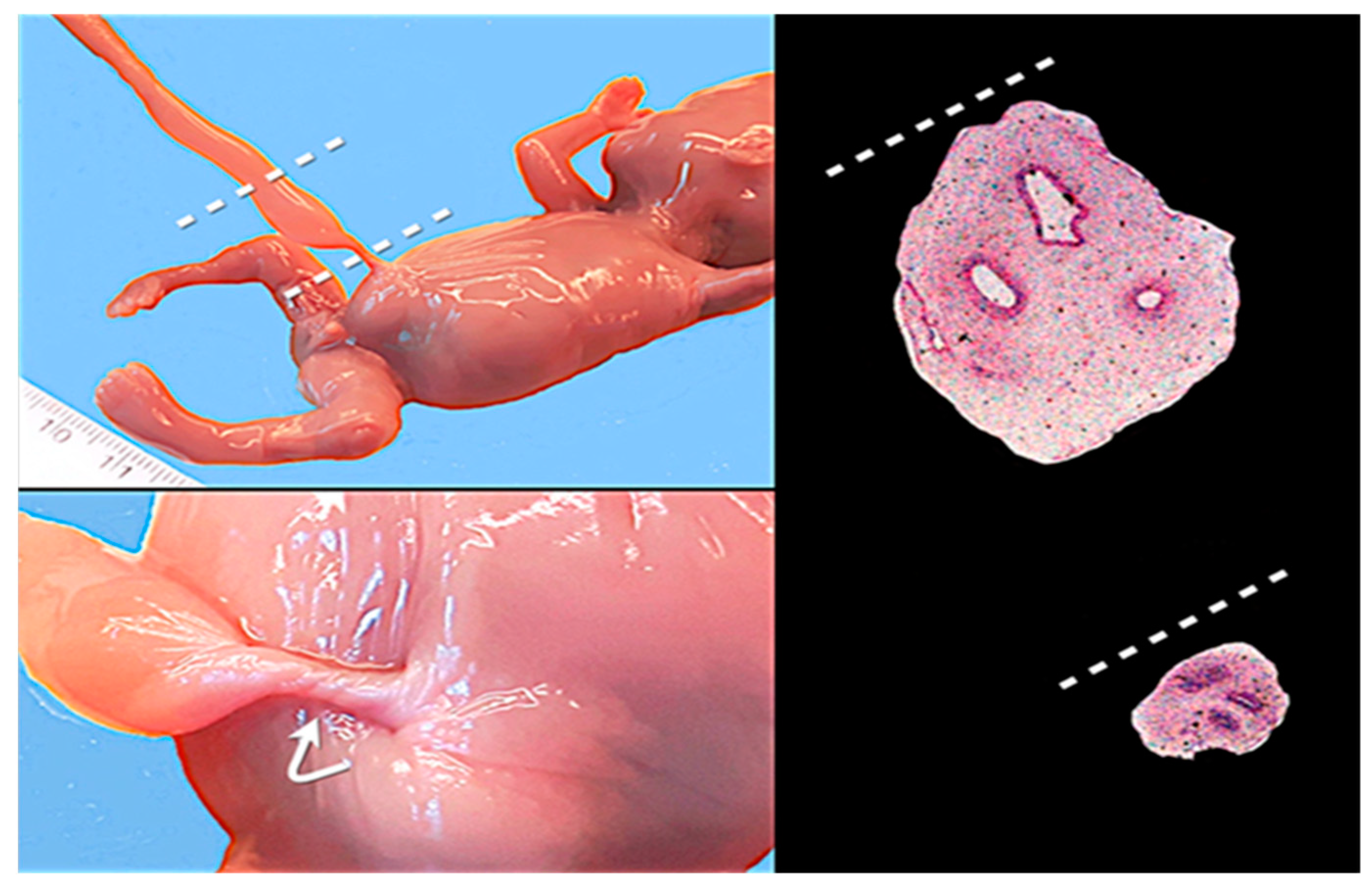
3.3. Umbilical Cord Stricture
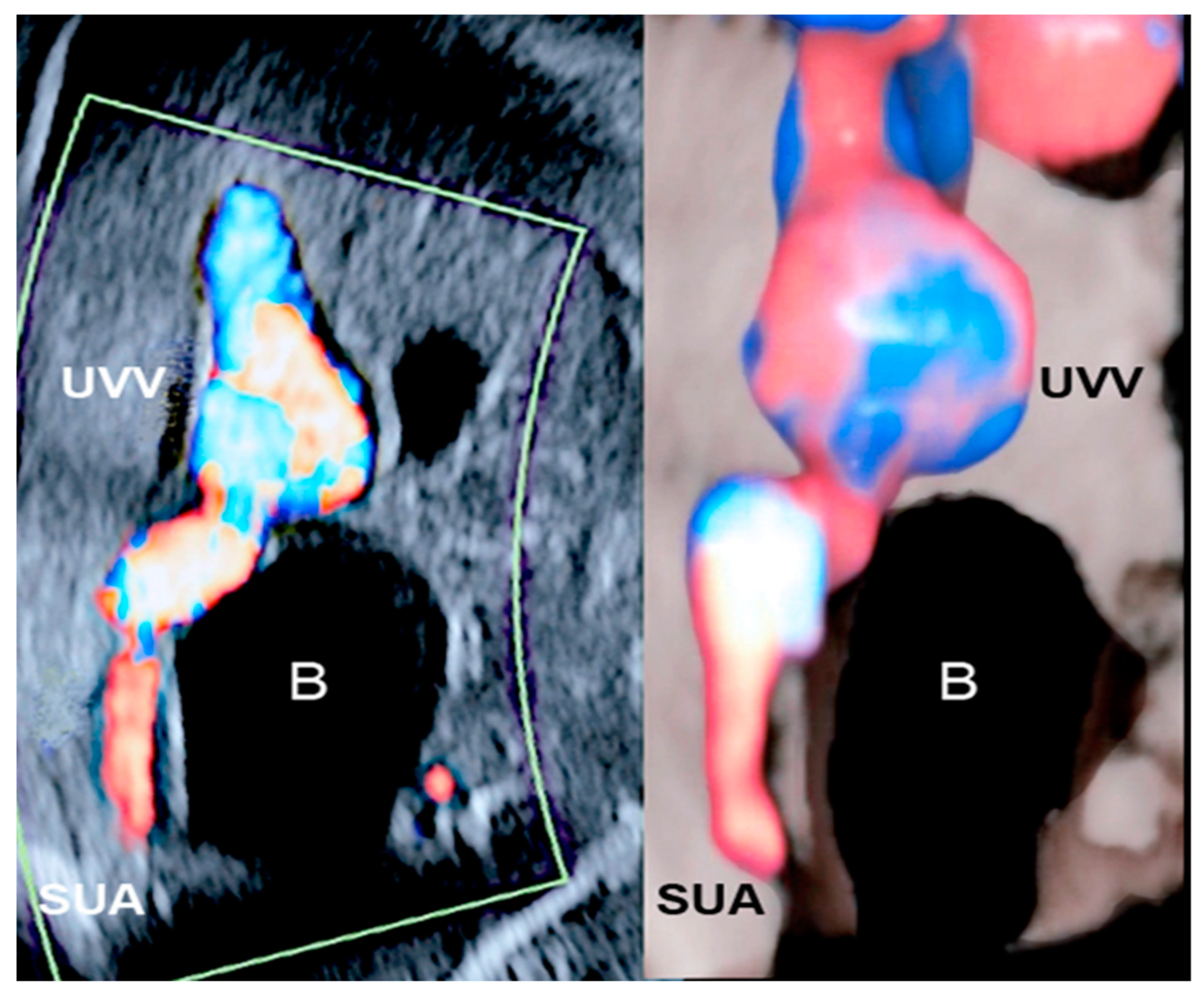
3.4. Single Umbilical Artery
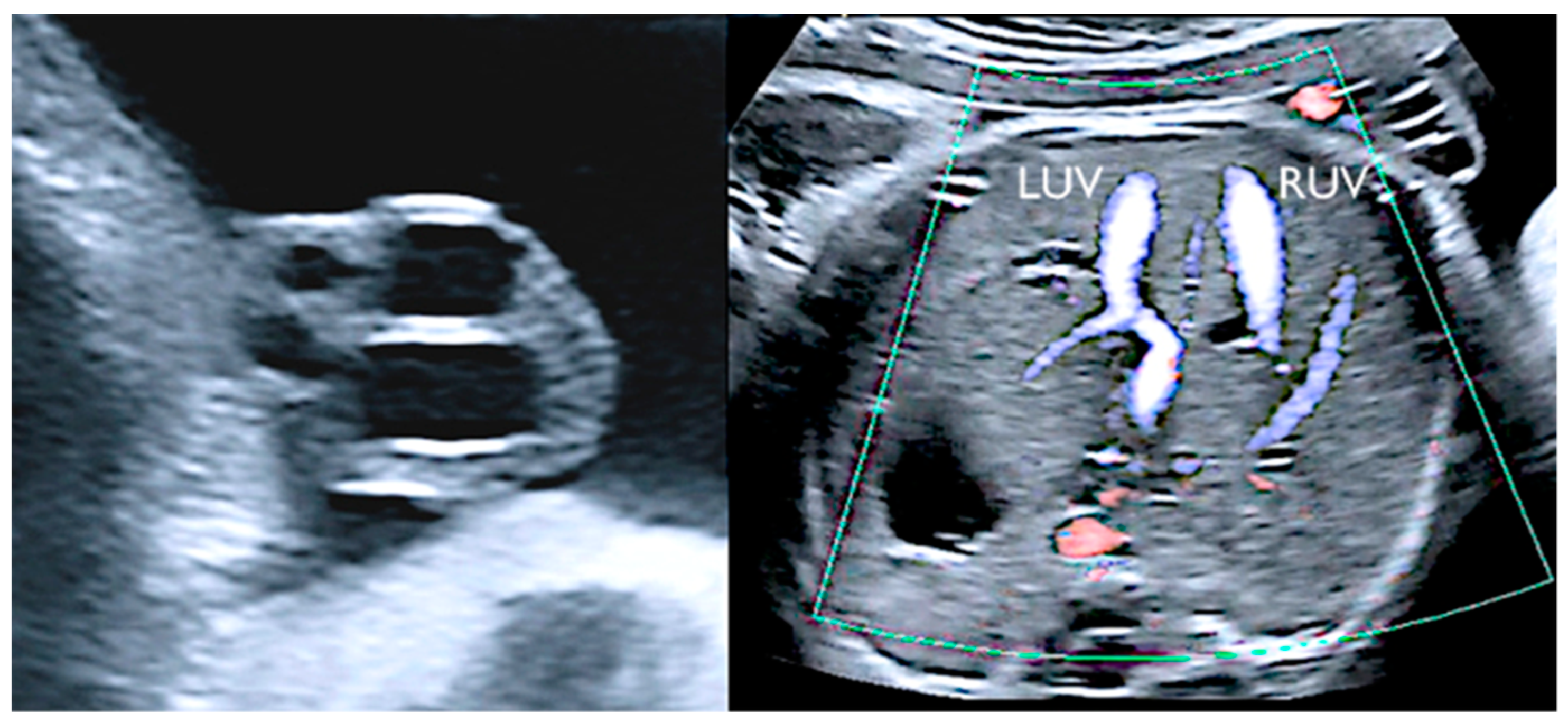
3.5. Supernumerary Vessels
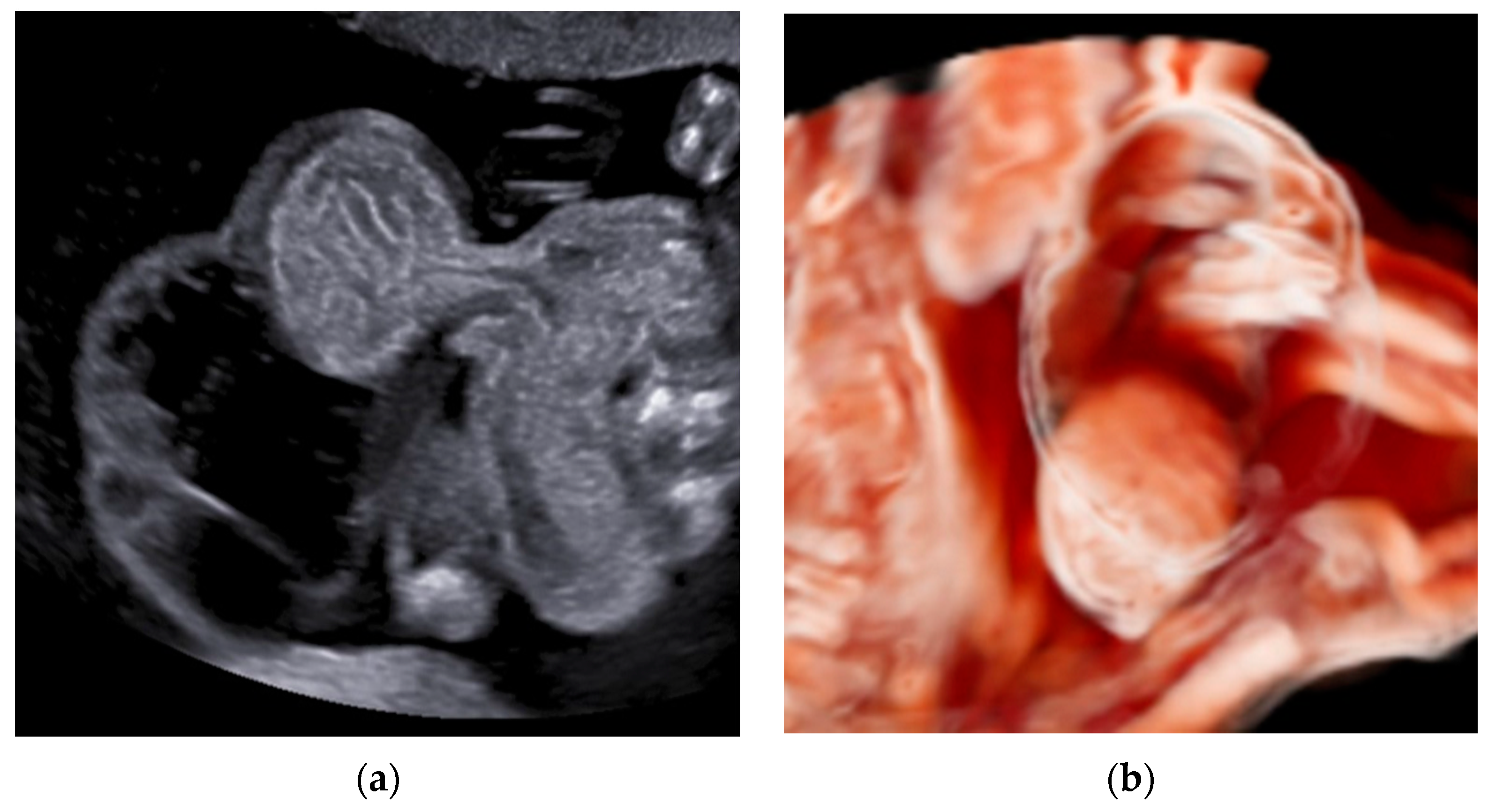
3.6. Umbilical Cord Cysts
3.7. Angiomyxoma/Hemangioma of the Umbilical Cord
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dutman, A.C.; Nikkels, P.G.J. Umbilical Hypercoiling in 2nd- and 3rd-Trimester Intrauterine Fetal Death. Pediatr. Dev. Pathol. 2015, 18, 10–16. [Google Scholar] [CrossRef]
- The Stillbirth Collaborative Research Network Writing Group. Causes of death among stillbirths. JAMA 2011, 306, 2459–2468. [Google Scholar] [CrossRef]
- Stillbirths and Stillbirth Rates. Available online: https://data.unicef.org/topic/child-survival/stillbirths/ (accessed on 1 January 2023).
- Ptacek, I.; Sebire, N.; Man, J.; Brownbill, P.; Heazell, A. Systematic review of placental pathology reported in association with stillbirth. Placenta 2014, 35, 552–562. [Google Scholar] [CrossRef]
- Hayes, D.J.L.; Warland, J.; Parast, M.M.; Bendon, R.W.; Hasegawa, J.; Banks, J.; Clapham, L.; Heazell, A.E.P. Umbilical cord characteristics and their association with adverse pregnancy outcomes: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0239630. [Google Scholar] [CrossRef]
- Redline, R.W. Classification of placental lesions. Am. J. Obstet. Gynecol. 2015, 213, S21–S28. [Google Scholar] [CrossRef]
- Po’, G.; Monari, F.; Zanni, F.; Grandi, G.; Lupi, C.; Facchinetti, F. Stillbirth Emilia-Romagna Audit Group. A regional audit system for stillbirth: A way to better understand the phenomenon. BMC Pregnancy Childbirth 2019, 19, 276. [Google Scholar] [CrossRef]
- Crispi, F.; Miranda, J.; Gratacós, E. Long-term cardiovascular consequences of fetal growth restriction: Biology, clinical implications, and opportunities for prevention of adult disease. Am. J. Obstet. Gynecol. 2018, 218, S869–S879. [Google Scholar] [CrossRef]
- Takahashi, M.; Makino, S.; Oguma, K.; Imai, H.; Takamizu, A.; Koizumi, A.; Yoshida, K. Fetal growth restriction as the initial finding of preeclampsia is a clinical predictor of maternal and neonatal prognoses: A single-center retrospective study. BMC Pregnancy Childbirth 2021, 21, 678. [Google Scholar] [CrossRef]
- Tagliaferri, S.; Travaglino, A.; Raffone, A.; Saccone, G.; Campanino, M.R.; Zara, G.; Ammendola, A.; Pini, N.; Maruotti, G.M.; Magenes, G.; et al. Placental dysfunction in uncomplicated and complicated intrauterine growth restriction by preeclampsia and neonatal outcome. J. Matern. Fetal Neonatal Med. 2022, 35, 8169–8175. [Google Scholar] [CrossRef]
- Conrad, M.S.; Gardner, M.L.; Miguel, C.; Freitas, M.A.; Rood, K.M.; Ma’ayeh, M. Proteomic analysis of the umbilical cord in fetal growth restriction and preeclampsia. PLoS ONE 2022, 17, e0262041. [Google Scholar] [CrossRef]
- Subashini, G.; Anitha, C.; Gopinath, G.; Ramyathangam, K. A Longitudinal Analytical Study on Umbilical Cord Coiling Index as a Predictor of Pregnancy Outcome. Cureus 2023, 15, e35680. [Google Scholar] [CrossRef]
- Chitra, T.; Sushanth, Y.S.; Raghavan, S. Umbilical coiling index as a marker of perinatal outcome: An analytical study. Obstet. Gynecol. Int. 2012, 2012, 213689. [Google Scholar] [CrossRef]
- Kashanian, M.; Akbarian, A.; Kouhpayehzadeh, J. The umbilical coiling index and adverse perinatal outcome. Int. J. Gynaecol. Obstet. 2006, 95, 8e13. [Google Scholar] [CrossRef]
- Ernst, L.M.; Minturn, L.; Huang, M.H.; Curry, E.; Su, E.J. Gross patterns of umbilical cord coiling: Correlations with placental histology and stillbirth. Placenta 2013, 34, 583–588. [Google Scholar] [CrossRef]
- Hasegawa, J. Ultrasound Assessment of the Umbilical Cord. Donald Sch. J. Ultrasound Obstet. Gynecol. 2014, 8, 382–390. [Google Scholar] [CrossRef]
- Mittal, A.; Nanda, S.; Sem, J. Antenatal umbilical coiling index as a predictor of perinatal outcome. Arch. Gynecol. Obstet. 2015, 291, 763–768. [Google Scholar] [CrossRef]
- Strong, T.H., Jr.; Jarles, D.L.; Vega, J.S.; Feldman, D.B. The umbilical coiling index. Am. J. Obstet. Gynecol. 1994, 170 1 Pt 1, 29–32. [Google Scholar] [CrossRef]
- Hammad, I.A.; Blue, N.R.; Allshouse, A.A.; Silver, R.M.; Gibbins, K.J.; Page, J.M.; Goldenberg, R.L.; Reddy, U.M.; Saade, G.R.; Dudley, D.J.; et al. Umbilical Cord Abnormalities and Stillbirth. Obstet. Gynecol. 2020, 135, 644–652. [Google Scholar] [CrossRef]
- Slack, J.C.; Boyd, T.K. Fetal vascular malperfusion due to long and hypercoiled umbilical cords resulting in recurrent second trimester pregnancy loss: A case series and literature review. Pediatr. Dev. Pathol. 2021, 24, 12–18. [Google Scholar] [CrossRef]
- Feist, H.; Hussein, K.; Blöcker, T.; Wohlschlaeger, J. Pathoanatomical lesions in placentas with excessively hypercoiled umbilical cords: Frequent detection of massive perivillous fibrin deposition. Ped Dev. Pathol. 2020, 23, 107–114. [Google Scholar] [CrossRef]
- Ayala, N.K.; Ernst, L.M.; Miller, E.S. Is umbilical coiling genetically determined? J. Perinatol. 2018, 38, 653–657. [Google Scholar] [CrossRef]
- Redline, R.W.; Ravishankar, S. Fetal vascular malperfusion, an update. APMIS J. Path Micro Immun. 2018, 126, 561–569. [Google Scholar] [CrossRef]
- Bamberg, C.; Diemert, A.; Glosemeyer, P.; Tavares De Sousa, M.; Hecker, K. Discordance of umbilical coiling index between recipients and donors in twin-twin transfusion syndrome. Placenta 2019, 76, 19–22. [Google Scholar] [CrossRef]
- Laranjo, M.; Neves, B.M.; Peixinho, C. True double umbilical cord knot. BMJ Case Reports 2022, 15, e251388. [Google Scholar] [CrossRef]
- Räisänen, S.; Georgiadis, L.; Harju, M.; Keski-Nisula, L.; Heinonen, S. True umbilical cord knot and obstetric outcome. Int. J. Gynaecol. Obstet. 2013, 122, 18–21. [Google Scholar] [CrossRef]
- Stabile, G.; Carlucci, S.; De Bonis, L.; Sorrentino, F.; Nappi, L.; Ricci, G. Umbilical Cord Knots: Is the Number Related to Fetal Risk? Medicina 2022, 58, 703. [Google Scholar] [CrossRef]
- Sherer, D.M.; Dalloul, M.; Ward, K.; Nakagawa, J.; Joseph, I.; Grube, S.; Abulafia, O. Coexisting true umbilical cord knot and nuchal cord: Possible cumulative increased risk of adverse perinatal outcome. Ultrasound Obstet. Gynecol. 2017, 50, 404–405. [Google Scholar] [CrossRef]
- Ikechebelu, J.; Eleje, G.; Ofojebe, C. True umbilical cord knot leading to fetal demise. Ann. Med. Health Sci. Res. 2014, 4, S155–S158. [Google Scholar] [CrossRef]
- Moshiri, M.; Zaidi, S.F.; Robinson, T.J.; Bhargava, P.; Siebert, J.R.; Dubinsky, T.J.; Katz, D.S. Comprehensive imaging review of abnormalities of the umbilical cord. Radiographics 2014, 34, 179–196. [Google Scholar] [CrossRef]
- Blichárová, A.; Verbóová, L.; Benetinová, Z.; Mátyás, T.; Bašista, R.; Tancoš, V.; Kollárová, P. Loss of Wharton’s jelly and fibrosis in umbilical cord stricture area: A case report. J. Forensic Leg. Med. 2023, 96, 102512. [Google Scholar] [CrossRef]
- Peng, H.Q.; Levitin-Smith, M.; Rochelson, B.; Kahn, E. Umbilical cord stricture and overcoiling are common causes of fetal demise. Pediatr Dev Pathol. 2006, 9, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Kadivar, M.; Khamseh, M.E.; Malek, M.; Khajavi, A.; Noohi, A.H.; Najafi, L. Histomorphological changes of the placenta and umbilical cord in pregnancies complicated by gestational diabetes mellitus. Placenta 2020, 97, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Tica, O.S.; Tica, A.A.; Cojocaru, D.; Tica, I.; Cojocaru, V.; Tica, V.I. Single umbilical artery: A continuous dilemma and challenge in obstetric management. Clin. Exp. Obst Gynecol. 2021, 48, 1200–1205. [Google Scholar]
- Friebe-Hoffmann, U.; Hiltmann, A.; Friedl, T.W.P.; Lato, K.; Hammer, R.; Janni, W.; Kozlowski, P. Prenatally Diagnosed Single Umbilical Artery (SUA)—Retrospective Analysis of 1169 Fetuses. Ultraschall Der Medizin. 2019, 40, 221–229. [Google Scholar] [CrossRef]
- Martínez-Frías, M.L.; Bermejo, E.; Rodríguez-Pinilla, E.; Prieto, D.; ECEMC Working Group. Does single umbilical artery (SUA) predict any type of congenital defect? Clinical-epidemiological analysis of a large consecutive series of malformed infants. Am. J. Med. Genet. Part. A 2008, 146, 15–25. [Google Scholar] [CrossRef]
- Chang, K.T.E.; Aw, S.J. Single Umbilical Artery, Supernumerary Vessels, Segmental Thinning of the Umbilical Cord Vessels and Vascular Calcifications in Umbilical Vessels; Khong, T., Mooney, E., Nikkels, P., Morgan, T., Gordijn, S., Eds.; Pathology of the Placenta; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Dagklis, T.; Defigueiredo, D.; Staboulidou, I.; Casagrandi, D.; Nicolaides, K.H. Isolated single umbilical artery and fetal karyotype. Ultrasound Obstet. Gynecol. 2010, 36, 291–295. [Google Scholar] [CrossRef]
- Lubusky, M.; Dhaifalah, I.; Prochazka, M.; Hyjanek, J.; Mickova, I.; Vomackova, K.; Santavy, J. Single umbilical artery and its siding in the second trimester of pregnancy: Relation to chromosomal defects. Prenat. Diagn. 2007, 27, 327–331. [Google Scholar] [CrossRef]
- Lei, T.; Xie, H.N.; Feng, J.l. Prenatal diagnosis of four-vessel umbilical cord with supernumerary vein varix: A case report and literature review. J. Obstet. Gynaecol. Res. 2017, 43, 1200–1204. [Google Scholar] [CrossRef]
- Du, X.; Yuan, Q.; Li, Z.; Li, Y. Three umbilical arteries resulting in a four-vessel umbilical cord in a stillbirth. Int. J. Clin. Exp. Med. 2015, 8, 4682–4685. [Google Scholar]
- Ruiz Campo, L.; Savirón Cornudella, R.; Gámez Alderete, F.; Martínez-Payo, C.; Pérez Pérez, P.; Garrido Fernández, P.; Lerma Puertas, D. Prenatal diagnosis of umbilical cord cyst: Clinical significance and prognosis. Taiwan. J. Obstet. Gynecol. 2017, 56, 622–627. [Google Scholar] [CrossRef]
- Zangen, R.; Boldes, R.; Yaffe, H.; Schwed, P.; Weiner, Z. Umbilical cord cysts in the second and third trimesters: Significance and prenatal approach. Ultrasound Obstet. Gynecol. 2010, 36, 296–301. [Google Scholar] [CrossRef]
- Umeda, S.; Usui, N.; Kanagawa, T.; Yamamichi, T.; Nara, K.; Ueno, T.; Owari, M.; Uehara, S.; Oue, T.; Kimura, T.; et al. Prenatal and Postnatal Clinical Course of an Urachus Identified as an Allantoic Cyst in the Umbilical Cord. Eur. J. Pediatr. Surg. 2016, 26, 200–202. [Google Scholar] [CrossRef]
- Chen, H.; Jia, M.; Yang, S.; Zou, J.; Xiao, X. Umbilical cord cysts: Classification, diagnosis, prognosis, and pregnancy recommendations. Int. J. Gynaecol. Obstet. 2023. (Online ahead of print). [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Heerema-McKenney, A.; Kollikonda, S.; Karnati, S. Changing course of an umbilical cord mass—Chasing the diagnosis of agiomyxoma. Ped Dev. Pathol. 2022, 25, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Deus, A.; Pérez-Muñuzuri, A.; Urisarri, A.; Bautista-Casasnovas, A.; Couce, M.-L. Umbilical cord and visceral hemangiomas diagnosed in the neonatal period. Medicine. 2016, 95, e5196. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Fukumura, Y.; Saito, T.; Arakawa, A.; Okabe, H.; Takeda, S.; Yao, T. A giant cord hemangioma with extramedullary hematopoiesis and elevated maternal serum human chorionic gonadotropin: A case report and review of the literature. Diagn. Pathol. 2015, 10, 154. [Google Scholar] [CrossRef]
- Sathiyathasan, S.; Jeyanthan, K.; Hamid, R. Umbilical hemangioma: A case report. Arch. Gynecol. Obstet. 2011, 283 (Suppl. 1), 15–17. [Google Scholar] [CrossRef]
- Ben Thayer, M.; Helal, I.; Khanchel, F.; Mbarki, C.; Bettaieb, H.; Ben Brahim, E.; Jouini, R.; Chadli Debbiche, A. Hemangioma of the umbilical cord: A case report on a rare entity. Clin. Case Rep. 2022, 10, e6441. [Google Scholar] [CrossRef]
- Daniel-Spiegel, E.; Weiner, E.; Gimburg, G. The association of umbilical cord hemangioma with fetal vascular markers. Prenat. Diagn. 2005, 25, 300–303. [Google Scholar] [CrossRef]
- Lisovaja, I.; Franckevica, I.; Vedmedovska, N. Large angiomyxoma of the umbilical cord-uncomplicated rupture of tumor membranes at 32 weeks of gestation. Diagnostics 2022, 12, 1339. [Google Scholar] [CrossRef]
- ISSVA. ISSVA Classification of Vascular Anomalies 2018 International Society for the Study of Vascular Anomalies. Available online: https://www.Issva.Org/Classification (accessed on 1 January 2023).
- Hafeez, F.; Krakowski, A.C.; Lian, C.G.; Nazarian, R.M.; Maleszewski, J.J. Sporadic superficial angiomyxomas demonstrate loss of PRKAR1A expression. Histopathology 2022, 80, 1001–1003. [Google Scholar] [CrossRef] [PubMed]
- Scalise, C.; Cordasco, F.; Sacco, M.A.; Ricci, P.; Aquila, I. The Importance of Post-Mortem Investigations in Stillbirths: Case Studies and a Review of the Literature. Int. J. Environ. Res. Public. Health 2022, 19, 8817. [Google Scholar] [CrossRef] [PubMed]













Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonni, G.; Lituania, M.; Cecchi, A.; Carboni, E.; Resta, S.; Bonasoni, M.P.; Ruano, R. Umbilical Cord Diseases Affecting Obstetric and Perinatal Outcomes. Healthcare 2023, 11, 2634. https://doi.org/10.3390/healthcare11192634
Tonni G, Lituania M, Cecchi A, Carboni E, Resta S, Bonasoni MP, Ruano R. Umbilical Cord Diseases Affecting Obstetric and Perinatal Outcomes. Healthcare. 2023; 11(19):2634. https://doi.org/10.3390/healthcare11192634
Chicago/Turabian StyleTonni, Gabriele, Mario Lituania, Alessandro Cecchi, Elisa Carboni, Serena Resta, Maria Paola Bonasoni, and Rodrigo Ruano. 2023. "Umbilical Cord Diseases Affecting Obstetric and Perinatal Outcomes" Healthcare 11, no. 19: 2634. https://doi.org/10.3390/healthcare11192634