
Prevalence of Type 2 Diabetes, Impaired Fasting Glucose, and Diabetes Risk in an Adult and Older North-Eastern Portuguese Population

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Sample
2.2. Ethical Procedures
2.3. Data Collection
2.3.1. Anthropometric Measures
2.3.2. Age Groups
2.3.3. Diabetes Diagnosis and Fasting Glucose
2.3.4. Diabetes Risk
2.4. Statistical Analysis
3. Results
3.1. Prevalence of T2D
3.2. Prevalence of IFG
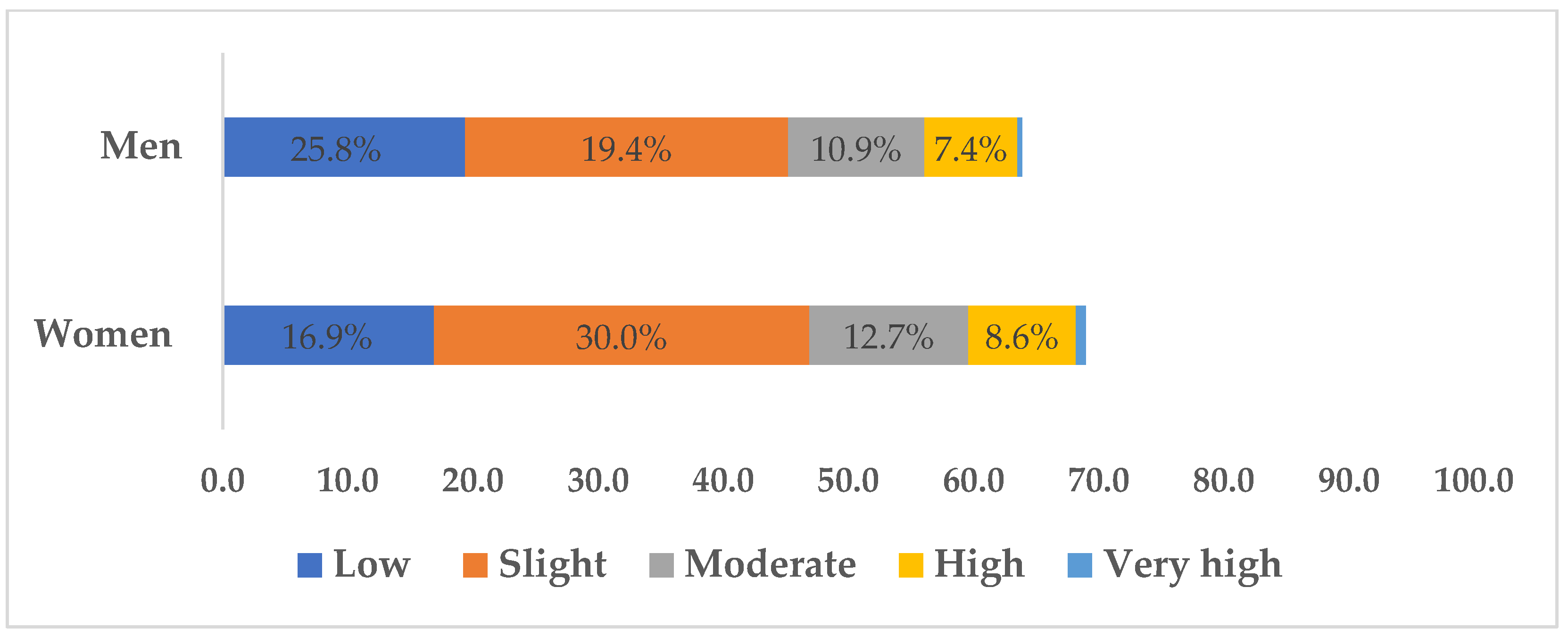
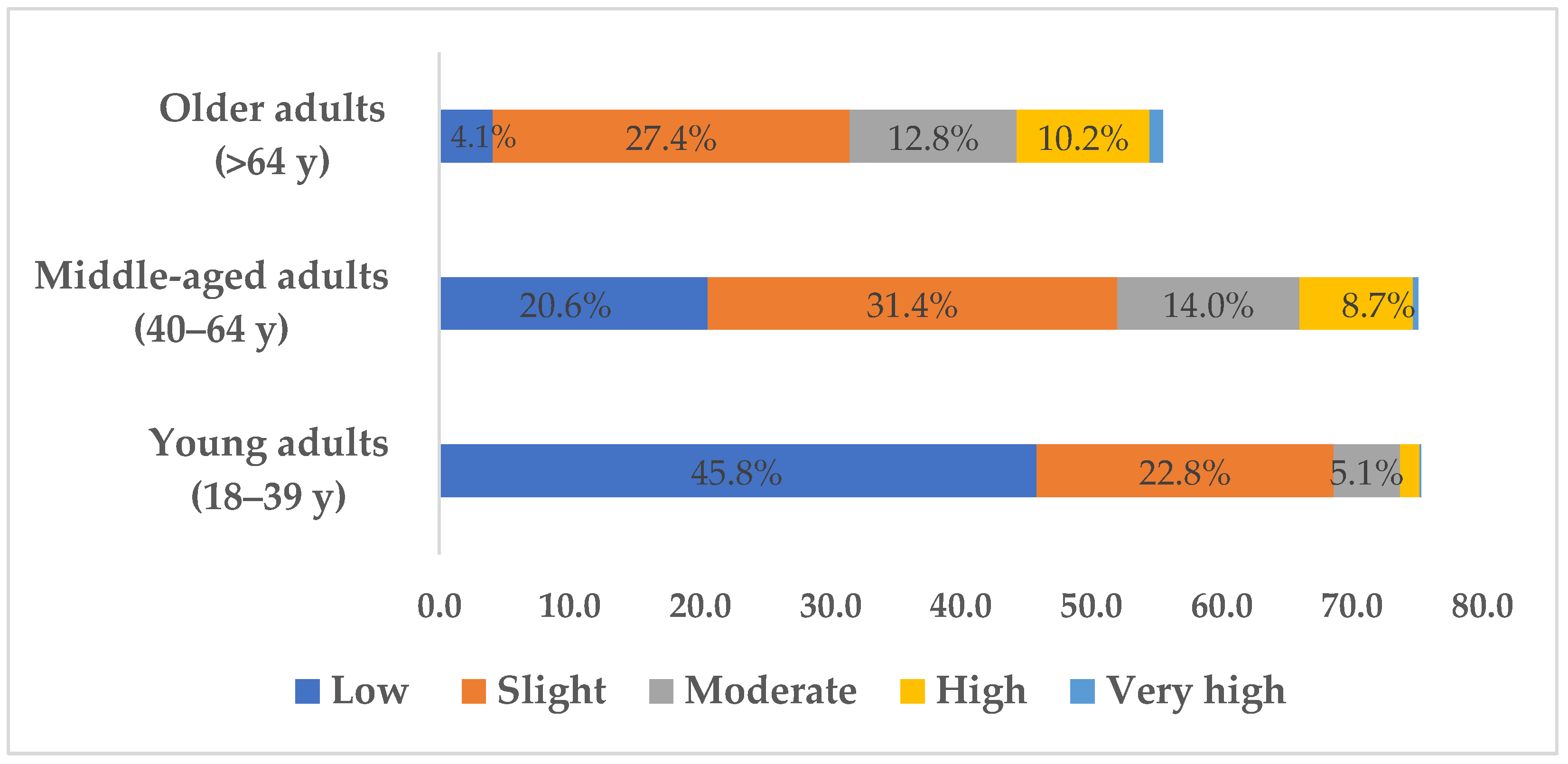
3.3. T2D Risk in Individuals without Diabetes
4. Discussion
4.1. Prevalence of T2D
4.2. Prevalence of IFG
4.3. Diabetes Risk in Individuals without Diabetes
4.4. Limitations, Practical Application, and Futures Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alexander, C.M.; Landsman, P.B.; Teutsch, S.M.; Haffner, S.M. NCEP-Defined Metabolic Syndrome, Diabetes, and Prevalence of Coronary Heart Disease Among NHANES III Participants Age 50 Years and Older. Diabetes 2003, 52, 1210–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The Growing Epidemic of Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Burgos-Morón, E.; Abad-Jiménez, Z.; Martínez de Marañón, A.; Iannantuoni, F.; Escribano-López, I.; López-Domènech, S.; Salom, C.; Jover, A.; Mora, V.; Roldan, I.; et al. Relationship between Oxidative Stress, ER Stress, and Inflammation in Type 2 Diabetes: The Battle Continues. J. Clin. Med. 2019, 8, 1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 Diabetes Mellitus. Nat. Rev. Dis. Primer 2015, 1, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The Diabetes Mellitus–Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef] [Green Version]
- Gothandam, K.; Ganesan, V.S.; Ayyasamy, T.; Ramalingam, S. Antioxidant Potential of Theaflavin Ameliorates the Activities of Key Enzymes of Glucose Metabolism in High Fat Diet and Streptozotocin—Induced Diabetic Rats. Redox Rep. 2019, 24, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Hudish, L.I.; Reusch, J.E.B.; Sussel, L. β Cell Dysfunction during Progression of Metabolic Syndrome to Type 2 Diabetes. J. Clin. Investig. 2019, 129, 4001–4008. [Google Scholar] [CrossRef] [Green Version]
- Prentki, M.; Nolan, C.J. Islet β Cell Failure in Type 2 Diabetes. J. Clin. Investig. 2006, 116, 1802–1812. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.M.Y.; Wellberg, E.A.; Kopp, J.L.; Johnson, J.D. Hyperinsulinemia in Obesity, Inflammation, and Cancer. Diabetes Metab. J. 2021, 45, 285–311. [Google Scholar] [CrossRef]
- Punthakee, Z.; Goldenberg, R.; Katz, P. Definition, Classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Can. J. Diabetes 2018, 42, S10–S15. [Google Scholar] [CrossRef] [Green Version]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A High-Risk State for Diabetes Development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuniss, N.; Freyer, M.; Müller, N.; Kielstein, V.; Müller, U.A. Expectations and Fear of Diabetes-Related Long-Term Complications in People with Type 2 Diabetes at Primary Care Level. Acta Diabetol. 2019, 56, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Muzurović, E.; Kraljević, I.; Solak, M.; Dragnić, S.; Mikhailidis, D.P. Homocysteine and Diabetes: Role in Macrovascular and Microvascular Complications. J. Diabetes Complicat. 2021, 35, 107834. [Google Scholar] [CrossRef]
- Sun, B.; Luo, Z.; Zhou, J. Comprehensive Elaboration of Glycemic Variability in Diabetic Macrovascular and Microvascular Complications. Cardiovasc. Diabetol. 2021, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, Z. Prediabetes: Definition, Diagnostic Criteria and Management. J. Diabetes Nursin 2018, 22, 4. [Google Scholar]
- American Diabetes Association Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 33 (Suppl. S1), S62–S69. [CrossRef] [Green Version]
- Djelmis, J.; Pavić, M.; Mulliqi Kotori, V.; Pavlić Renar, I.; Ivanisevic, M.; Oreskovic, S. Prevalence of Gestational Diabetes Mellitus According to IADPSG and NICE Criteria. Int. J. Gynecol. Obstet. 2016, 135, 250–254. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consultation Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation. Part 1, Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999.
- World Health Organization. International Diabetes Federation Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of a WHO/IDF Consultation; World Health Organization: Geneva, Switzerland, 2006.
- Shaw, J.E.; Sicree, R.A.; Zimmet, P.Z. Global Estimates of the Prevalence of Diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2010, 87, 4–14. [Google Scholar] [CrossRef]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of Cardiovascular Disease in Type 2 Diabetes: A Systematic Literature Review of Scientific Evidence from across the World in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.-F. Global, Regional, and National Burden and Trend of Diabetes in 195 Countries and Territories: An Analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef]
- Raposo, J.F. Diabetes: Factos e números 2016, 2017 e 2018. Rev. Port. Diabetes 2020, 15, 19–27. [Google Scholar]
- Barreto, M.; Kislaya, I.; Gaio, V.; Rodrigues, A.P.; Santos, A.J.; Namorado, S.; Antunes, L.; Gil, A.P.; Boavida, J.M.; Silva, A.C.; et al. Prevalence, awareness and control of diabetes in Portugal: Results from the first National Health Examination Survey. Diabetes Res. Clin. Pract. 2018, 5, 271–278. [Google Scholar] [CrossRef] [PubMed]
- De Sousa-Uva, M.; Antunes, L.; Nunes, B.; Rodrigues, A.P.; Simões, J.A.; Ribeiro, R.T.; Boavida, J.M.; Matias-Dias, C. Trends in Diabetes Incidence from 1992 to 2015 and Projections for 2024: A Portuguese General Practitioner’s Network Study. Prim. Care Diabetes 2016, 10, 329–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, J.E.; Bragada, J.A.; Bragada, J.P.; Coelho, J.P.; Pinto, I.G.; Reis, L.P.; Fernandes, P.O.; Morais, J.E.; Magalhães, P.M. Structural Equation Modelling for Predicting the Relative Contribution of Each Component in the Metabolic Syndrome Status Change. Int. J. Environ. Res. Public Health 2022, 19, 3384. [Google Scholar] [CrossRef]
- Teixeira, J.; Bragada, J.; Bragada, J.; Coelho, J.; Pinto, I.; Reis, L.; Magalhaes, P. The Prevalence of Metabolic Syndrome and Its Components in Bragança District, North-Eastern Portugal: A Retrospective Observational Cross-Sectional Study. Rev. Port. Endocrinol. Diabetes E Metab. 2022, 17, 51–57. [Google Scholar] [CrossRef]
- Resnik, D.B. Trust as a Foundation for Research with Human Subjects. In The Ethics of Research with Human Subjects: Protecting People, Advancing Science, Promoting Trust; Resnik, D.B., Ed.; International Library of Ethics, Law, and the New Medicine; Springer International Publishing: Cham, Switzerland, 2018; pp. 87–111. ISBN 978-3-319-68756-8. [Google Scholar]
- Sagun, G.; Oguz, A.; Karagoz, E.; Filizer, A.T.; Tamer, G.; Mesci, B. Application of Alternative Anthropometric Measurements to Predict Metabolic Syndrome. Clinics 2014, 69, 347–353. [Google Scholar] [CrossRef]
- Tsigos, C.; Hainer, V.; Basdevant, A.; Finer, N.; Fried, M.; Mathus-Vliegen, E.; Micic, D.; Maislos, M.; Roman, G.; Schutz, Y.; et al. Management of Obesity in Adults: European Clinical Practice Guidelines. Obes. Facts 2008, 1, 106–116. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD: The Task Force for Diabetes, Pre-Diabetes, and Cardiovascular Diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Cho, N.H.; Colagiuri, S.; Distiller, L.; Dong, B.; Dunning, T.; Gadsby, R.; Goel, A.; Munshi, M.; Sinclair, A.; Sinay, I. Managing Older People with Type 2 Diabetes; International Diabetes Federation: Brussels, Belgium, 2013; ISBN 978-2-930229-86-7. [Google Scholar]
- Haeckel, R.; Wosniok, W. The Importance of Correct Stratifications When Comparing Directly and Indirectly Estimated Reference Intervals. Clin. Chem. Lab. Med. 2021, 59, 1628–1633. [Google Scholar] [CrossRef]
- Lindström, J.; Tuomilehto, J. The Diabetes Risk Score: A Practical Tool to Predict Type 2 Diabetes Risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Vandersmissen, G.J.M.; Godderis, L. Evaluation of the Finnish Diabetes Risk Score (FINDRISC) for Diabetes Screening in Occupational Health Care. Int. J. Occup. Med. Environ. Health 2015, 28, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Horta, M.R.; Santos, R.; Mendes, Z.; Jacinto, I.; Guerreiro, J.; Cary, M.; Miranda, A.; Helling, D.K.; Martins, A.P. Diabetes Policies and Pharmacy-Based Diabetes Interventions in Portugal: A Comprehensive Review. J. Pharm. Policy Pract. 2019, 12, 5. [Google Scholar] [CrossRef] [Green Version]
- Bland, M. An Introduction to Medical Statistics, 3rd ed.; Oxford University Press: New York, NY, USA, 2000; ISBN 978-0-19-263269-2. [Google Scholar]
- Cohen, J. A Power Primer. In Methodological Issues and Strategies in Clinical Research, 4th ed.; American Psychological Association: Washington, DC, USA, 2016; p. 284. ISBN 978-1-4338-2091-5. [Google Scholar]
- Agresti, A. An Introduction to Categorical Data Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2018; ISBN 978-1-119-40526-9. [Google Scholar]
- Stewart, A. Basic Statistics and Epidemiology: A Practical Guide; CRC Press: Boca Raton, FL, USA, 2022; ISBN 978-1-00-050637-2. [Google Scholar]
- Censos 2021 (Prodata®), O Que Mudou No Seu Munícipio Em 10 Anos? Available online: https://www.pordata.pt/censos/resultados/emdestaque-braganca-446 (accessed on 27 May 2023).
- Gardete-Correia, L.; Boavida, J.M.; Raposo, J.F.; Mesquita, A.C.; Fona, C.; Carvalho, R.; Massano-Cardoso, S. First Diabetes Prevalence Study in Portugal: PREVADIAB Study. Diabet. Med. 2010, 27, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Geer, E.B.; Shen, W. Gender Differences in Insulin Resistance, Body Composition, and Energy Balance. Gend. Med. 2009, 6, 60–75. [Google Scholar] [CrossRef] [Green Version]
- Atlas, D. International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2006; Volume 2, p. 33. ISBN 2-930229-27-6. [Google Scholar]
- Palmer, A.K.; Gustafson, B.; Kirkland, J.L.; Smith, U. Cellular Senescence: At the Nexus between Ageing and Diabetes. Diabetologia 2019, 62, 1835–1841. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, H.N.; Hardman, M.J. Wound Senescence: A Functional Link between Diabetes and Ageing? Exp. Dermatol. 2021, 30, 68–73. [Google Scholar] [CrossRef]
- Tremblay, J.; Hamet, P. Environmental and Genetic Contributions to Diabetes. Metabolism 2019, 100, 153952. [Google Scholar] [CrossRef]
- Ahmad, O.B.; Boschi Pinto, C.; Lopez, A.; Murray, C.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New WHO Standard; World Health Organization: Geneva, Switzerland, 2001; Volume 9, pp. 1–14.
- Savić, S.; Stanivuković, S.; Lakić, B. Ten-Year Risk Assessment for Type 2 Diabetes Mellitus Using the Finnish Diabetes Risk Score in Family Medicine. Med. Glas. 2020, 17, 517–522. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measures | Women (n = 3865) | Men (n = 2705) | Total (n = 6570) |
|---|---|---|---|
| Age (y) | 57.4 ± 18.1 | 60.0 ± 16.8 | 58.4 ± 17.6 |
| Height (cm) | 170.0 ± 7.2 | 158.7 ± 6.7 | 163.3 ± 8.9 |
| Weight (kg) | 68.7 ± 13.9 | 80.5 ± 13.5 | 73.6 ± 14.9 |
| BMI (kg/m2) | 27.3 ± 5.3 | 27.8 ± 4.1 | 27.5 ± 4.9 |
| WC (cm) | 92.0 ± 13.3 | 99.6 ± 11.1 | 95.2 ± 13.0 |
| Variables | Group Analysis | Diagnosis | n (%) | 95% CI (Min–Max) |
|---|---|---|---|---|
| Sex | Women | With T2D | 542 (14.0) | (13.0–15.2) |
| Without T2D | 3323 (86.0) | (84.8–87.1) | ||
| Total | 3865 (100.0) | – | ||
| Men | With T2D | 600 (22.2) | (20.6–23.8) | |
| Without T2D | 2105 (77.7) | (76.2–79.4) | ||
| Total | 2705 (100.0) | – | ||
| Age group | Young adults (18–39 y) | With T2D | 13 (1.2) | (0.64–2.0) |
| Without T2D | 1093 (98.8) | (98.2–99.5) | ||
| Total | 1106 (100.0) | – | ||
| Middle-aged adults (40–64 y) | With T2D | 319 (11.9) | (10.6–13.1) | |
| Without T2D | 2369 (88.1) | (86.9–89.4) | ||
| Total | 2688 (100.0) | – | ||
| Older adults (>64 y) | With T2D | 810 (29.2) | (27.5–30.9) | |
| Without T2D | 1966 (70.8) | (69.1–72.5) | ||
| Total | 2776 (100.0) | – | ||
| Population | Overall | With T2D | 1142 (17.4) | (16.5–18.3) |
| Without T2D | 5425 (82.6) | (81.6–83.5) | ||
| Total | 6570 (100.0) | – |
| Variables | Group Analysis | Diagnosis | n (%) | 95% CI (Min–Max) |
|---|---|---|---|---|
| Sex | Women | IFG | 326 (8.4) | (7.6–9.4) |
| Normal FG | 3539 (91.6) | (90.6–92.4) | ||
| Total | 3865 (100.0) | – | ||
| Men | IFG | 382 (14.1) | (12.8–15.5) | |
| Normal FG | 2323 (85.9) | (84.5–87.2) | ||
| Total | 2705 (100.0) | – | ||
| Age group | Young adults (18–39 y) | IFG | 16 (1.4) | (0.8–2.3) |
| Normal FG | 1090 (98.6) | (97.7–99.2) | ||
| Total | 1106 (100.0) | – | ||
| Middle-aged adults (40–64 y) | IFG | 255 (9.5) | (32.9–36.4) | |
| Normal FG | 2433 (90.5) | (89.3–91.6) | ||
| Total | 2688 (100.0) | – | ||
| Older adults (>64 y) | IFG | 437 (15.7) | (14.4–17.2) | |
| Normal FG | 2339 (84.3) | (82.9–85.6) | ||
| Total | 2776 (100.0) | – | ||
| Population | Overall | IFG | 708 (10.8) | (10.0–11.6) |
| Normal FG | 5862 (89.2) | (88.5–90.0) | ||
| Total | 6570 (100.0) | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magalhães, P.M.; Teixeira, J.E.; Bragada, J.P.; Duarte, C.M.; Bragada, J.A. Prevalence of Type 2 Diabetes, Impaired Fasting Glucose, and Diabetes Risk in an Adult and Older North-Eastern Portuguese Population. Healthcare 2023, 11, 1712. https://doi.org/10.3390/healthcare11121712
Magalhães PM, Teixeira JE, Bragada JP, Duarte CM, Bragada JA. Prevalence of Type 2 Diabetes, Impaired Fasting Glucose, and Diabetes Risk in an Adult and Older North-Eastern Portuguese Population. Healthcare. 2023; 11(12):1712. https://doi.org/10.3390/healthcare11121712
Chicago/Turabian StyleMagalhães, Pedro M., José E. Teixeira, João P. Bragada, Carlos M. Duarte, and José A. Bragada. 2023. "Prevalence of Type 2 Diabetes, Impaired Fasting Glucose, and Diabetes Risk in an Adult and Older North-Eastern Portuguese Population" Healthcare 11, no. 12: 1712. https://doi.org/10.3390/healthcare11121712