
Interactions between Metabolic Syndrome, MASLD, and Arterial Stiffening: A Single-Center Cross-Sectional Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Anthropometric Data
2.3. Metabolic Syndrome Criteria, MeTS, and MASLD Diagnosis
2.4. Laboratory Measurements and Simple Score Calculation
2.5. Vibration-Controlled Transient Elastography
2.6. Arterial Stiffness Measurement
2.7. Carotid Intima–Media Thickness
2.8. Measurement Methodology
2.9. Statistical Analysis
2.10. Two-Step Cluster Analysis
3. Results
3.1. Study Population and Gender Differences
3.2. Comparison between Patients with and without MetS
3.3. Cluster Analysis
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
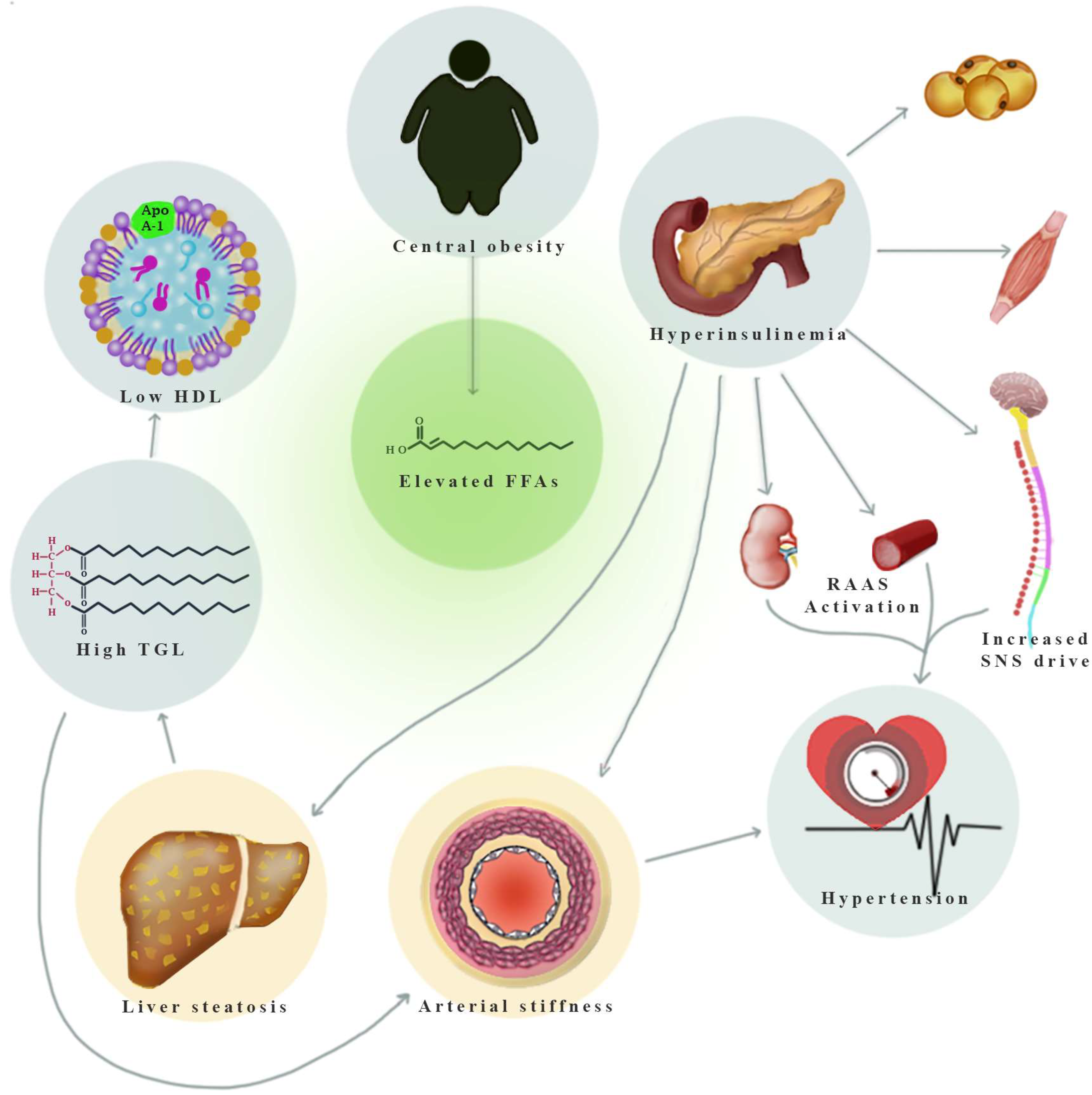
Appendix A. Overview of Mechanisms Linking MetS Components to Hepatic Steatosis and Arterial Stiffness
Appendix A.1. Central Obesity
Appendix A.2. Hypertriglyceridemia
Appendix A.3. Low HDL-Cholesterol
Appendix A.4. Impaired Fasting Glucose/T2DM
Appendix A.5. Hypertension
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multi-Society Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. Hepatology 2023, 101133. [Google Scholar] [CrossRef]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the Epidemic of Nonalcoholic Fatty Liver Disease Demonstrates an Exponential Increase in Burden of Disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Hardy, T.; Wonders, K.; Younes, R.; Aithal, G.P.; Aller, R.; Allison, M.; Bedossa, P.; Betsou, F.; Boursier, J.; Brosnan, M.J.; et al. The European NAFLD Registry: A Real-World Longitudinal Cohort Study of Nonalcoholic Fatty Liver Disease. Contemp. Clin. Trials 2020, 98, 106175. [Google Scholar] [CrossRef] [PubMed]
- Maurice, J.; Manousou, P. Non-Alcoholic Fatty Liver Disease. Clin. Med. 2018, 18, 245–250. [Google Scholar] [CrossRef]
- European Association for the Study of The Liver; European Association for the Study of Diabetes. EASL–EASD–EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Yip, G.W.-K.; Lo, A.O.-S.; Limquiaco, J.; Chu, W.C.-W.; Chim, A.M.-L.; Yu, C.-M.; Yu, J.; Chan, F.K.-L.; et al. Coronary Artery Disease and Cardiovascular Outcomes in Patients with Non-Alcoholic Fatty Liver Disease. Gut 2011, 60, 1721–1727. [Google Scholar] [CrossRef]
- Villela-Nogueira, C.; Leite, N.; Cardoso, C.; Salles, G. NAFLD and Increased Aortic Stiffness: Parallel or Common Physiopathological Mechanisms? Int. J. Mol. Sci. 2016, 17, 460. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Pereira, T.; Correia, C.; Cardoso, J. Novel Methods for Pulse Wave Velocity Measurement. J. Med. Biol. Eng. 2015, 35, 555–565. [Google Scholar] [CrossRef]
- Boutouyrie, P.; Revera, M.; Parati, G. Obtaining Arterial Stiffness Indices from Simple Arm Cuff Measurements: The Holy Grail? J. Hypertens. 2009, 27, 2159–2161. [Google Scholar] [CrossRef]
- Naqvi, T.Z.; Lee, M.-S. Carotid Intima-Media Thickness and Plaque in Cardiovascular Risk Assessment. JACC Cardiovasc. Imaging 2014, 7, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Use of Carotid Ultrasound to Identify Subclinical Vascular Disease and Evaluate Cardiovascular Disease Risk: A Consensus Statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis—2021 Update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Orlic, L.; Franjic, N.; Hauser, G.; Stimac, D.; Milic, S. Transient Elastography (FibroScan®) with Controlled Attenuation Parameter in the Assessment of Liver Steatosis and Fibrosis in Patients with Nonalcoholic Fatty Liver Disease—Where Do We Stand? World J. Gastroenterol. 2016, 22, 7236. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Foucquier, J.; Younossi, Z.M.; Harrison, S.A.; Newsome, P.N.; Chan, W.-K.; Yilmaz, Y.; De Ledinghen, V.; Costentin, C.; Zheng, M.-H.; et al. Enhanced Diagnosis of Advanced Fibrosis and Cirrhosis in Individuals with NAFLD Using FibroScan-Based Agile Scores. J. Hepatol. 2023, 78, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Defining Adult Obesity. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html#:~:text=If%20your%20BMI%20is%2018.5,falls%20within%20the%20obesity%20range (accessed on 3 September 2023).
- McPherson, S.; Stewart, S.F.; Henderson, E.; Burt, A.D.; Day, C.P. Simple Non-Invasive Fibrosis Scoring Systems Can Reliably Exclude Advanced Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef]
- Wong, S.; Huynh, D.; Zhang, F.; Nguyen, N.Q. Use of Aspartate Aminotransferase to Platelet Ratio to Reduce the Need for FibroScan in the Evaluation of Liver Fibrosis. World J. Hepatol. 2017, 9, 791. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic Steatosis Index: A Simple Screening Tool Reflecting Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Rajzer, M.W.; Wojciechowska, W.; Klocek, M.; Palka, I.; Brzozowska-Kiszka, M.; Kawecka-Jaszcz, K. Comparison of Aortic Pulse Wave Velocity Measured by Three Techniques: Complior, SphygmoCor and Arteriograph. J. Hypertens. 2008, 26, 2001–2007. [Google Scholar] [CrossRef]
- Mattace-Raso, F.U.; Hofman, A.; Verwoert, G.C.; Wittemana, J.C.; Wilkinson, I.; Cockcroft, J.; McEniery, C.; Yasmin; Laurent, S.; Boutouyrie, P.; et al. The Reference Values for Arterial Stiffness’ Collaboration. Determinants of Pulse Wave Velocity in Healthy People and in the Presence of Cardiovascular Risk Factors: ‘Establishing Normal and Reference Values’. Eur. Heart J. 2010, 31, 2338–2350. [Google Scholar] [CrossRef]
- Randrianarisoa, E.; Rietig, R.; Jacob, S.; Blumenstock, G.; Haering, H.-U.; Rittig, K.; Balletshofer, B. Normal Values for Intima-Media Thickness of the Common Carotid Artery—An Update Following a Novel Risk Factor Profiling. Vasa 2015, 44, 444–450. [Google Scholar] [CrossRef]
- Solomon, A.; Cipăian, C.R.; Negrea, M.O.; Boicean, A.; Mihaila, R.; Beca, C.; Popa, M.L.; Grama, S.M.; Teodoru, M.; Neamtu, B. Hepatic Involvement across the Metabolic Syndrome Spectrum: Non-Invasive Assessment and Risk Prediction Using Machine Learning. J. Clin. Med. 2023, 12, 5657. [Google Scholar] [CrossRef] [PubMed]
- Stehouwer, C.D.A.; Henry, R.M.A.; Ferreira, I. Arterial Stiffness in Diabetes and the Metabolic Syndrome: A Pathway to Cardiovascular Disease. Diabetologia 2008, 51, 527–539. [Google Scholar] [CrossRef]
- Aydin, M.; Bulur, S.; Alemdar, R.; Yalçin, S.; Türker, Y.; Basar, C.; Aslantas, Y.; Yazgan, Ö.; Albayrak, S.; Özhan, H.; et al. The Impact of Metabolic Syndrome on Carotid Intima Media Thickness. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2295–2301. [Google Scholar] [CrossRef] [PubMed]
- Al Rifai, M.; Silverman, M.G.; Nasir, K.; Budoff, M.J.; Blankstein, R.; Szklo, M.; Katz, R.; Blumenthal, R.S.; Blaha, M.J. The Association of Nonalcoholic Fatty Liver Disease, Obesity, and Metabolic Syndrome, with Systemic Inflammation and Subclinical Atherosclerosis: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2015, 239, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, K.; Uygun, A.; Guler, A.K.; Demirci, H.; Ozdemir, C.; Cakir, M.; Sakin, Y.S.; Turker, T.; Sari, S.; Demirbas, S.; et al. Nonalcoholic Fatty Liver Disease Is an Independent Risk Factor for Atherosclerosis in Young Adult Men. Atherosclerosis 2015, 240, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality With Arterial Stiffness. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Stahl, E.P.; Dhindsa, D.S.; Lee, S.K.; Sandesara, P.B.; Chalasani, N.P.; Sperling, L.S. Nonalcoholic Fatty Liver Disease and the Heart. J. Am. Coll. Cardiol. 2019, 73, 948–963. [Google Scholar] [CrossRef]
- Cai, J.; Zhang, X.-J.; Ji, Y.-X.; Zhang, P.; She, Z.-G.; Li, H. Nonalcoholic Fatty Liver Disease Pandemic Fuels the Upsurge in Cardiovascular Diseases. Circ. Res. 2020, 126, 679–704. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-Alcoholic Fatty Liver Disease and Risk of Incident Cardiovascular Disease: A Meta-Analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef]
- Li, N.; Zhang, G.-W.; Zhang, J.-R.; Jin, D.; Li, Y.; Liu, T.; Wang, R.-T. Non-Alcoholic Fatty Liver Disease Is Associated with Progression of Arterial Stiffness. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, T.; Schlinzig, T.; Krohn, K.; Meinertz, T.; Münzel, T. Endothelial Dysfunction, Oxidative Stress, and Risk of Cardiovascular Events in Patients with Coronary Artery Disease. Circulation 2001, 104, 2673–2678. [Google Scholar] [CrossRef]
- Jesmin, S.; Sakuma, I.; Salah-Eldin, A.; Nonomura, K.; Hattori, Y.; Kitabatake, A. Diminished Penile Expression of Vascular Endothelial Growth Factor and Its Receptors at the Insulin-Resistant Stage of a Type II Diabetic Rat Model: A Possible Cause for Erectile Dysfunction in Diabetes. J. Mol. Endocrinol. 2003, 31, 401–418. [Google Scholar] [CrossRef]
- Matsubayashi, Y.; Fujihara, K.; Yamada-Harada, M.; Mitsuma, Y.; Sato, T.; Yaguchi, Y.; Osawa, T.; Yamamoto, M.; Kitazawa, M.; Yamada, T.; et al. Impact of Metabolic Syndrome and Metabolic Dysfunction-Associated Fatty Liver Disease on Cardiovascular Risk by the Presence or Absence of Type 2 Diabetes and According to Sex. Cardiovasc. Diabetol. 2022, 21, 90. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, C.; Deng, S.; Yuan, T.; Zhu, X.; Deng, Y.; Qin, Y.; Wang, Y.; Yang, P. Transition Patterns of Metabolic Dysfunction-Associated Fatty Liver Disease Status in Relation to Arterial Stiffness Progression: A Health Check-up Cohort Study. Sci. Rep. 2023, 13, 9690. [Google Scholar] [CrossRef]
- Echeverri, D.; Pizano, A.; Cabrales, J.; Moreno, K. Validation of Central and Peripheral Non-Invasive Hemodynamic Variables Using an Oscillometric Method. High. Blood Press. Cardiovasc. Prev. 2018, 25, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Vicente, W.R.P.; Rodrigues, S.; Cepeda, F.X.; Jordão, C.P.; Costa-Hong, V.; Dutra-Marques, A.C.B.; Carvalho, J.C.; Alves, M.J.N.N.; Bortolotto, L.A.; Trombetta, I.C. Arterial Stiffness and Its Association with Clustering of Metabolic Syndrome Risk Factors. Diabetol. Metab. Syndr. 2017, 9, 87. [Google Scholar] [CrossRef] [PubMed]
- Tsaban, G.; Yaskolka Meir, A.; Zelicha, H.; Rinott, E.; Kaplan, A.; Shalev, A.; Katz, A.; Brikner, D.; Blüher, M.; Ceglarek, U.; et al. Diet-Induced Fasting Ghrelin Elevation Reflects the Recovery of Insulin Sensitivity and Visceral Adiposity Regression. J. Clin. Endocrinol. Metab. 2022, 107, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Kump, D.S.; Booth, F.W. Alterations in Insulin Receptor Signalling in the Rat Epitrochlearis Muscle upon Cessation of Voluntary Exercise. J. Physiol. 2005, 562, 829–838. [Google Scholar] [CrossRef]
- Lombardo, M.; Guseva, E.; Perrone, M.A.; Müller, A.; Rizzo, G.; Storz, M.A. Changes in Eating Habits and Physical Activity after COVID-19 Pandemic Lockdowns in Italy. Nutrients 2021, 13, 4522. [Google Scholar] [CrossRef]
- Negrea, M.O.; Neamtu, B.; Dobrotă, I.; Sofariu, C.R.; Crisan, R.M.; Ciprian, B.I.; Domnariu, C.D.; Teodoru, M. Causative Mechanisms of Childhood and Adolescent Obesity Leading to Adult Cardiometabolic Disease: A Literature Review. Appl. Sci. 2021, 11, 11565. [Google Scholar] [CrossRef]
- Castro, A.V.B.; Kolka, C.M.; Kim, S.P.; Bergman, R.N. Obesity, Insulin Resistance and Comorbidities? Mechanisms of Association. Arq. Bras. Endocrinol. Metabol. 2014, 58, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Rampanelli, E.; Ochodnicky, P.; Vissers, J.P.; Butter, L.M.; Claessen, N.; Calcagni, A.; Kors, L.; Gethings, L.A.; Bakker, S.J.; de Borst, M.H.; et al. Excessive Dietary Lipid Intake Provokes an Acquired Form of Lysosomal Lipid Storage Disease in the Kidney. J. Pathol. 2018, 246, 470–484. [Google Scholar] [CrossRef] [PubMed]
- Ye, J. Mechanisms of Insulin Resistance in Obesity. Front. Med. 2013, 7, 14–24. [Google Scholar] [CrossRef]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef] [PubMed]
- Björntorp, P. “Portal” Adipose Tissue as a Generator of Risk Factors for Cardiovascular Disease and Diabetes. Arteriosclerosis 1990, 10, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Virtue, S.; Vidal-Puig, A. Adipose Tissue Expandability, Lipotoxicity and the Metabolic Syndrome—An Allostatic Perspective. Biochim. Biophys. Acta (BBA)—Mol. Cell Biol. Lipids 2010, 1801, 338–349. [Google Scholar] [CrossRef]
- Rider, O.J.; Banerjee, R.; Rayner, J.J.; Shah, R.; Murthy, V.L.; Robson, M.D.; Neubauer, S. Investigating a Liver Fat. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 198–203. [Google Scholar] [CrossRef]
- Steinberg, H.O.; Paradisi, G.; Hook, G.; Crowder, K.; Cronin, J.; Baron, A.D. Free Fatty Acid Elevation Impairs Insulin-Mediated Vasodilation and Nitric Oxide Production. Diabetes 2000, 49, 1231–1238. [Google Scholar] [CrossRef]
- Harrison, D.G.; Widder, J.; Grumbach, I.; Chen, W.; Weber, M.; Searles, C. Endothelial Mechanotransduction, Nitric Oxide and Vascular Inflammation. J. Intern. Med. 2006, 259, 351–363. [Google Scholar] [CrossRef]
- Hamdy, O. The Role of Adipose Tissue as an Endocrine Gland. Curr. Diabetes Rep. 2005, 5, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Yaskolka Meir, A.; Tene, L.; Cohen, N.; Shelef, I.; Schwarzfuchs, D.; Gepner, Y.; Zelicha, H.; Rein, M.; Bril, N.; Serfaty, D.; et al. Intrahepatic Fat, Abdominal Adipose Tissues, and Metabolic State: Magnetic Resonance Imaging Study. Diabetes Metab. Res. Rev. 2017, 33, e2888. [Google Scholar] [CrossRef] [PubMed]
- Pedro-Botet, J.; Ascaso, J.F.; Barrios, V.; De la Sierra, A.; Escalada, J.; Millán, J.; Mostaza, J.M.; Pérez-Martínez, P.; Pintó, X.; Salas-Salvadó, J.; et al. COSMIC Project: Consensus on the Objectives of the Metabolic Syndrome in Clinic. Diabetes Metab. Syndr. Obes. 2018, 11, 683–697. [Google Scholar] [CrossRef]
- Murakami, T.; Michelagnoli, S.; Longhi, R.; Gianfranceschi, G.; Pazzucconi, F.; Calabresi, L.; Sirtori, C.R.; Franceschini, G. Triglycerides Are Major Determinants of Cholesterol Esterification/Transfer and HDL Remodeling in Human Plasma. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 1819–1828. [Google Scholar] [CrossRef]
- Kashyap, S.R.; Osme, A.; Ilchenko, S.; Golizeh, M.; Lee, K.; Wang, S.; Bena, J.; Previs, S.F.; Smith, J.D.; Kasumov, T. Glycation Reduces the Stability of ApoAI and Increases HDL Dysfunction in Diet-Controlled Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2018, 103, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Heinecke, J.W. Quantifying HDL Proteins by Mass Spectrometry: How Many Proteins Are There and What Are Their Functions? Expert Rev. Proteom. 2018, 15, 31–40. [Google Scholar] [CrossRef]
- Cohen, D.; Fisher, E. Lipoprotein Metabolism, Dyslipidemia, and Nonalcoholic Fatty Liver Disease. Semin. Liver Dis. 2013, 33, 380–388. [Google Scholar] [CrossRef]
- Marušić, M.; Paić, M.; Knobloch, M.; Liberati Pršo, A.-M. NAFLD, Insulin Resistance, and Diabetes Mellitus Type 2. Can. J. Gastroenterol. Hepatol. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Safar, M.E.; Asmar, R.; Benetos, A.; Blacher, J.; Boutouyrie, P.; Lacolley, P.; Laurent, S.; London, G.; Pannier, B.; Protogerou, A.; et al. Interaction Between Hypertension and Arterial Stiffness. Hypertension 2018, 72, 796–805. [Google Scholar] [CrossRef]
- Rizzoni, D.; Porteri, E.; Guelfi, D.; Muiesan, M.L.; Valentini, U.; Cimino, A.; Girelli, A.; Rodella, L.; Bianchi, R.; Sleiman, I.; et al. Structural Alterations in Subcutaneous Small Arteries of Normotensive and Hypertensive Patients with Non–Insulin-Dependent Diabetes Mellitus. Circulation 2001, 103, 1238–1244. [Google Scholar] [CrossRef]
- Nickenig, G.; Röling, J.; Strehlow, K.; Schnabel, P.; Böhm, M. Insulin Induces Upregulation of Vascular AT 1 Receptor Gene Expression by Posttranscriptional Mechanisms. Circulation 1998, 98, 2453–2460. [Google Scholar] [CrossRef] [PubMed]
- Russo, B.; Menduni, M.; Borboni, P.; Picconi, F.; Frontoni, S. Autonomic Nervous System in Obesity and Insulin-Resistance—The Complex Interplay between Leptin and Central Nervous System. Int. J. Mol. Sci. 2021, 22, 5187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Aspect Measured | Parameter | Device | Method | Cut-Offs |
|---|---|---|---|---|
| Weight status | BMI | Electronic scale, stadiometer | A calibrated scale was used to measure the patient’s body weight in kilograms (kg). In order to minimize measurement errors, lightweight clothing and no shoes were worn. Height in centimeters (cm) was measured while the patient was standing erect with their back against a wall and heels together. The following formula was employed: BMI = Weight (kg)/(Height m2) | Underweight: BMI less than 18.5 Normal weight: BMI 18.5 to 24.9 Overweight: BMI 25 to 29.9 Obesity class 1: BMI 30 to 34.9 Obesity class 2: BMI 35 to 39.9 Obesity class 3: BMI 40 or greater |
| MetS | WC | Flexible measuring tape | The measuring tape was positioned around the waistline, horizontal and parallel to the floor. It was wrapped snugly around the waist without compressing the skin, and not over clothing. The measurement was taken in centimeters. | ≥94/≥80 cm for men/women |
| Blood pressure | Manual sphygmomanometer; stethoscope | At least two measurements taken, using the appropriate cuff size, after the patient rested in a seated position for at least 5 min. The results were expressed in mmHg. | ≥130/85 mm Hg | |
| Fasting plasma glucose | Automated analyzer | A fast of at least 8 h before the test. The blood sample was collected through venipuncture and labeled with the individual’s information, including name and date of birth, to ensure accurate identification. The sample was sent to the laboratory for analysis. The result was reported in milligrams per deciliter (mg/dL). | ≥100 mg/dL | |
| HDL Cholesterol | Blood was drawn after a minimum 8 h fast, and the sample was adequately labeled and sent to the laboratory. The result was reported in milligrams per deciliter (mg/dL). | <40/50 mg/dL for men/women | ||
| Serum Triglycerides | >150 mg/dL | |||
| Arterial stiffness | PWV, AiX | Arteriograph Tensiomed (Medexpert, Budapest). Software version 3.0.0.3 | Participants refrained from alcohol, caffeine, and smoking for at least 10 h before the examination. After 10 min of rest in a supine position, measurements were taken. During the assessment, patients were instructed to minimize movement and remain quiet to reduce interference. Appropriate cuff sizes, determined by individual arm circumference using a flexible measuring tape, were selected. Additionally, the distance from the jugular notch to the symphysis pubis was measured to estimate travel distance. Demographic data, including age, gender, height, weight, and smoking status, were recorded. An appropriately sized cuff, similar to a sphygmomanometer, was placed on the patient’s arm. The device then automatically inflated and gradually deflated the cuff while communicating with a laptop. This method records oscillometric pressure curves through plethysmography, capturing pressure changes in an upper arm artery. Pulsatile pressure fluctuations caused by the artery under the cuff result in periodic pressure changes. The Arteriograph calculates PWV and Aix by analyzing these changes, decomposing systolic and diastolic waves, and identifying wave onsets and peaks using its software. | Assessed as continuous variables |
| Atherosclerosis | CIMT | General Electric S8 ultrasound device, using a >7 MHz linear array transducer | High-resolution B-mode ultrasonography was conducted with minimal compression. CIMT assessments were made on arterial segments free of plaques, characterized by clear lumen–intima and media–adventitia interface. A straight 10 mm long segment of the far wall of the common carotid artery (CCA) was selected. The specific region of interest was expanded to a high-resolution 1.2 × 1.2 cm image. Longitudinal images of the carotid arteries were captured using the lateral probe position, which optimizes CIMT resolution. CIMT measurements were taken at a location situated at least 5 mm below the distal end of the CCA. | Assessed as continuous variable |
| Liver involvement | Platelet count, AST, and ALT for simple score calculation | Automated analyzer | Blood samples were collected after an overnight fast through venipuncture using appropriate collection tubes. | HIS, FIB4, APRI, AAR cut-offs described in text |
| E (kPa), CAP | Fibroscan 502 Touch | The patient undergoes a three-hour fasting period before the procedure and is positioned in a supine posture with the right arm abducted. The choice between the M and XL probe is determined based on the device’s prompt for optimal assessment. The method of 1D transient elastography provides a quantitative assessment of 1D elasticity within hepatic tissue, referred to as liver stiffness measurement (LSM) or E (measured in kPa). This method also enables the measurement of steatosis using the controlled attenuation parameter (CAP, measured in dB/m). It involves the generation of a mechanical pulse to estimate tissue stiffness along a fixed ultrasonographic line. The assessed tissue volume is approximately 1 cm × 4 cm. To ensure accuracy, ten measurements were taken, and the variability between these measurements was less than 30% of the mean stiffness value (interquartile range, IQR). | Assessed as continuous variables |
| Variable | Descriptive Parameter | Gender | p-Value | |
|---|---|---|---|---|
| Female | Male | |||
| AST (U/L) | Mean | 24.13 | 33.87 | 0.045 |
| StdDev | 13.18 | 36.72 | ||
| IQR | 9 | 14 | ||
| MIN | 12 | 10 | ||
| MAX | 82 | 217 | ||
| 95% CI | 20.17–28.09 | 20.16–47.58 | ||
| Platelets (109/L) | Mean | 280.07 | 252.9 | 0.044 |
| StdDev | 83.93 | 63.72 | ||
| IQR | 102 | 65.75 | ||
| MIN | 53 | 154 | ||
| MAX | 480 | 441 | ||
| 95% CI | 254.85–305.28 | 229.11–276.69 | ||
| APRI | Mean | 0.3440 | 0.4060 | <0.01 |
| StdDev | 0.4978 | 0.3673 | ||
| IQR | 0.12 | 0.2 | ||
| MIN | 0.08 | 0.07 | ||
| MAX | 3.16 | 2.06 | ||
| 95% CI | 0.1944–0.4936 | 0.2689–0.5431 | ||
| HDL-cholesterol | Mean | 65.2 | 54.93 | <0.01 |
| StdDev | 15.66 | 12.73 | ||
| IQR | 19.5 | 20.75 | ||
| MIN | 37 | 34 | ||
| MAX | 100 | 80 | ||
| 95% CI | 60.5 –69.9 | 50.18–59.69 | ||
| HSI | Mean | 40.99 | 37.10 | <0.01 |
| StdDev | 6.32 | 5.01 | ||
| IQR | 9.97 | 8.53 | ||
| MIN | 26.8 | 27.77 | ||
| MAX | 53.37 | 46.18 | ||
| 95% CI | 39.09–42.89 | 35.23–38.98 | ||
| Variable | Descriptive Parameter | MetS | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| Age | Mean | 50.92 | 66.81 | <0.01 |
| StdDev | 13.17 | 11.03 | ||
| IQR | 20 | 16 | ||
| MIN | 19 | 45 | ||
| MAX | 74 | 85 | ||
| 95% CI | 47.14–54.7 | 62.35–71.26 | ||
| BMI | Mean | 26.88 | 31.49 | <0.01 |
| StdDev | 3.99 | 5.05 | ||
| IQR | 5.2 | 7.83 | ||
| MIN | 20.8 | 24.2 | ||
| MAX | 40.6 | 42.7 | ||
| 95% CI | 25.73–28.02 | 29.45–33.53 | ||
| HDL-cholesterol | Mean | 65.3 | 53.15 | <0.01 |
| StdDev | 14.06 | 14.68 | ||
| IQR | 17.5 | 23 | ||
| MIN | 38 | 34 | ||
| MAX | 100 | 92 | ||
| 95% CI | 61.27–69.35 | 47.22–59.08 | ||
| Triglycerides | Mean | 105.63 | 152.04 | <0.01 |
| StdDev | 57.11 | 75.54 | ||
| IQR | 53 | 75.75 | ||
| MIN | 26 | 42 | ||
| MAX | 293 | 368 | ||
| 95% CI | 89.23–122.04 | 121.53–182.55 | ||
| HSI | Mean | 37.92 | 42.31 | <0.01 |
| StdDev | 5.99 | 5.32 | ||
| IQR | 9.33 | 7.34 | ||
| MIN | 26.8 | 31.3 | ||
| MAX | 51.3 | 53.37 | ||
| 95% CI | 36.19–39.64 | 40.16–44.46 | ||
| FIB-4 | Mean | 1 | 1.93 | <0.01 |
| StdDev | 0.73 | 2.23 | ||
| IQR | 0.5 | 1.1 | ||
| MIN | 0.22 | 0.42 | ||
| MAX | 4.4 | 11.49 | ||
| 95% CI | 0.79–1.21 | 1.02–2.83 | ||
| Agile 3+ | Mean | 0.128 | 0.4509 | <0.01 |
| StdDev | 0.1597 | 0.3194 | ||
| IQR | 0.1354 | 0.5699 | ||
| MIN | 0.0095 | 0.0382 | ||
| MAX | 0.9082 | 0.9915 | ||
| 95% CI | 0.0821–0.1738 | 0.3219–0.58 | ||
| Agile 4 | Mean | 0.0232 | 0.131 | <0.01 |
| StdDev | 0.0982 | 0.2283 | ||
| IQR | 0.0121 | 0.1641 | ||
| MIN | 0.0003 | 0.0003 | ||
| MAX | 0.6921 | 0.8459 | ||
| 95% CI | −0.005–0.0514 | 0.0388–0.2233 | ||
| CAP | Mean | 255.22 | 303.92 | <0.01 |
| StdDev | 51.18 | 49.56 | ||
| IQR | 81 | 52.5 | ||
| MIN | 140 | 153 | ||
| MAX | 361 | 381 | ||
| 95% CI | 240.52–269.93 | 283.9–323.94 | ||
| E(kPa) | Mean | 4.86 | 8.97 | <0.01 |
| StdDev | 1.96 | 5.96 | ||
| IQR | 1.5 | 5.83 | ||
| MIN | 2.4 | 2.1 | ||
| MAX | 15.6 | 27.7 | ||
| 95% CI | 4.29–5.42 | 6.57–11.37 | ||
| AoPWV | Mean | 8.87 | 9.73 | 0.029 |
| StdDev | 2.54 | 1.33 | ||
| IQR | 3.65 | 2.03 | ||
| MIN | 4.1 | 7.6 | ||
| MAX | 17.7 | 13.3 | ||
| 95% CI | 8.14–9.6 | 9.19–10.26 | ||
| AoAix | Mean | 29.12 | 38.78 | <0.01 |
| StdDev | 15.44 | 13.89 | ||
| IQR | 22.45 | 20.58 | ||
| MIN | −2.3 | 11.4 | ||
| MAX | 62.8 | 70.8 | ||
| 95% CI | 24.68–33.55 | 33.17–44.39 | ||
| CIMT | Mean | 0.74 | 1.05 | <0.01 |
| StdDev | 0.19 | 0.13 | ||
| IQR | 0.3 | 0.23 | ||
| MIN | 0.4 | 0.8 | ||
| MAX | 1.2 | 1.3 | ||
| 95% CI | 0.69–0.8 | 1–1.11 | ||
| Variable | Values | MetS | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| BMI category | Normal | 23 (46.9%) | 2 (7.7%) | <0.01 |
| Overweight | 15 (30.6%) | 9 (34.6%) | ||
| Obese (class 1) | 9 (18.4%) | 8 (30.8%) | ||
| Obese (class 2) | 1 (2%) | 5 (19.2%) | ||
| Obese (class 3) | 1 (2%) | 2 (7.7%) | ||
| APRI ≥ 0.5 | No | 47 (95.9%) | 20 (76.9%) | 0.018 |
| Yes | 2 (4.1%) | 6 (23.1%) | ||
| FIB-4 ≥ 1.3 | No | 43 (87.8%) | 13 (50%) | <0.01 |
| Yes | 6 (12.2%) | 13 (50%) | ||
| HSI > 36 | No | 19 (38.8%) | 4 (15.4%) | 0.037 |
| Yes | 30 (61.52%) | 22 (84.6%) | ||
| Variable | Characteristic | Cluster 1 | Cluster 2 | Cluster 3 | p-Value |
|---|---|---|---|---|---|
| Count | - | 28 (37.3%) | 13 (17.3%) | 34 (45.3%) | |
| CAP (dB/m) | Mean | 226.46 | 246.23 | 319.58 | <0.01 |
| StdDev | 39.33 | 36.57 | 39.33 | ||
| IQR | 58.25 | 33.5 | 45.25 | ||
| MIN | 140 | 198 | 271 | ||
| MAX | 300 | 336 | 381 | ||
| 95% CI | 211.21–241.71 | 224.13–268.33 | 309.81–326.37 | ||
| Predictor importance | 1 | ||||
| AoPWV | Mean | 7.38 | 12.23 | 9.46 | <0.01 |
| StdDev | 1.43 | 2.02 | 1.2 | ||
| IQR | 2.03 | 2.2 | 1.78 | ||
| MIN | 4.1 | 9.8 | 7.6 | ||
| MAX | 10.1 | 17.7 | 12 | ||
| 95% CI | 6.83–7.94 | 11–13.45 | 9.05–9.88 | ||
| Predictor importance | 0.88 | ||||
| Variable | Values | Cluster 1 | Cluster 2 | Cluster 3 | p-Value |
|---|---|---|---|---|---|
| MetS | No | 25 (89.3%) | 10 (76.9%) | 14 (41.2%) | <0.01 |
| Yes | 3 (10.7%) | 3 (23.1%) | 20 (58.8%) | ||
| HWC | No | 26 (92.9%) | 8 (61.5%) | 11 (32.4%) | <0.01 |
| Yes | 2 (7.1%) | 5 (38.5%) | 23 (67.6%) | ||
| IFG/T2DM | No | 19 (67.9%) | 7 (53.8%) | 8 (23.5%) | <0.01 |
| Yes | 9 (32.1%) | 6 (46.2%) | 26 (76.5%) | ||
| LHDL | No | 27 (96.4%) | 9 (69.2%) | 24 (70.6%) | 0.023 |
| Yes | 1 (3.6%) | 4 (30.8%) | 10 (29.4%) | ||
| HBP | No | 22 (78.6%) | 5 (38.5%) | 11 (32.4%) | <0.01 |
| Yes | 6 (21.4%) | 8 (61.5%) | 23 (67.6%) |
| Variable | Characteristic | Cluster 1 | Cluster 2 | Cluster 3 | p-Value |
|---|---|---|---|---|---|
| Triglycerides | Mean | 96.96 | 120.85 | 142.44 | <0.01 |
| StdDev | 55.42 | 60.28 | 73.33 | ||
| IQR | 46.75 | 45.5 | 59.25 | ||
| MIN | 26 | 65 | 42 | ||
| MAX | 293 | 292 | 368 | ||
| 95% CI | 75.48–118.45 | 84.42–157.27 | 116.85–168.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solomon, A.; Negrea, M.O.; Cipăian, C.R.; Boicean, A.; Mihaila, R.; Rezi, C.; Cristinescu, B.A.; Berghea-Neamtu, C.S.; Popa, M.L.; Teodoru, M.; et al. Interactions between Metabolic Syndrome, MASLD, and Arterial Stiffening: A Single-Center Cross-Sectional Study. Healthcare 2023, 11, 2696. https://doi.org/10.3390/healthcare11192696
Solomon A, Negrea MO, Cipăian CR, Boicean A, Mihaila R, Rezi C, Cristinescu BA, Berghea-Neamtu CS, Popa ML, Teodoru M, et al. Interactions between Metabolic Syndrome, MASLD, and Arterial Stiffening: A Single-Center Cross-Sectional Study. Healthcare. 2023; 11(19):2696. https://doi.org/10.3390/healthcare11192696
Chicago/Turabian StyleSolomon, Adelaida, Mihai Octavian Negrea, Călin Remus Cipăian, Adrian Boicean, Romeo Mihaila, Cristina Rezi, Bianca Andreea Cristinescu, Cristian Stefan Berghea-Neamtu, Mirela Livia Popa, Minodora Teodoru, and et al. 2023. "Interactions between Metabolic Syndrome, MASLD, and Arterial Stiffening: A Single-Center Cross-Sectional Study" Healthcare 11, no. 19: 2696. https://doi.org/10.3390/healthcare11192696